
Abstract
Objectives
To understand behaviors and attitudes of adults with diabetes who read their clinicians’ visit notes.
Methods
By linking a large 2017 patient survey involving three institutions with administrative and portal use data, we identified patients with diabetes mellitus from outpatient records and examined reading behaviors related to eligible notes—initial, follow-up, history and physical, and progress notes. We analyzed patients’ perceived benefits of reading notes.
Results
2104 respondents had diagnoses of diabetes mellitus and had read ≥1 note in the 12-month period. Patients had an average of 8.7 eligible notes available and read 59% of them. The strongest predictor of reading more notes was having more notes available; the specialties of the authoring clinicians were not correlated with note reading rates. Patients reported understanding notes by primary care clinicians and specialists equally well; more than 90% of patients reported understanding everything or almost everything in a self-selected note. Across visit types, 73–80% of patients reported that note reading was extremely important for taking care of their health.
Discussion
People with diabetes want to read their clinicians’ notes, are accessing them at high rates, and report understanding the notes and benefiting from reading them.
Introduction
Diabetes is a chronic illness that requires attentive daily self-care and systematic follow-up, making effective partnership between people with diabetes (PWDs) and their clinicians an essential component of effective care. 1 Most patients now have online access to their medical records via patient portals, and studies have shown that PWDs are active portal users and that portal use may be associated with better outcomes.2,3 In recent years, more portals have included clinicians’ notes in the information available to patients. 4 Nearly all patients who read their notes report many benefits from doing so.5–8 A study of PWDs seen in primary care offices found they were even more likely than patients without diabetes diagnoses to report benefits related to feeling in control, following medication regimens, and practicing better self-care. 9
Because diabetes can be correlated with other medical problems, PWDs may see specialist providers for screening or treatment in addition to or in lieu of their primary care providers (PCPs). Reading visit notes can help patients to coordinate care as well as to process and interpret information from multiple clinicians. PWDs may have different preferences regarding reading open visit notes written by primary care versus specialty clinicians. Understanding patients’ note reading preferences and behaviors may help to guide use of the visit notes as tools for diabetes self-management.
We examined note-reading behaviors and attitudes of adults with diabetes mellitus over a 12-month period. We hypothesized that they would read a higher proportion of their specialists’ visit notes than their primary care notes, that they would view specialist notes as more helpful, and that they would report understanding both primary care and specialty notes equally.
Methods
Setting
Participants were respondents to a large online survey conducted by OpenNotes between June and October 2017 in three health care systems: Beth Israel Deaconess Medical Center (BIDMC), a teaching hospital affiliated with Harvard Medical School in Boston, MA; Geisinger, a regional health system in Pennsylvania; and University of Washington Medicine (UW), an academic health system that includes four community-based hospitals in Seattle, WA. 10 All three systems began opening notes to primary care patients in 2010, and by 2014 they had expanded the practice to nearly all outpatient offices and clinicians such that patients were independently reading notes by specialists as well as primary care clinicians. Patients aged 18 years or older who had read at least one ambulatory outpatient visit note on the patient portal within the prior 12 months were invited to participate. We obtained socio-demographics, ambulatory note counts, and diagnosis codes from electronic administrative data. Details about the survey were published previously.10,11
Analytic sample
Patients in our analytic sample had opened at least one note in the 12 months prior to the survey according to portal tracking data, and they reported in the survey that they had read at least one note. We used ICD-10 codes E08-E11 and E13 to identify patients with diabetes mellitus. 12 We restricted eligible note types to initial, progress, follow-up, and history and physical exam notes; we excluded patients whose total number of eligible notes available during the study year were above the 99th percentile (39 notes) of the total note count.
Measurements
Our dependent measures were note reading rate, number of notes read, and the benefit score. We used note reading rate and number of notes read to measure patients’ reading behavior, and we used the benefit score to measure patient-reported benefits of reading their notes. Each patient's note reading rate was calculated as the number of notes read divided by number of total available notes, where number of notes read and number of total available notes were aggregated from date-stamped notes read and all available visit notes in the administrative notes data. Note reading benefits items included six survey questions (two of them available at UW only) addressing potential benefits on an 11-point scale, with each benefit item ranging from 0 (not at all important) to 10 (extremely important). We classified responses of 0–7 as “not important” or “less important” and responses of 8–10 as “extremely important.” Using a validated approach, we calculated the benefit score by averaging the four 11-point survey items that were asked at all three health systems. 13
Our primary independent variable was each note's visit type, derived from the specialty of the authoring clinician in administrative data: (1) visits to PCPs, (2) visits to clinicians in specialties that address diabetes or common complications of diabetes, and (3) visits to other clinicians (Supplemental Table 1).
