
Abstract
Objectives
To find the prevalence of knowledge of arteriovenous fistula (AVF) self-care, its characteristics, and associated factors among hemodialysis patients and summarize the findings of various domains of AVF self-care in south Asian countries.
Methods
The systematic literature search was performed on online databases and additional sources to retrieve published articles on AVF self-care. We estimated the pooled prevalence using a random effects model in meta-analysis. Additionally, thematic knowledge regarding various aspects of AVF self-care was narratively summarized.
Results
Among the articles retrieved seven studies met our inclusion and exclusion criteria. The prevalence of AVF self-care in individual studies ranged from 59% to 99%, with an overall random pooled prevalence of 81% (95% CI, 68% to 94%). Major factors associated with self-care of AVF knowledge included patients’ educational status, age, vintage of hemodialysis, and healthcare personnel’s advice.
Discussion
Knowledge scarcity regarding potential measures of AVF self-care obligates the need for continuous education in hemodialysis patients. A multidisciplinary approach is vital to enhance self-care from pre- to post-creation of AVF in hemodialysis patients as well as their caregivers in order to prolong the patency rates and decrease the subsequent morbidity and mortality due to failure of AVF.
Introduction
The kidneys are a pair of vital excretory organs with extensive cellular complexity and functional diversity. 1 These are located just below the rib cage, one lies on each side of the spine, and are integral in maintaining the body's homeostasis, hormone secretion, metabolism, and excretion. 2 Permanent damage to these organs is known as chronic kidney disease (CKD). It can adversely affect the functioning of body systems and may prove to be fatal (estimated prevalence is around 8% to 16% worldwide). 3 Renal replacement therapy (RRT) is essential for survival as CKD advances to end-stage kidney disease (ESKD).2,4 There are two major modalities under RRT namely dialysis (hemodialysis (HD) and peritoneal dialysis) and kidney transplantation. HD is a life-sustaining extracorporeal blood purification therapy effective for rapid correction of symptoms in patients with ESKD.5,6 It is the most preferred choice when other RRT modalities such as peritoneal dialysis and kidney transplantation are contraindicated.2,7,8
Arteriovenous fistulas (AVFs) are a widely used means of establishing HD vascular access and are recommended by the Dialysis Outcomes Quality Initiative (DOQI) guidelines. 9 It is created by a surgical procedure where an artery is connected to a vein under the skin, which results in venous engorgement and enlargement, allowing large-bore needles to be cannulated for HD.10,11 A native AVF is a preferred HD vascular access because of its superior patency and lower complication rates.12,13 An AVF providing adequate blood flow is the key to effective HD and is also recognized as a “lifeline” for ESKD patients on long-term maintenance HD (MHD).14,15 They are also known as the “Achilles heel” of a chronic HD therapy because the fistula is susceptible to several complications such as edema in the hand, AVF thrombosis, aneurysm, infection, ischemia, and cardiovascular diseases.11,12,16,17 A leading problem associated with AVF is primary fistula failure due to multifactorial reasons explained under the broad categories of pre- and post-AVF creation, and long-term maintenance.10,12 Failure of AVF places the patient at a probability of inadequate dialysis, which may increase the complications along with morbidity and mortality.14,17,18 Periodical and persistent monitoring of AVF, along with self-care, can fend off the access complications.19,20 The responsibility of AVF care lies in the hands of the healthcare team and the ESKD patients.
Therefore, the patients should be instructed on self-care for AVF right from the pre-construction phase to its subsequent management. Early identification of AVF dysfunction and its management improves long-term patency and reduces secondary AVF failure. In developing countries, HD centers lack periodic vascular access monitoring teams. The lack of an AVF team increases the load on the nephrologist or dialysis nurse/technician to monitor AVF performance and identify impairments in addition to their regular responsibilities.14,18,19,21 Although there have been systematic reviews and meta-analyses on various aspects of AVF, no published systematic reviews have evaluated patients’ knowledge of AVF care. Through this systematic review, we aim to find the prevalence of knowledge of AVF self-care, its characteristics, and associated factors among HD patients and summarize the findings of individual studies over various domains of AVF self-care in south Asian countries. This will help CKD patients, various healthcare professionals, and researchers in the field of renal sciences to enhance their knowledge of AVF self-care.
Methods
This systematic review and meta-analysis were performed in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) quality requirement. 22 The review protocol was registered with PROSPERO (Registration number: CRD42022306300). The protocol was not published.
Eligibility criteria
A systematic search was conducted for cohort and cross-sectional studies aiming to appraise the knowledge of AVF self-care in ESKD patients undergoing HD in south Asian countries. The countries were Bangladesh, Bhutan, India, the Maldives, Nepal, Pakistan, and Sri Lanka. The authors did not include Afghanistan as some parts of this country belong to Central Asia. Studies were required to have knowledge or awareness related to AVF care as an outcome. Studies were also required to be empirical in nature. Articles were excluded if they did not assess the knowledge or awareness of AVF as an outcome, did not have a clearly stated methodology, and reported beyond South Asian countries. Systematic reviews, commentaries, grey literature, articles not published in English, and peer-reviewed journals were also excluded.
