
Abstract
Objectives
People living with chronic obstructive pulmonary disease (COPD) in regional communities experience a higher disease burden and have poorer access to support services. This study sought to investigate the acceptability of a peer-led self-management program (SMP) in regional Tasmania, Australia.
Methods
This descriptive qualitative study, underpinned by interpretivism used semi-structured one-to-one interviews to gather data to explore COPD patients’ views of peer-led SMPs. Purposeful sampling recruited a sample of 8 women and 2 men. Data was analysed using a thematic approach.
Results
The three final themes, ‘Normality and Living with the disease’, a ‘Platform for sharing’ and ‘Communication mismatch’ suggest that peer-led SMPs could offer an opportunity to share experiences. The themes also suggest that COPD often manifested as a deviation from ‘normal life’. Communication was often felt to be ambiguous leading to tension between the health experts and people living with the condition.
Discussion
Peer-led SMP has the potential to provide the much-needed support for people living with COPD in regional communities. This will ensure that they are empowered to live with the condition with dignity and respect. Benefits of exchanging ideas and socialisation should not be ignored and may enhance sustainability of SMPs.
Introduction
Chronic obstructive pulmonary disease (COPD) is an umbrella term for a group of progressive lung conditions including emphysema, chronic bronchitis and chronic asthma in which airway narrowing causes breathing difficulties. It is the third leading cause of death worldwide and the third leading burden of disease in Australia. 1 A characteristic of chronic diseases is that they often require a long period of supervision, observation and care. 2 COPD is associated with significant disability, impaired quality of life and high utilisation of healthcare resources. 3 People living with COPD in rural communities in Australia suffer from a higher disease burden and have poorer access to support services. 1 Tasmania experiences the same issues of rural health as the rest of Australia in addition to some unique factors specific to the state. Like other regions in Australia, due to the burden on the health care system, most of the population must travel to get to health services. Tasmania has unique demographic and socioeconomic factors that impact on demand for services, the cost of providing healthcare and the efficient and effective delivery of services. Tasmania has the third smallest population in Australia, and it is significantly dispersed. 4 This often means that even relatively short distances are long drives reducing access to support. 4 In addition to having the highest proportion of people aged 65 and over, Tasmania has one of the highest rates of chronic conditions of all Australian states and territories. 5 49.8% compared to 39% nationally of all potentially preventable hospitalisations (PPHs) are attributed to chronic conditions in Tasmania. 5 Prevalence of COPD in Tasmania is at 2.7% compared to 2.5% national average. 5 Furthermore, 16.4% of adults in Tasmania are daily smokers compared with 13.8% nationally in Australia. 4 Regional and remote Tasmania are relatively under-resourced by allied health professionals, providing an impetus for reviewing models of care that spread allied health services equitably. 6 Currently, most clinics and support programs are based or run from the tertiary hospital sites.
Self-management is an aspect of the continuum of disease management whose goal is to empower the patient at all stages of the disease. 7 Self-management programs (SMPs) aim at behaviour change to sustain treatment effects. 7 Implementation of SMPs for chronic diseases has been so varied, often reported poor because the most effective model is unclear. 8 Consequently, there has been a shift towards a need for more collaborative interdisciplinary approaches of chronic disease management. New patient-led models of care such as peer-led SMPs are emerging to include patients, families, and their carers as partners in care. 9 As well as playing an important role in the provision of quality care for chronic conditions, SMPs attempt to shift some of the decision-making focus to the patient, 10 moving the balance of power from experts where the patient takes a passive role to a more active patient-centred model that offers greater autonomy to the patient. 10 Such patient-centred models present a promising strategy for managing chronic conditions beyond healthcare walls, increasing access to support for people living in outer regional and low socio-economic areas who are less likely to seek help. 11 It is unclear how SMP programs are viewed by people living with COPD, consequently, this study sought to investigate the acceptability of peer-led SMP for people living with COPD and living in regional Southern Tasmania, Australia.