We aggregated each patient's eligible visits during the study year and assigned the patient to one of seven mutually exclusive groups reflecting the visits they made: (1) PCP visits only, (2) diabetes-related specialist visits only, (3) other specialist visits only, (4) PCP and diabetes-related specialist visits, (5) PCP and other specialist visits, (6) diabetes-related and other specialist visits, and (7) all three types of visits (Supplemental Tables 2 and 3). We assigned patients who had only PCP visits as the reference group.
Additionally, in the survey, patients were asked to refer to a single self-selected note they had read and report what type of specialist wrote the note and how much of the note they understood (response options: very little, some, almost everything, everything). Other measures included total number of ambulatory visit notes and socio-demographics including age, gender, race, ethnicity, education, employment status, and health condition.
Statistical analysis
We calculated the mean and standard deviation of total number of available notes according to patients’ sociodemographic characteristics. We used univariate ANOVA analysis to test the differences between groups and notes reading rates across each of the characteristics. We used Chi-square tests for trend (1df) to test for trend in benefits according to number of notes read and according to age group of respondents. Unadjusted linear regression was used to test for trend in benefits score according to age groups. We used multivariate ordinary least squares regression models to estimate the associations between note reading behavior (note reading rate and number of notes read) and type of specialty visits. All models were adjusted for self-reported age, gender, race, ethnicity, education, employment, and health status; the model for number of notes read also adjusted for the total number of available notes. We used the Chi-square test for independence to compare each benefit measures (binary measure) across type of specialty visits, we also conducted one-way ANOVA to investigate the difference in the aggregated benefit score across type of specialty visits. We completed all analysis using SAS software version 9.4 (SAS Institute Inc., Cary, N.C.).
Results
Of 136,815 patients who received the survey, 21.7% responded. 10 Among the 28,782 patients across the three institutions who responded, 2440 had a diagnosis of diabetes mellitus in the EHR and had read at least one note (Supplemental Figure). Of these, 2104 patients had one or more eligible visit notes available and were included in this study.