Search strategy
The systematic literature search was performed using online databases such as MEDLINE, EMBASE, PUBMED, Web of Science, and Google Scholar. Studies that were published from 2011 to 2021 were considered. The search strategy was developed by authors using database-specific controlled vocabularies and free text terms as presented in Table 1. Two authors (VNK and MNN) separately examined the titles, abstracts of citations, and full texts of potentially eligible studies were derived. Disagreement was addressed through one-on-one discussions, and if it persisted, the opinion of the senior author was solicited (PM). Bibliographies of retrieved articles were further examined for potential additional studies for inclusion. The final primary extraction for the authors was AVF self-care knowledge in HD patients.
Keywords developed for search strategy.
Data extraction
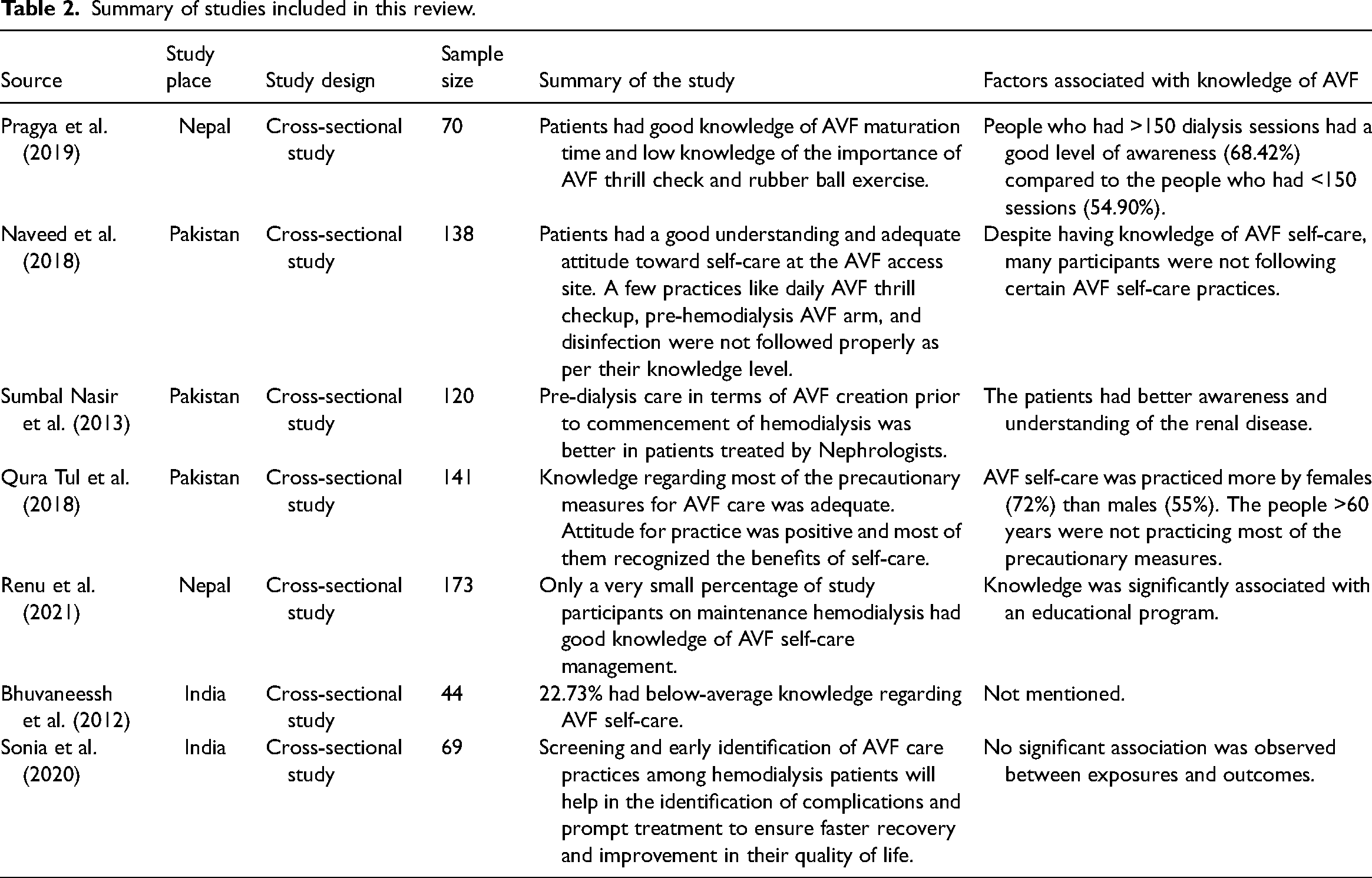
VNK and MNN independently extracted data from the appended studies in a Microsoft Excel Sheet. The following particulars regarding each eligible study were included: Title of the article, first author name, publication year, publisher, study place, study design, sampling technique, sample size, study duration, key findings regarding knowledge of AVF, the association of knowledge with exploratory variables, findings regarding other aspects of AVF and HD, limitations mentioned by authors, and future implications of studies. A list of finally selected articles with their characteristics has been presented in Table 2.
Summary of studies included in this review.