Methods
Design
This descriptive qualitative study used semi-structured one-to-one interviews to gather data to explore COPD patients’ views of peer-led SMP. This study design is suitable as it allows the researcher to firstly explore how patients interpret, understand, and give meaning to living with their COPD, and secondly describe their subjective views about SMP within the context of living with COPD in regional and rural areas. 12 The theoretical framework for this study was interpretivism which provides a lens to explore how people living with COPD might interact with SMP, interpret and make sense of their experiences within their social context. 12 The researcher’s backgrounds in allied health (physiotherapy) and public health facilitated identifying and describing the COPD patient's acceptability of the content and barriers to a peer-led SMP.13,14 For this study, SMP interventions were defined as those that enhance patients’ active role and responsibility in symptom monitoring, problem solving skills and healthy living. 7 The study was approved by the Tasmanian Human Research Ethics Committee (H0017642).
Setting
This study was undertaken in 2019, in the state of Tasmania, Australia with a reported population of 522,327 at the time of the study. 4 Tasmania is considered regional or remote under the Australian Standard Geographic Classification Remoteness Areas. 15 Two regional sites were used for this study, Hobart, an RA2 Regional area with a population of approximately 200,000 residents and New Norfolk, an outer regional centre with a population of 5500, in Southern Tasmania. The Royal Hobart Hospital (RHH), a 501-bed tertiary referral hospital in Southern Tasmania and New Norfolk District Hospital (NNDH), a 14-bed sub-acute facility, 45 km from the RHH were the recruitment sites.
Sample and recruitment
Purposeful sampling was used to recruit a sample of up to 15 men and women aged >18 years who were living with COPD during inpatient admission at either the RHH or NNDH and at least 2 months post-COPD exacerbation. COPD was not necessarily the primary diagnosis or reason for admission. Recruitment occurred between April and August 2019. Potential participants were first identified by treating physiotherapists during their hospital admission at both sites and verbally invited to participate. Participants were provided with written study information and asked to complete an expression of interest form. Interested participants were invited to participate in one face-to-face interview of approximately 60–90 minutes during their hospital admission. Physiotherapy staff were provided with a 1-hour study information briefing to support the recruitment strategy prior to commencing. Recruitment continued until no new participants expressed interest in joining the study during the period. 13 A total of 8 females and 2 males (N = 10) consented and were invited to participate in one face-to-face interview of approximately 60–90 minutes during their hospital admission. All participants were in the hospital for ‘other’ reasons, not COPD primarily. One person was discharged home before the interview could take place and another became medically unwell, leaving a total sample of 8.
Data collection and analysis
One researcher, Author 1, an allied health professional conducted all interviews and used written field notes to record thoughts, and observations during data collection. At the commencement of the interview, the SMP was described to each participant and interview prompts were used to collect information on age, gender, and usual place of care and to generate conversation on views and suggestions for peer-led SMPs. Interview prompts were informed by the research questions, the aim of the study and the literature 8 and included ‘tell me about your COPD, age, supports, benefits and barriers to SMP, and any advice to other people living with COPD’ (see Supplementary File 1). The interview prompts were piloted on two staff members and minor adjustments to the wording were made to limit question ambiguity. All interviews were audio recorded and transcribed verbatim by Author 1 and any names; places were replaced with pseudonyms. Two researchers, Author 1, a male, allied health care professional with experience treating COPD patients in acute, sub-acute and community settings, and Author 3, a female with a background in public health, analysed the data. All data including researcher field notes were combined and thematically analysed by the two researchers using a matrix (see Supplementary File 2) and a five-step process: familiarisation through reading and re-reading, initial coding to a coding framework (Peer-led, Content and Barriers) informed by the literature and aim, re-reading, reviewing the coded data and reducing into sub-themes, analysing, and refining to generate, define/describe and name the final three themes,13,16 ‘Normality and Living with the disease’, a ‘Platform for sharing’ and ‘Communication mismatch’ (Figure 1). Direct quotes from the data were used to formulate meanings using a matrix. 17 The team met weekly during the 5-month period of data collection and analysis. Any conflicts were resolved through discussion at each meeting.