Nearly half of participants were aged 65 or older and 51% were men (Table 1). Overall, the 2104 patients with diabetes had an average of 8.7 eligible notes available (range 1–39) during the previous year and had read 59% of those notes. There were no differences in note reading rates according to age and sex. Education was associated with note reading; for example, patients with no more than a high school education read 53% of available notes compared with 63% of patients who had graduate degrees.
Characteristics of patients with diabetes according to the mean number of eligible ambulatory visit notes a available in 12 months and mean note reading rate (N = 2104).
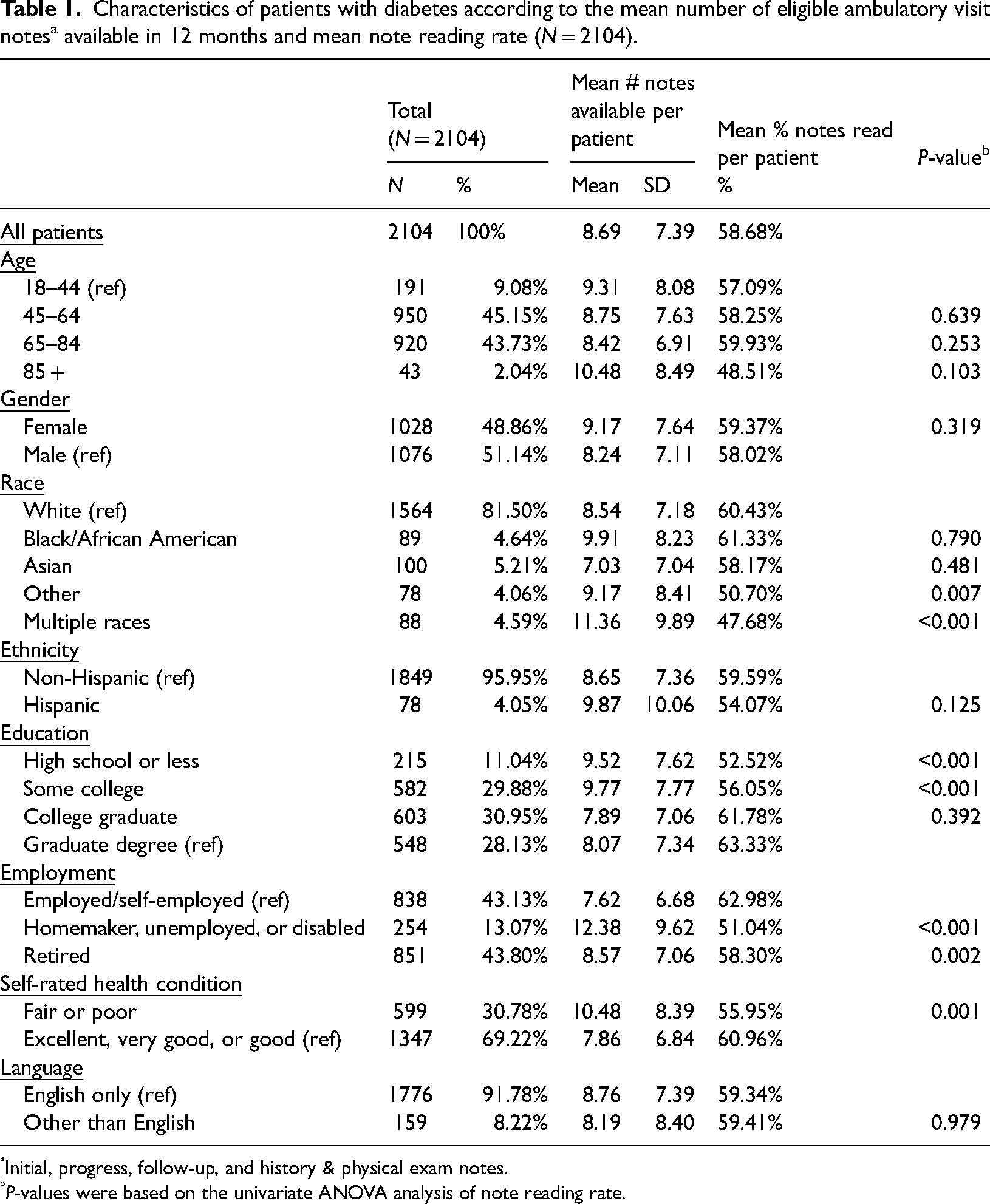
Initial, progress, follow-up, and history & physical exam notes.
P-values were based on the univariate ANOVA analysis of note reading rate.
On average, patients who saw all three types of providers had the greatest number of notes available (14.5) and, despite reading the greatest number of notes (6.7), had the lowest reading rate (49%) (Supplemental Table 2). Patients who had seen only diabetes-related specialists had the fewest notes (4.1) and the highest note reading rate (73%), but their reading rate was not significantly different from that of patients who had seen only a PCP (69%, the next highest reading rate). Adjusted for sociodemographic and health characteristics, all other groups had significantly lower reading rates than the PCP-visit-only group (Supplemental Table 3).
The strongest independent predictor of number of notes read in the past year was the total number of notes available, regardless of type of provider visits (data not shown). In other words, among these patients with diabetes across three institutions who had read at least one note, the more notes they had available to them, the more notes they read.
In general, patients reported the importance of many benefits to note reading, regardless of the type of providers they had seen during the previous year (Table 2). The highest proportions of patients (73–80%) across provider types reported that note reading was extremely important for taking care of their health. The least endorsed benefit—importance of note reading for preparing for office visits—was still endorsed by more than half of patients across groups (50–63%). The average overall score in the 0–10 importance of benefits ratings was 7.9, and although statistically significant differences were observed between groups, the range of the average scores across groups was very limited, from 7.7 to 8.3.
Proportion of 2104 patients with diabetes reporting extreme importance of benefits of reading notes (score 8–10 out of 10), according to type of visit notes available in the past year.