Statistical analysis
Statistical analyses were conducted to produce pooled event rates of outcomes of interest (proportion of patients with the correct knowledge score of AVF care). Anticipated to the nature of studies, substantial heterogeneity was expected, hence a random effects model meta-analysis using the inverse-variance method was done. 23 Publication bias was assessed using the Eggers test, as well as a visual inspection of the funnel plot. 24 Heterogeneity of the prevalence estimated between studies was assessed by the Q statistic and the I2 index, assuming that I2 values of 25%, 50%, and 75% represented low, medium, and high heterogeneity, respectively. 25 Statistical analyses were done using STATA 15.1.
Quality assessment of the included studies
The National Heart, Lung, and Blood Institute Study Quality Assessment Tools for observational and cross-sectional studies were utilized to assess the methodological quality of the final screened articles. 26 The tool has 14 items that have been used in preceding systematic reviews of observational studies.27,28 Each item was assessed through a criterion where the possible answers were “yes,” “no,” or “other” (cannot determine, not applicable, or not reported). The tool enables us to score and weigh the evidence to rate the overall quality of each study as “good,” “fair,” or “poor,” indicating the validity of findings in each study.
Results
Study selection
The process of study selection is outlined in the PRISMA flow diagram in Figure 1. The initial search furnished 17,300 results. After removing duplicates, 15,560 articles were available for title and abstract screening. Sixty-eight articles remained for full-text evaluation, of which 61 were excluded because of non-compliance to inclusion criteria: few were reviews (n = 12) and conference presentations (n = 5), 18 articles presented knowledge of AVF care among healthcare staff, nine studies focused on AVF complications and management, 11 studies evaluated knowledge of diet in dialysis patients, and the rest of the articles were interventions associated with AVF and HD (n = 6).
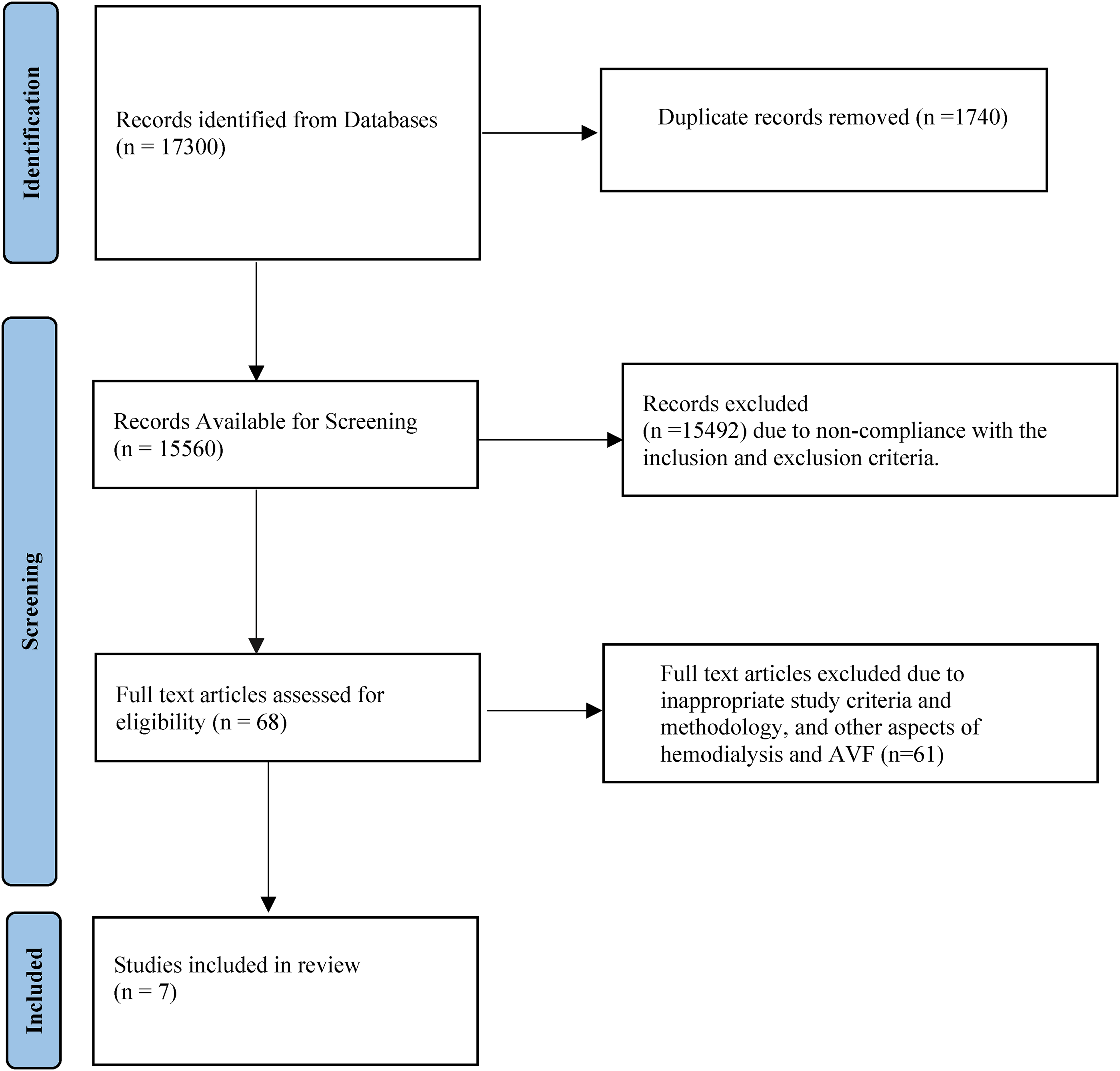
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow diagram depicting the process and recruitment of studies.