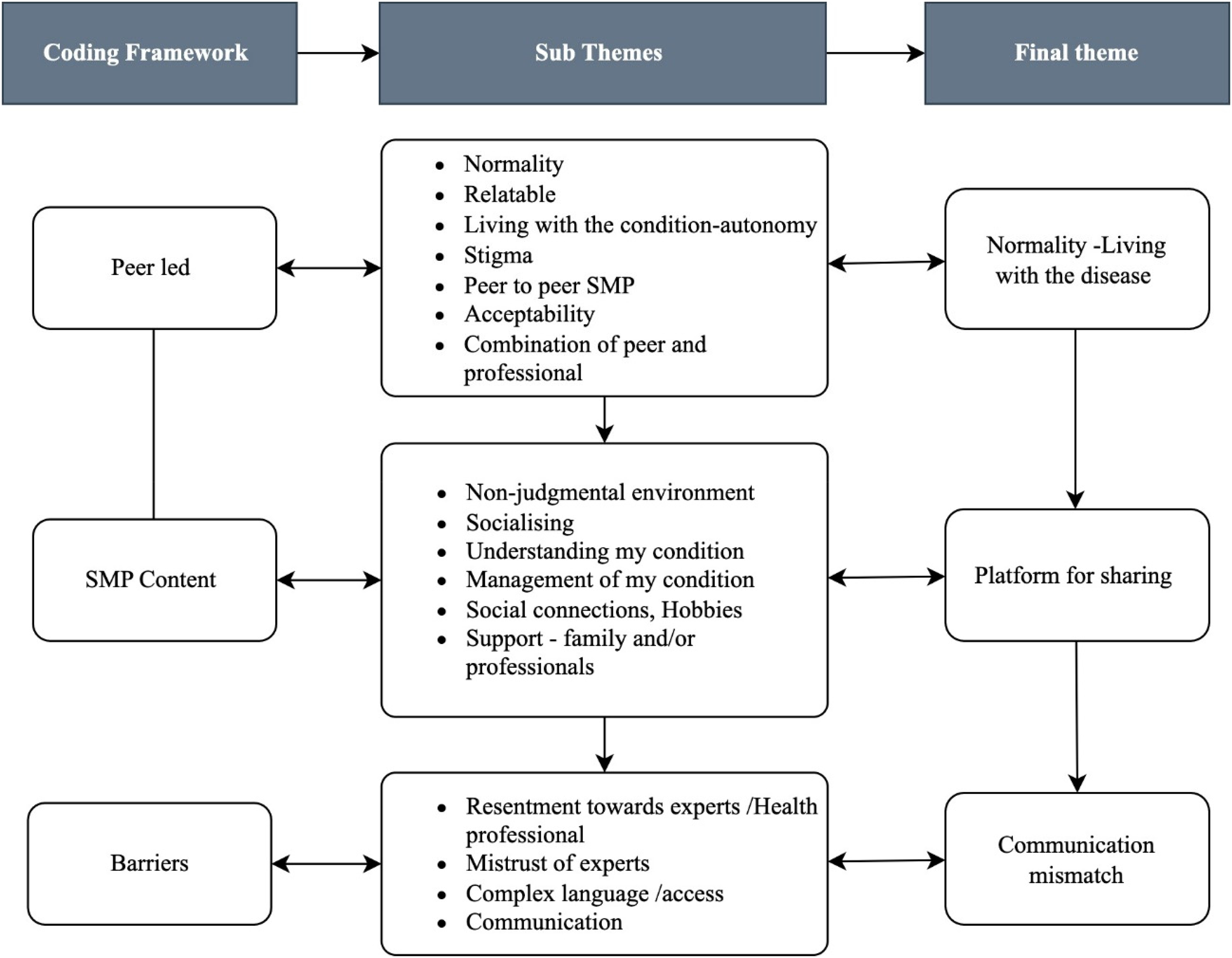
Coding framework.