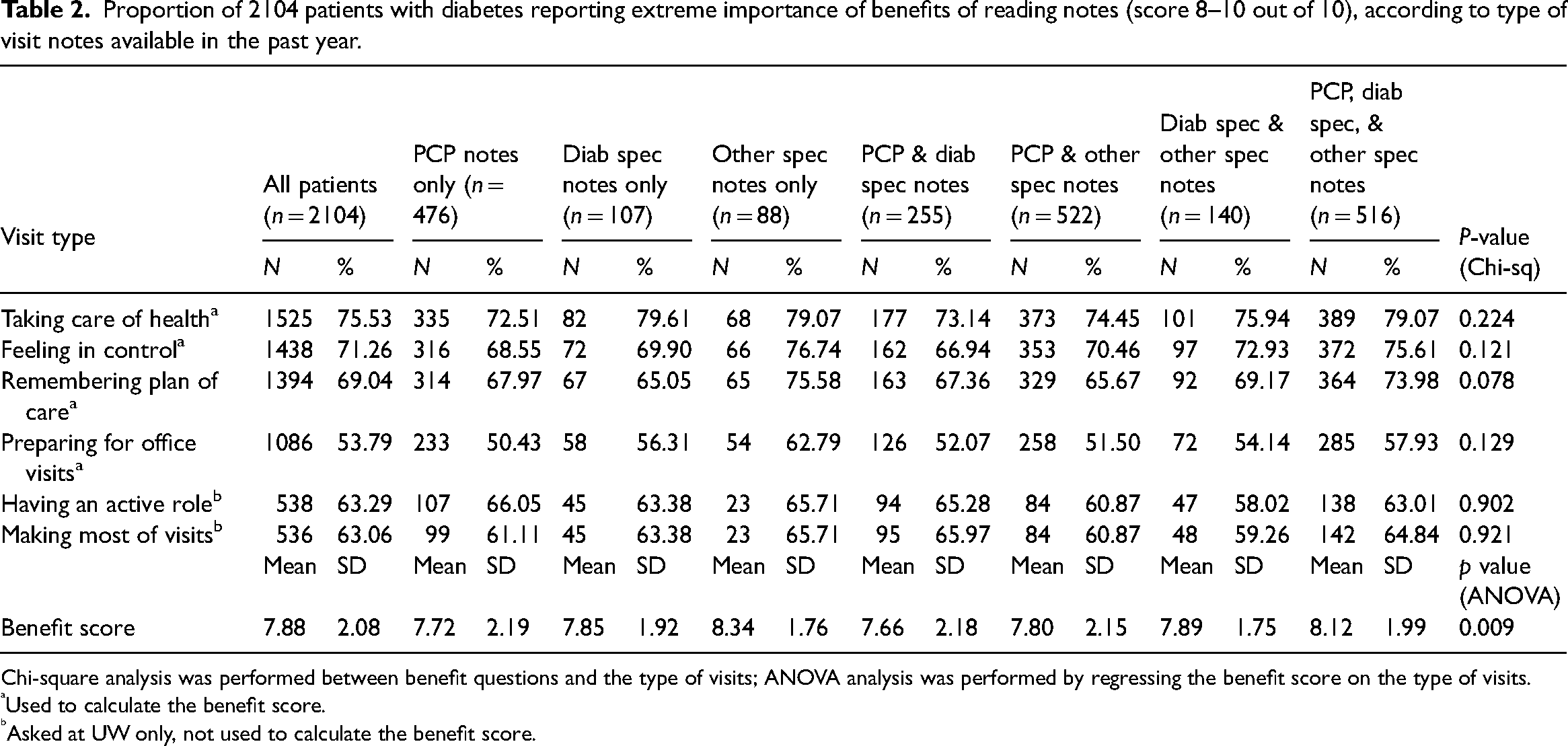
Chi-square analysis was performed between benefit questions and the type of visits; ANOVA analysis was performed by regressing the benefit score on the type of visits.
Used to calculate the benefit score.
Asked at UW only, not used to calculate the benefit score.