Study characteristics
The attributes of each included study are summarized in Table 2. There were a total of seven studies: two from Nepal conducted in the years 2019 and 2021,29,30 three from Pakistan conducted in the years 2013 and 2018,31–33 and two from India conducted in the years 2012 and 2020.34,35 Study designs and sampling techniques were clearly defined in all the studies except for Rashid et al., 32 who did not mention the sampling technique. Besides the two studies from India,34,35 the authors in the other studies mentioned the duration of the study. All the studies were cross-sectional in nature with the outcome variable as knowledge or awareness of AVF self-care. Among the articles assessing the knowledge/awareness of self-care, four articles also attempted to evaluate the attitude and practice associated with self-care of AVF in HD patients. All the studies recruited participants from a tertiary care hospital. Most of the studies reported the limitation of a cross-sectional design because of the temporal relation between the outcome and exposure could not be established as both are explored at the same time.
Knowledge regarding AVF and meta-analysis
Among the included studies, five studies examined the knowledge score simultaneously, where each component was categorized as good or poor. Hence, the pooled estimate has been derived for the prevalence of good knowledge scores using meta-analysis. The sample size of the studies ranged from 44 to 141 individuals. Altogether, the five studies included 566 individuals. Variation between studies was observed as expected. The meta-analysis indicated that between-study variability was high (Tau2 = 0.02; heterogeneity I2 = 96.77% with heterogeneity chi-square = 105.36; degree of freedom = 4; and p < 0.001). Individual study prevalence estimates ranged from 59% to 99% with the overall random pooled prevalence of 81% (95% CI, 68% to 94%). Studies weighted approximately equal weights on individual studies ranging from 18.13% to 21.70% due to high heterogeneity between studies. Figure 2 presents the forest plot derived from the meta-analysis of the knowledge score.
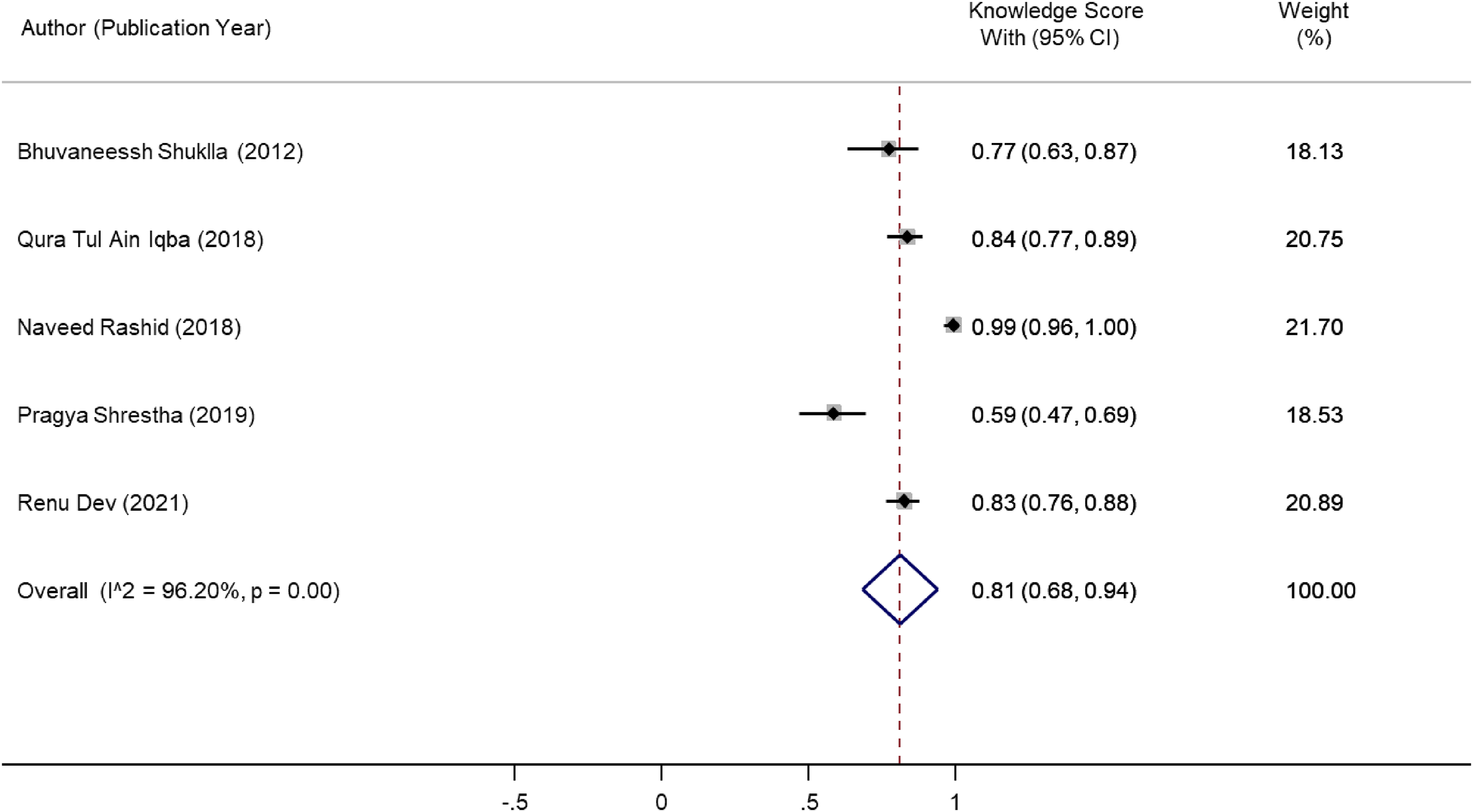
Forest plot derived from knowledge score.