Results
Most participants were female, 6 compared to 2 males and 7 were living and receiving care at the NNDH. The age of participants ranged from 45 to over 75 years old, with the majority being over 65 years which is consistent with Australian disease profiles for COPD. 1
Normality and living with the disease
Participants openly spoke about the physical and emotional impact of living with their illness describing COPD as an ‘emotional thing’. Alternative models of care that were socially relevant to regional life were viewed in general as offering better support on how they navigated their illness. For all participants, both male and female, COPD manifested as a deviation from ‘normal life’, where they were always short of breath, often fearing the future and dependent on oxygen or a ventilator. Maintaining a sense of control was an important part of learning to live with what was felt to be a debilitating illness. Both men and women frequently expressed a desire to live ‘normal lives’ and not as people with a condition or disease label assigned to them by their doctors. As George (69 years) said, ‘To tell you the truth, I don’t know whether people can just straightaway manage it. It is something that really strikes you. The more you talk about it, the more you get to know about it and the more you get to know the more are able to control it a bit better. It's not you are being able to control the COPD but maybe it should not control you. You gotta be careful and do the best you can’.
Consequently, participants in this study appeared to work hard to manage their chronic condition and reclaim what they often described as a loss of control by trying to adhere to often complex prescription action plans and preventative medications.
The participant's desire to regain autonomy over chronic illness suggests that people-centred programs such as peer-led SMPs may offer avenues for improved self-management. This was felt to allow them to opt out of the medicalised chronic disease ‘sick role’ where they are not responsible for being ill and instead learn to manage their condition and live a normal life. 18
Platform for sharing
Overall, participants felt positive about peer-led SMPs. When asked how the peer-led SMPs could support them to manage their COPD better, participants responded with a sense of camaraderie citing that they could be ‘more honest with someone who has been there’ (Jo, 74 years). Similarly, Mary (47 years) felt that peer support would be ‘great because you’d be talking one on one to someone that's got exactly the same thing that you’ve got; you can relate to them’.
Social interaction with peers (others living with COPD) was considered a major benefit of peer-led SMP's and key to helping sustain access to support for those living with a chronic illness, particularly those in outer regional areas. It was clear from the data that people living with COPD often felt isolated by their condition as it often limit their mobility and opportunities to socialise outside of their homes. Providing avenues to socialise, share experiences, and pass on ways of managing COPD in their own communities was felt to offer great insight into managing their condition. Participants highlighted the need for social connectiveness which includes sharing of experiences, passing on support that is based on lived experiences and provision of emotional support in a relaxed manner. This was because, as George (69 years) explained ‘never think that you know everything, it’s only by engaging with other people that you realise what you don't know but then I also have things that I can share in return’.
‘I could say social benefits, you enjoy the company of those people [who are living with COPD] more, say the boys dance, or walking club or your singing, you are more likely to relax and more likely to take it all in and take an interest and keep on continuing rather than quit’ (Alice 73 years).
A consistent response to the question about the benefits of SMPs was a need to share and tell and have their story heard as Prom (55 years) stated, ‘to tell our own stories’. Peer-led programs like SMPs have the potential to offer space for the sharing of experiences and learning through a non-judgmental environment that may help to reduce the sense of isolation and stigma associated with COPD. 18
Communication mismatch
There was variable confidence in their own ability to be a peer-leader for a COPD peer-led SMP. This was supported by statements like ‘I’m not very educated myself; I know I’m not a very good talker’. When asked about potential barriers to the program, participants highlighted issues of accessibility.