Ratings of importance of the benefits of note reading varied somewhat according to the total number of notes read, with the greater number of notes read associated with higher benefits ratings (Table 3). For example, 73% of patients who read one note rated note reading as extremely important for taking care of their health, compared with 81% of patients who read seven or more notes. Similarly, lower proportions of patients rated note reading as important for preparing for office visits, though at least half of patients, according to numbers of notes read, rated note reading as extremely important for this purpose. We repeated this analysis, grouping patients according to their proportions of notes read, and observed similar patterns with higher rates of note reading associated with higher ratings of benefits, though the gradients across groups were not as strong (data not shown). Differences were observed in the individual perceived benefits and in the overall benefit score according to age, with older patients reporting somewhat lower benefit ratings though the mean scores, in general, were over 7.0 out of 10 in most items (Table 4).
Proportion of 2104 patients with diabetes reporting extreme importance of benefits of reading notes (score 8–10 out of 10), according to quartiles of notes read in the past year.
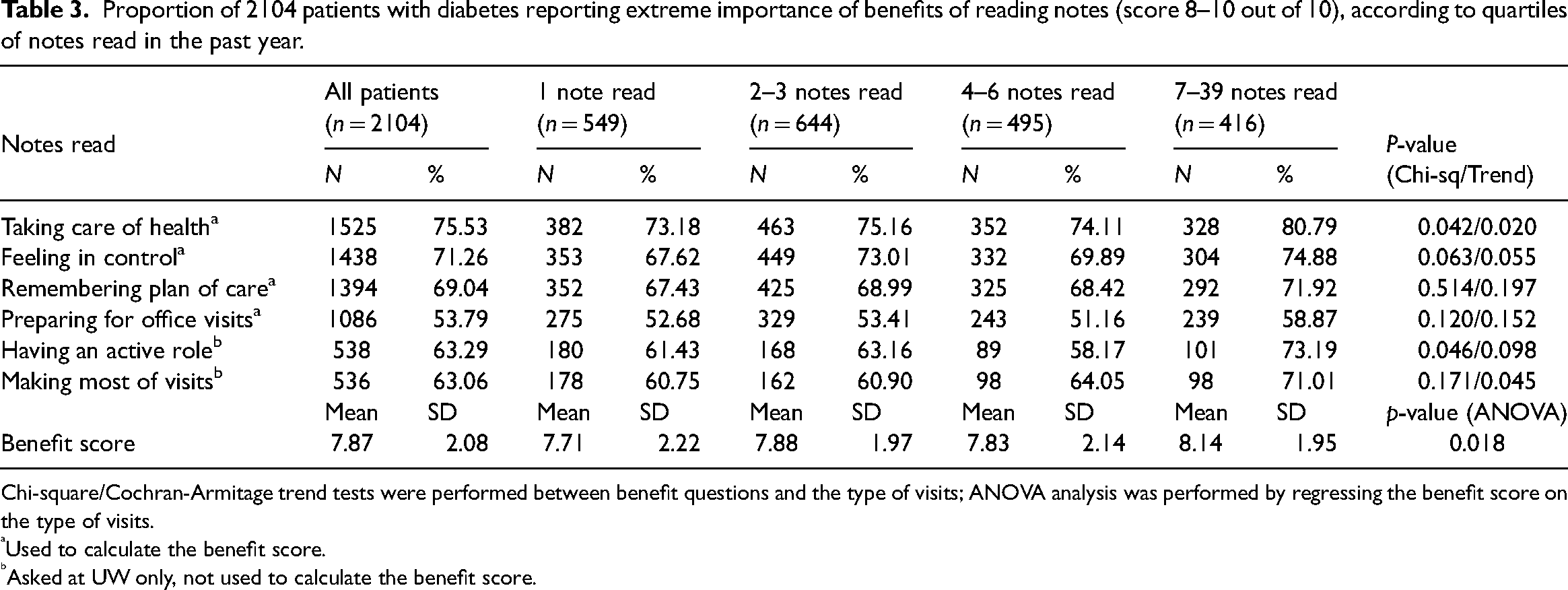
Chi-square/Cochran-Armitage trend tests were performed between benefit questions and the type of visits; ANOVA analysis was performed by regressing the benefit score on the type of visits.
Used to calculate the benefit score.
Asked at UW only, not used to calculate the benefit score.
Proportion of 2104 patients with diabetes reporting extreme importance of benefits of reading notes (score 8–10 out of 10), according to age categories.