Egger's test for the asymmetry in the funnel plot was significant (intercept = −6.36, 95% CI, −9.58 to −3.15, p = 0.00). However, the inadequate numbers of studies underpowered the existing publication bias evaluation methods, as presented in Figure 3.
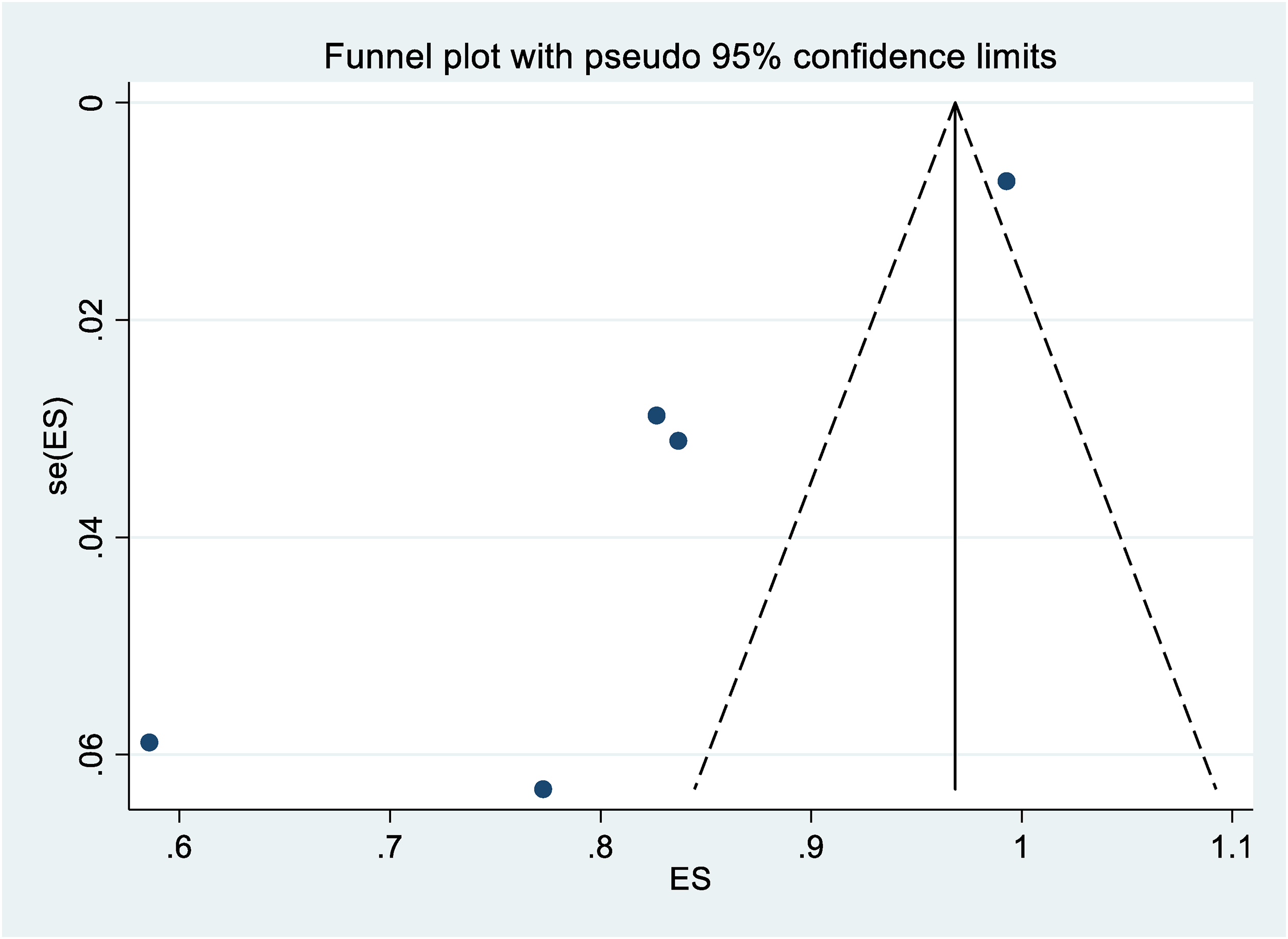
Funnel plot.