On the whole, where SMP are led and facilitated by health experts, there seem to be overwhelming communication mismatch between people living with COPD and health experts. Whilst participants appeared to appreciate the role played by health experts in the provision of support in medication and symptom management, there were mixed feelings and often a sense of resentment towards the role played by the health experts in SMPs. This included ambiguous use of language that acted to distance the patient 19 often leading to confusion. Others felt disempowered and dehumanised by the health experts in the ‘city’ hospital where they described being treated as a ‘disease rather than a human’. Alice (73 years) spoke of feeling like a ‘social outcast’. Some participants spoke of feeling unheard, ‘talked down to’ and pressured by health experts to change lifestyles focusing on losing weight, diet and exercising. This sentiment appeared again to be centred around the relationship between health and medical experts generated by the language used by health experts when offering support or instructions for disease management. As Mary (47 years) explained, ‘Whereas sometimes medical professionals forget that they are talking to an actual human being … and that we don’t always understand what they’re saying. We need it simplified and if it's shown in a simplified manner, in a way that's understood …then people can follow say the action plan and umm… understand it more and understand their asthma better’.
Overall participants felt that health experts lacked lived experience and therefore could not understand what it was like to live with COPD, citing that reading about it does not help them understand the lived experiences. Others felt that health experts were not aware of some barriers faced by people living with COPD which include need to travel, access to specialists and general practitioners, care demands and stress on family members. These issues were felt to be more problematic for those who lived in regional areas where services were often scarce. 19
Discussion
This pilot study sought to investigate the acceptability of peer-led SMP from the perspective of people living with COPD in Southern Tasmania, with a view to informing a new patient-centred model of care. Overall, peer-led SMPs were viewed positively. The study findings reveal the importance of tailoring the SMP model and language to allow people living with the condition to engage. The strength of this study is the insight gained into the patient's perspective on peer-led SMP. People living with COPD wish for relaxed and non-judgemental environments to share experiences and socialise. This approach would empower those living with chronic conditions to adapt to their diagnosis and promote positive health behaviours resulting in higher levels of knowledge, skills, and confidence. 20
The role of SMPs in the management of chronic conditions and in reducing hospital admissions is not disputed but there is still a poverty of evidence as to the role played by peer-led SMPs. 7 Further research has been recommended to identify specific support that will help patients with mild to moderate COPD cope and adapt to the progressive condition, 21 making the findings of this research significant. Most current evidence supports collaborative models of care involving a partnership between the individual and the care provider. 7 Such programs have focussed on COPD patients in secondary and tertiary care settings following hospitalisation with less focus on improving COPD self-management outcomes in primary care settings. 21 However, there is a growing emphasis and shift towards care beyond the clinic settings making the findings of this study insightful. 7 A study on multiple sclerosis compared peer-led and nurse-led self-management training in enhancing the subjective well-being of patients and found improved positive experience in the peer-led group. 22 Culturally relevant peer support in diabetes programs for the United Kingdom Bangladeshi and New Zealand Maori communities was associated with improved health outcomes. 23 Peer-led SMP have been shown to be effective because people share social and cultural connections. Whilst COPD impacts negatively on social interactions due to associated limited function, mobility, embarrassment from symptoms and fear of shortness of breath, 7 the benefits of exchanging ideas and socialisation should not be ignored and can potentially enhance the sustainability of SMPs. In our study, participants expressed confidence when speaking and learning from people with the same condition. Peer-led SMP provides a safe platform for sharing ideas and assisting in addressing issues around stigmas. Peers can relate to each other making activities meaningful and satisfying. 23 In the book, the wounded storyteller, Frank, Arthur W. 24 highlights that people tell stories not just to work out their own changing identities, but also to guide others who will follow them. The narrativised reconstruction is concerned with gaining meaning and import to the illness by placing it within the context of one's own life and reconstructing the narrative of the self. 24 The reconstruction of one's own life story is of central importance and could be integrated as part of the framework of SMPs.