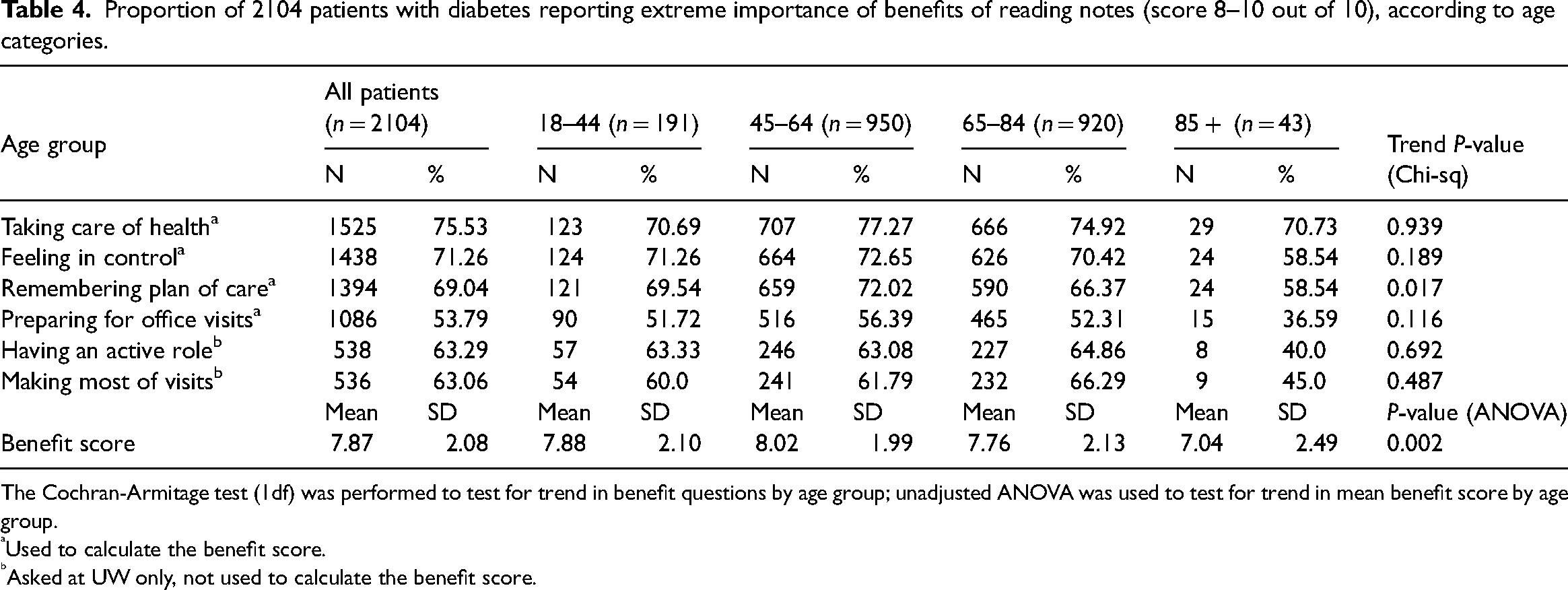
The Cochran-Armitage test (1df) was performed to test for trend in benefit questions by age group; unadjusted ANOVA was used to test for trend in mean benefit score by age group.
Used to calculate the benefit score.
Asked at UW only, not used to calculate the benefit score.
Patients were asked to answer questions about a specific note they remembered reading, and to rate their level of understanding of the note. More than 90% of patients reported they understood everything or almost everything in the note. When grouped according to type of provider, 97% reported understanding everything or almost everything in the note from a PCP visit, versus 94% who reported on a diabetes specialist note, and 91% of a note by another specialist (Chi-square test for overall differences, p = 0.005, data not shown).
Discussion
This is among the first studies to examine behaviors related to reading ambulatory visit notes among patients with diabetes. In 12 months, patients had an average of 8.7 initial, follow-up, history and physical, and progress notes and read 59% of them. The number of notes available was the strongest predictor of how many notes they read, thus disproving our hypothesis that the specialty of the authoring clinician would be the driving factor. Patient-reported benefit scores were not significantly different among patients who saw different types of providers, counter to our hypothesis that they would find greater benefits in reading specialty notes. Over 90% of patients reported understanding everything or almost everything in a self-selected note, regardless of author, thus supporting our hypothesis that PWD would understand notes by their primary and specialty care clinicians equally well.