Knowledge regarding AVF maturation time
The knowledge regarding adequate AVF maturation time was reflected in the responses of less than half of the study subjects (54.28%). 29 The study conducted by Qura Tul et al. reported that 83.4% of patients had appropriate knowledge regarding AVF care during the maturation and curative phases. 31 AVF care during the maturation phase was better in patients who saw nephrologists rather than a general physician. Around 2.1% of the population had no knowledge about practicing manual compression exercises during the AVF maturation phase. 31
Knowledge of the importance of AVF thrill check
The included studies reported a lack of knowledge in patients regarding checking AVF thrill. 29 Less than 50% of the patients had the awareness to check their AVF thrill and pulse daily. Around 94% of participants reported knowledge of checking AVF thrill regularly. 32 Abraham et al. 35 reported that 49% of the subjects had poor knowledge and practice in checking AVF thrills. Some participants had a poor practice of checking the thrill even after having adequate knowledge of self-care.32,35
Knowledge regarding continuous management of AVF
Shrestha et al. 29 evidenced that most of the people were aware of protecting the AVF arm from injuries. The article also reported good knowledge about avoiding blood pressure measurement on the AVF arm and avoiding carrying heavy items.29,31 The study also reported good knowledge of HD patients about avoiding intravenous administration of drugs and wearing tight watches, jewelry, and clothes on the arm with AVF. Awareness regarding rubber ball exercise was very low among the participants of the study (24.28%). Rashid et al. reported good self-care knowledge in patients with compliance to AVF arm weight avoidance and needle pricking. 32 Patients reported a lack of knowledge regarding the disinfection of the AVF access site prior to cannulation and were unaware of the consequences of wearing tight clothes. Aspects of AVF care like hemostasis at the fistula site, prevention of hematoma after dialysis, and arm elevation to prevent swelling of the access site were least common in patients as reported by Iqbal et al. 31 They also reported that around 37% of patients were unaware of the importance of washing the AVF arm with soap and water prior to dialysis. A similar proportion of the population presented a lack of knowledge about avoiding sleeping on AVF arm. In the studies, around 44.7% of the population attempted to take care of AVF and follow all the precautionary measures, while 40.4% took maximum precautionary measures most of the time.31,33
The sub-group analysis could not be done as there was an inadequate number of studies. It was possible to present a sub-group analysis for the percentage of participants having correct knowledge to “avoid sleeping over the AVF access arm,” and the forest plot presented (Figure 4) suggests the overall random pooled estimate of 88% (95% CI, 77% to 99%), while individual study estimates ranged from 73% to 98%.
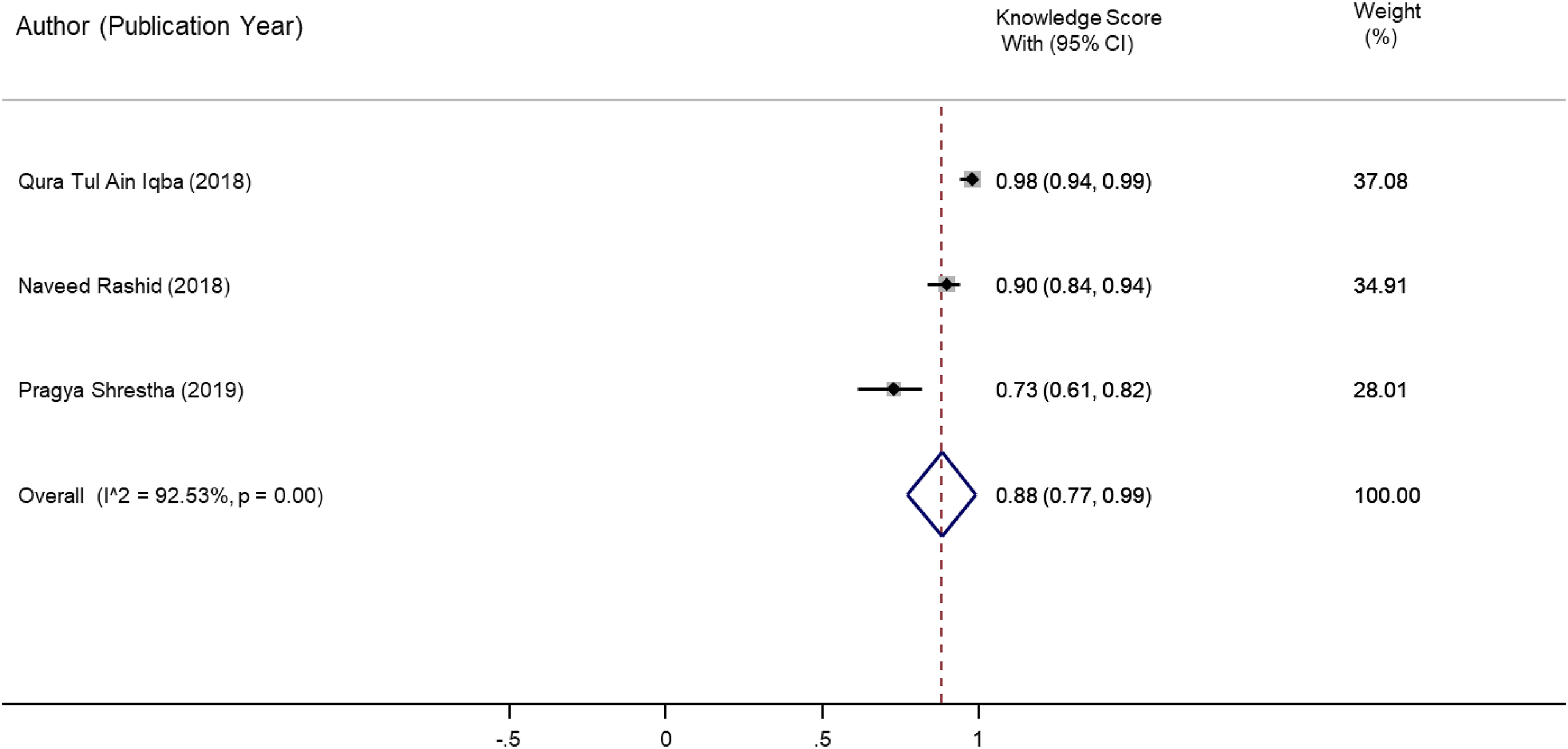
Forest plot for knowledge to avoid sleeping on access site.