Findings from this study highlighted the fact that people living with COPD want to be treated with dignity and respect. Stigma, judgement and victim blaming often increase the burden of living with a chronic disease and people living with COPD experience isolation and loss of function and social life. 7 In addition, living with a chronic disease brings a sense of hostility and self-blame due to perceived stigma, 18 negatively affecting people's sense of identity and resulting in changes in values, expectations and life priorities. 19 Consequently, as our study and others have shown, people living with chronic diseases such as COPD work hard to self-manage and regain control of their lives. 25 Peer-led SMPs may assist self-reflection whereby patients adopt an active role in the management of their condition driven by the motivation to prevent another exacerbation attack. 7
Consistent with other research, ambiguous interaction between health professionals and patients with a chronic disease was evident in this study. 19 People with COPD are often left feeling like they are victims of the disease, dehumanised by some of the medical language and interventions. 10 In our study, interactions with health professionals were sometimes viewed as condescending in their approach. Other studies have suggested that health professionals view people living with COPD as lacking health literacy which limits their understanding and authority over their condition and healthcare because of insufficient knowledge. 18 However, our study suggests that patients had a good understanding of their COPD and actively managed their treatment plans but felt distanced from health professionals by the medical technical language. Peer-led interventions such as SMPs may help to unite health professionals with their patients and support the translation of health knowledge and empower the person living with complex chronic conditions to make more informed choices and decisions about their treatment and well-being.
Implication to practice and study limitations
In an area of research dominated by survey and biological research, this qualitative study generated valuable insights and intricate perspectives from a patient's perspective on the acceptability of peer-led SMP in regional communities. The strength of this study is the insight gained into the patient's perspective about managing their conditions and living ‘normal’ lives. Whilst peer-led SMPs were viewed positively, people living with COPD wish for relaxed and non-judgemental environments to share experiences and socialise. When designing SMPs the patient's social context, perspective and needs should guide the framework.
A limitation of our study is that most of our small sample was made up of women living with COPD in a regional area. Though this offers an interesting women's perspective from rurally based women which is often lacking in the literature, 26 a more diverse representative sample is needed. Further analysis is needed to explore the impact of gender and social context. Studies to explore the health literacy of health professionals and people living with COPD in regional places are required to inform how health and medical professionals can work more closely with patients to improve trust and autonomy. 19
Conclusion
Peer-led SMP has the potential to provide the much-needed support for people living with COPD in regional communities. With tailored peer-led SMPs, COPD patients are empowered to live with the condition with dignity and respect. The benefits of exchanging ideas and socialisation should not be ignored and may enhance the sustainability of SMP's.
Supplemental Material
sj-docx-1-chi-10.1177_17423953231163450 - Supplemental material for Acceptability of a peer-led self-management program for people living with chronic obstructive pulmonary disease in regional Southern Tasmania in Australia: A qualitative study
Supplemental material, sj-docx-1-chi-10.1177_17423953231163450 for Acceptability of a peer-led self-management program for people living with chronic obstructive pulmonary disease in regional Southern Tasmania in Australia: A qualitative study by Innocent Tawanda Mudzingwa and Jennifer E Ayton in Chronic Illness
Supplemental Material
sj-docx-2-chi-10.1177_17423953231163450 - Supplemental material for Acceptability of a peer-led self-management program for people living with chronic obstructive pulmonary disease in regional Southern Tasmania in Australia: A qualitative study
Supplemental material, sj-docx-2-chi-10.1177_17423953231163450 for Acceptability of a peer-led self-management program for people living with chronic obstructive pulmonary disease in regional Southern Tasmania in Australia: A qualitative study by Innocent Tawanda Mudzingwa and Jennifer E Ayton in Chronic Illness
Footnotes
Acknowledgements
The authors wish to thank the patients who volunteered their time and stories for this study, and the Royal Hobart and New Norfolk Regional Hospitals. The research was part of the research promotion and partnership initiative between Tasmania Health Service and the University of Tasmania. They wish to thank Professor Roger Hughes for his leadership in developing the partnership.
Contributorship
Authors 1 and 2 designed and conducted the study. Data collection was undertaken by Author 1, and the analysis was done by Authors 1 and 2. The manuscript was written by Author 1, reviewed, and edited by all named authors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data sharing statement
Due to the nature of the data (audio recordings and transcripts), we are not able to share the raw data.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient consent for publication
Signed consent. Patient details not identifiable in report.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.