Because effective diabetes care relies on effective self-management, patients’ access to information in their EHRs is an important component of care. A recent review suggests that PWDs achieve better glycemic control and lower blood pressure when they use patient portals, 3 including messaging 14 and medication refill functions 15 as well as general portal use. 16 However, only 3 of the 12 studies involved portals with access to visit notes and none studied the impact of note reading. Visit notes offer a level of detail about clinicians’ assessments and treatment plans not found in other sections of the EHR and note reading may be an important enhancement of portal-supported diabetes self-management. Under provisions of the 21st Century Cures Act, nearly all notes are available electronically to patients. 17 The association of note reading with clinical outcomes such as glycemic control, blood pressure, and cholesterol level is yet to be determined.
In provider-rich environments such as those in our study, a variety of specialists and non-specialists may be overseeing and directing diabetes care. But there is substantial geographic variation in access to diabetes specialists across the United States, and patients in non-urban and lower income areas may receive a larger proportion of their care from primary care clinicians.18–21 Nonetheless, we have no reason to believe that patients in other locations would perceive less value in note reading. PWDs in our study valued notes regardless of whether written by primary care or specialty clinicians.
Both primary care and specialty providers need to encourage PWDs to read their notes and to more consistently tailor notes to patients’ literacy levels, combining mindful writing with elements of technology-supported translation to other languages and various reading levels.22,23 Though notes by specialists may be more technical and challenging to read, patients are still reading them, and report that they understand and value reading them.24,25 Patients should also be notified of availability of notes; evidence shows that reading behaviors decline if notifications are stopped. 26
New technical developments may further encourage patient engagement. We have no doubt that easy portal access to visit notes, medication information, and laboratory results, as well as many free-standing computer applications (apps), improve the support and monitoring that are central for diabetes self-management. Beginning in 2023, the 21st Century Cures Act will require standardized APIs that will enable patients to download their health records using apps of their choice, likely causing a major shift in the tools that can help patients make sense of and optimize the extraordinary amount of information in their EHRs and other sources. 27 New apps may offer new functionalities, including patient-friendly ways to organize and visualize individuals’ health information.
Limitations
This study has important limitations that may limit its generalizability. Patients received care in three regional systems and the majority were white, well educated, and reported being in relatively good health. We did not have access to clinical measures such as A1c values and could not assess whether severity was associated with perceived benefit. The results may not be generalizable to areas where patients with diabetes see a different mix of providers, or fewer specialists, or obtain most diabetes-related care from a PCP. The response rate was low, though not out of line with other large surveys, and more engaged note users may have been more likely to respond. 28 We created service types for analysis, but we had no way to know whether visits included in the analysis addressed primary care, diabetes, comorbid conditions, or issues unrelated to diabetes. Self-selected notes may not be representative of all notes read, but these patterns mirror results from the larger survey showing patients across institutions and specialties and provider types generally report very high levels of understanding of notes they read. 11
Conclusions
PWD want to read their notes, are accessing them at high rates regardless of author specialty and visit type, and report understanding the notes and benefiting from reading them. These are reassuring findings given the intensity of self-management required in diabetes. Clinicians can encourage further engagement by enhancing the readability of notes and discussing the availability of notes with patients.
Supplemental Material
sj-docx-1-chi-10.1177_17423953231171890 - Supplemental material for People with diabetes who read their clinicians’ visit notes: Behaviors and attitudes
Supplemental material, sj-docx-1-chi-10.1177_17423953231171890 for People with diabetes who read their clinicians’ visit notes: Behaviors and attitudes by Zhiyong Dong, Suzanne Leveille, Dana Lewis and Jan Walker in Chronic Illness
Footnotes
Contributorship
Zhiyong Dong and Jan Walker researched literature and conceived the study. Zhiyong Dong, Jan Walker and Suzanne Leveille were involved in data access and data analysis. Dana Lewis provided a perspective as a patient author and provided important insights to the discussion. All authors drafted, reviewed, and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Institutional Review Board at Beth Israel Deaconess Medical Center reviewed this study, protocol #2017P000167.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dong, Leveille, and Walker received financial support from the Robert Wood Johnson Foundation, Gordon and Betty Moore Foundation, Peterson Center on Healthcare, and Cambia Health Foundation
Informed consent
The survey included a statement of implied consent, as determined by the IRB.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.