Knowledge regarding healthcare personnel advice
Studies reported that AVF self-care was better when it was created before the first HD, but only 20% of patients were dialyzed through AVF as access during the first HD. Studies reported that patients had trouble following the advice rendered by healthcare professionals and treating nephrologists. Less than half of the patients followed advice regarding AVF and self-care, while the remaining patients delayed the creation of AVF despite knowing the potential benefits of starting first HD through AVF. The patients attending general physicians reported following less advice (10.4%) on AVF self-care as compared to those who visited nephrologists (83.6%). Also, advice regarding follow-up was better rendered by nephrologists (55.8%) than physicians (40%).32,33
Association of AVF knowledge with exploratory variables
A significant association of knowledge with socio-demographic characteristics and other exploratory variables associated with HD and AVF self-care was observed. Those who were literate had good awareness compared to those who were illiterate. 29 Persons between 17 and 46 years of age had a high level of knowledge (60%) compared to the age group of 47 to 76 years (57.14%). 32 Males had better knowledge than females. Patients on HD for a period of <1 year had good knowledge (95.5%) in contrast to patients on HD for 1 to 3 years (89.5%) and more than 3 years (88.2%). AVF self-care was practiced more by females (72%) than males (55%). 31 Persons aged above 60 years were not practicing most of the precautionary measures. More than half of the participants (66.6%) underwent HD more than 50 times, and (97.1%) never had any exposure to AVF education. 35 Shukla and Kaur 34 did not report any association of AVF knowledge with exploratory variables in their study.
Attitude and practice regarding AVF self-care
The majority of the participants were aware of the purpose of AVF and its advantages over dialysis catheters. In total, 97.8% of participants agreed that fistula self-care is beneficial; 99.3% of the participants felt motivated to practice AVF self-care at home and during HD. 34 In the “always practising” group, compliance for “AVF arm weight avoidance” and “AVF access site prick avoidance” was highest.32,33,35 The majority of the participants were practicing AVF care during HD. 32 A “never practising” attitude was observed for “asking for pre hemodialysis disinfection requests” and “ability to avoid wearing accessories or clothes on the AVF access site.” The frequency of practice was high in the adequate knowledge group. In this group, 92.8% of people knew about avoiding weight on the AVF arm, and 94.9% practiced it. 33 Despite possessing knowledge of self-care, many were not following certain AVF self-care practices.31,33,35
Discussion
Self-care in ESKD patients influences health outcomes as MHD is a long-term life-sustaining treatment, and self-care of AVF is even vital to increase the quality of life. 36 The care and maintenance of vascular access for HD is a major challenge for people with ESKD. Implementing AVF self-care behavior helps to maintain the best possible conditions as a good state of access influences the efficacy of the HD treatment.32,33,35–37 The combined data from this systematic review and meta-analysis demonstrates that the majority of the participants had good knowledge about self-care for AVF (80%). In contrast, a study from Brazil concluded that the majority of the participants had inadequate knowledge regarding AVF self-care. 38 The primary reason for this dissimilarity is the educational status of the study population in both studies. The study conducted in Brazil had a greater number of participants who had a low education level whereas, in our systematic review, it was observed that the proportion of educated people was higher. The knowledge regarding AVF self-care involves many aspects right from the construction of AVF to lifelong continuous management.2,10 Once the AVF is constructed by the surgeons, the patient should be educated by the healthcare team about the self-care of the AVF. They should also follow the advice of the healthcare team and practice them in their routine self-care.32,35,37 We also found that knowledge regarding AVF care during the maturation phase ranged from 50% to 80%. It is recommended not to use AVF for HD soon after the creation, as it requires time for maturation which is around four to six weeks. 39 “According to KDOQI guidelines, a viable fistula is one that resides approximately 0.6 cm from the skin surface, has a flow of >600 mL/min, and has a diameter >0.6 cm.”15,39 Following the creation of an AVF, the vein gets increased blood flow, the wall of the vein eventually thickens, and the lumen dilates. These modifications allow the AVF vein to effectively deliver adequate blood for HD and allow repeated cannulation for each HD.40,41 A major complication after AVF creation is maturation failure. Prior studies report that around 30% to 50% of AVFs fail to mature. 40 The HD individuals should be sensitized about self-care during the curative phase and maturation time as this is vital to prevent AVF failure.37,40,41 It has been evidenced from the literature that a pre-dialysis education program has been vital in improving self-care for AVF and further complications.14,42
A narrative synthesis of the included articles reported poor knowledge (below 50%) of participants regarding the importance of checking AVF thrill. The continuous management of AVF includes monitoring and surveillance through physical examination and a few clinical procedures such as imaging, ultrasound, access recirculation, and pressure monitoring.16,42 It has also been evident that the efficiency of HD depends on AVF, and low efficiency affects the patient's quality of life. 43 Prior studies have reported that good management of AVF decreases hospitalization rates because of access failure and other complications.7,20 Physical examination of AVF includes site inspection, listening to bruits and palpating thrills are useful methods and are the step toward the diagnosis of various AVF-related complications.16,42 Patients themselves can do the physical examination and detect stenosis and related complications. Our review found that, apart from thrill check, a maximum number of people were aware of AVF protection precautionary measures in terms of avoiding blood pressure measurement, cannulation of the AVF arm except for HD, trauma, wearing of tight clothes or watch or jewelry, carrying heavy items, and sleeping over the AVF arm. Awareness of AVF needling site hemostasis, post-AVF cannulation hematoma prevention, arm elevation to prevent swelling of the AVF site, washing the AVF arm with soap prior to HD, and rubber ball exercise were less prevalent compared to the other precautionary measures. The study conducted in Brazil found similar variables related to AVF protection measures and reported that the maximum number of participants were less aware of AVF arm exercise, complications of weightlifting with the AVF arm, improper care during the curative phase, and hematoma formation in AVF arm. They also had good knowledge regarding the reduction of water intake to avoid weight gain, washing the AVF arm, avoiding blood pressure measurement, and cannulation of the AVF arm except for HD.16,37,42
In the above results, it is seen that the studies have listed many AVF care-related practices, knowledge levels, and how the participants have implemented them in their day-to-day lives. To increase the knowledge level of AVF care-related practices among the patients and make them practice, a close collaboration between the health professionals (nephrologists, vascular surgeons, dialysis professionals and nurses) and dialysis patients is required. This will help to minimize the problems of vascular access and potentiate its vigilance. 44 Patient education is of high importance for AVF care. Healthcare personnel must educate and advise the patients on how to take care of their fistula, assess the AVF function, and know the signs and symptoms of AVF dysfunction. The synthesis of this systematic review shows that although a group of participants (39.3%) had higher awareness about pre-dialysis care and AVF creation prior to the first HD by nephrologists and physicians, only 20% of patients had followed the advice for timely AVF creation and undergone first HD through it. A study conducted in the United States of America included outpatient dialysis clinics, and they observed that the use of AVF/arteriovenous graft for the first HD was very low in the participants with lower knowledge.10,45,46 All these studies recommend that continuous education programs are required to increase AVF use. Results of the reviewed studies reveal that there is a significant association between AVF knowledge and socio-demographic variables, literacy status, and continuous educational programs on HD self-care. A study from Saudi Arabia revealed similar findings. Those who were literate presented better awareness. The participants in the age group of 17 to 46 years had a high level of awareness compared to those in the age range of 47 to 76 years. Similar findings were reported in HD patients concerning the care of AVF in the Dialysis Centre of King Khaled Hospital and Hail Dialysis Care Centre, Saudi Arabia. 47 The reason behind the decreased perception of self-care in these studies were lack of motivation, inappropriate knowledge about health, and lifelong treatment of chronic illnesses.37,41 Adequate knowledge and motivation in patients with any chronic condition may help change the perceived negativity of the disease, specifically when the patient needs to undergo long-term treatment for survival.44,47,48
The presented review involves certain limitations, which are thus acknowledged. Firstly, limitations might be present in the existing body of literature as the studies were included from specific databases and sources, hence, there is a possibility that studies that might have met the criteria but did not appear in the search process. Another limitation is associated with high heterogeneity in methods and itemized responses, which restricted meta-analysis of specific factors. The included studies were longitudinal in design or had follow-ups that inhibit the determination of a causal relationship. It is recommended that future research acknowledge these limitations and informs better corroboration with precision.
Conclusion
The combined data from the systematic review and meta-analysis showed good knowledge regarding AVF self-care in HD patients. However, a lack of knowledge regarding potential measures of self-care was observed. The presented study obligates the need to establish a vascular access surveillance team to continuously monitor and educate the patients regarding AVF self-care. A multidisciplinary approach is vital to enhance self-care from pre- to post-creation of AVF in HD patients as well as their caregivers in order to prolong the patency rates and decrease the subsequent morbidity and mortality due to failure of AVF. Further research should include qualitative investigations to better understand the barriers and facilitators for AVF self-care among HD patients.
Footnotes
Acknowledgments
The authors are grateful to Ms. Shumayla and Ms. Shivani Garg, Jhpiego, India for proofreading this article. We would also like to extend our gratitude to Ms. Anitha Guru for copy-editing the manuscript. Last but not the least, we extend gratitude to our colleagues for their encouragement and motivation.
Contributorship
VNK, MNN, and BT conceptualized this study. VNK and MNN carried out a literature review and data extraction. NP carried out a statistical analysis. BT conducted narrative synthesis and interpretation. VNK and MNN were involved in preparing the initial draft of the manuscript, which was critically revised by BT. PG and PM were responsible for the methodological aspects of the study. All authors have read and approved the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Since this review is a synthesis of published articles, it does not require ethical approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
The first and corresponding authors of this study will act as a Guarantor.
Informed consent
Not applicable as the study involved synthesis of articles that have been published.