
Abstract
Objectives
This study aimed to explore the practice-representation links among Health Care Professionals (HCP)s practising Therapeutic Patient Education (TPE). Understanding these links might actually help to address the challenges of TPE implementation, particularly the patient-centred dimension.
Methods
A qualitative study using individual interviews was conducted with HCPs practising in French-speaking Belgium or in France. Data analysis was carried out in two steps: to draw up a typology of educational practices (including variations) and, in line with the Social Representation Theory, to identify possible related social representations.
Results
The typology, based on HCP-Patient power distribution, was built from 26 interviews. Four types and nine subtypes were identified. Besides the power distribution, practice (sub)types were also specific regarding communication modes, consideration for patients’ representations, motivational approach, personalization, complexity of methods and learning contents, and practice reflexivity. Practices were seldom constant. Three variations were highlighted: within a subtype, between different subtypes, and between education and technical care. Both practice subtypes and variations were related to specific decisive representations.
Discussion
Representations related to practices and those related to practices variations offer new perspectives for TPE implementation. There is no panacea for achieving more patient-centred approaches; tailored strategies based on practice subtypes are needed.
Keywords
Introduction
In recent years, a large body of literature has highlighted the difficulties encountered in implementing Therapeutic Patient Education (TPE).1–6 TPE is defined as a process that “should enable patients to acquire and maintain abilities that allow them to optimally manage their lives with their disease. It is therefore a continuous process, integrated in health care. It's patient-centred (…). It is designed to help patients and their families understand the disease and the treatment, cooperate with health care providers, live healthily, and maintain or improve their quality of life”. 7 One of the challenges for TPE implementation is addressing the “patient-centred” dimension. TPE was frequently reported as focusing on Health Care Professionals (HCPs)’ needs.1,2,6 The Heath Care Professional (HCP) involved the patient insufficiently in information exchange1,6 and decision-making, 1 or communicated biomedical aspects only3,6 without consideration for lay knowledge and psychosocial factors, 5 whereas collaborative 4 and patient-centred 3 approaches should be encouraged. Difficulties in integrating such practices into care routines were also reported. 2
HCPs’ representations might constitute a promising avenue for a better understanding of the difficulties in achieving the patient-centred dimension. If the representation-practice link is established on a theoretical level, only two studies8,9 in TPE explored this link and measured the quality of practices, as a recent literature review 10 showed. However, as long as what the HCP does when he/she educates is not specified, it remains impossible to draw lessons for practice. This review also highlighted that TPE practices were not constant. The extent to which representations contribute to variations would be interesting to explore.
This study uses the Social Representation Theory 11 in particular Abric's approach 12 to investigate the links between educational practices among HCPs and their representations. Representations are “a form of socially elaborated and shared knowledge, with a practical aim and contributing to the construction of a reality common to a social group” 13 or “schemas or sets of cognitions about the subjective experience. (…) Other terms for this construct include explanatory model, mental model, narrative, perceptions and beliefs”. 14 According to Abric, 12 in a given situation one of the four components of the representation of the situation (i.e. Representation of themselves, of the other, of the context and of the task) becomes predominant and leads to a behavior/practice.
This study aims to explore the practice-representation links in TPE, in two steps, consisting of: providing an overview of actual TPE practices (including variations) and examining possible representations in relation to these.
Methods
A qualitative approach, via individual interviews with the HCPs, was used to describe their TPE practices and possible related representations. The research programme was approved by the Ethics Committee of our research institute (project 24/2012).
Participants
The inclusion criteria were to: (1) practise as an HCP, (2) currently implement educational practices with patients, (3) understand and speak French and (4) agree to be interviewed individually. Given the possible variety of TPE practices, any practice the participant referred to as TPE was considered as such. HCPs from Belgium and France were included to ensure diversity of the sample. Potential participants were identified on the basis either of a list from a TPE training organization or their designation as “patient educators” by TPE specialists from their institution. Potential participants had given their prior consent for their details to be shared for research purposes. No disagreements were mentioned. The research team phoned them and offered to take part in the research. They were then free to accept/decline. All participants provided verbal informed consent. Interviews took place in an office at their workplace, at their request
In line with the data saturation principle, 15 interviews were conducted until further interviews no longer add to the conceptual framework.
Data collection
Semi-interviews were conducted by the first author, on the basis of an interview guide. Interview themes were: an actual TPE practice, the representations regarding TPE, the representations at work in the reported practice, practice variations, elements linked with these variations, and socio-administrative items. Within the interviews, the “explicitation interview” techniques were used to collect the practices. An “explicitation interview” is a technique designed to elicit verbalization of a past activity. 16 It helped the HCP to move back into an educational session (i.e. a sequence of actions with patient(s)), and to focus on what he/she did.
Regarding representations, the four components of the representation of the situation from Abric, 12 (i.e. Representations of themselves as HCPs, of the patient, of the context and of the task), shown as relevant in TPE, 10 structured the interview guide. Subcategories of the educational task representation were based on the model of Deccache, 17 which explains compliance with chronic disease treatments (health and health behavior objectives; the HCP-patient relationship; education goals). Links were built on the basis of the participants’ rationales for their practices. A validation was carried out with the participant during the interview. Interviews were audio-taped and fully transcribed.
Data analysis
Data analysis took place in two steps:
- Step 1. Elaborate a typology of educational practices. The interactions of the HCP with the patient (what he/she did and what the patient did) were retraced for various contrasting practices. A common criterion for ranking practices regarding patient-centredness was subsequently identified, namely the power distribution between the HCP and the patient. Since this criterion is shared with the models of Szasz and Hollender,
18
later supplemented by Botelho,
19
the proposed classification drew inspiration from these models. Szasz and Hollender
18
provided three models of the HCP-Patient relationship: (1) Activity-Passivity; (2) Guidance-Cooperation; (3) Mutual Participation. Botelho
19
added a fourth model: (4) Autonomism “in which the patient is exerting greater control over and responsibility for health care” than the HCP (p.212). A (sub)type was assigned to each interview on the basis of the (sub)types definitions. - Step 2. Identify the predominant/decisive representation in the reported practice.
In case of doubt, attribution was carried out by two reviewers independently (SR, BG). Disagreements were resolved through discussion. Regular meetings between the authors were held to ensure the quality of the coding categories and to validate each step.
Results
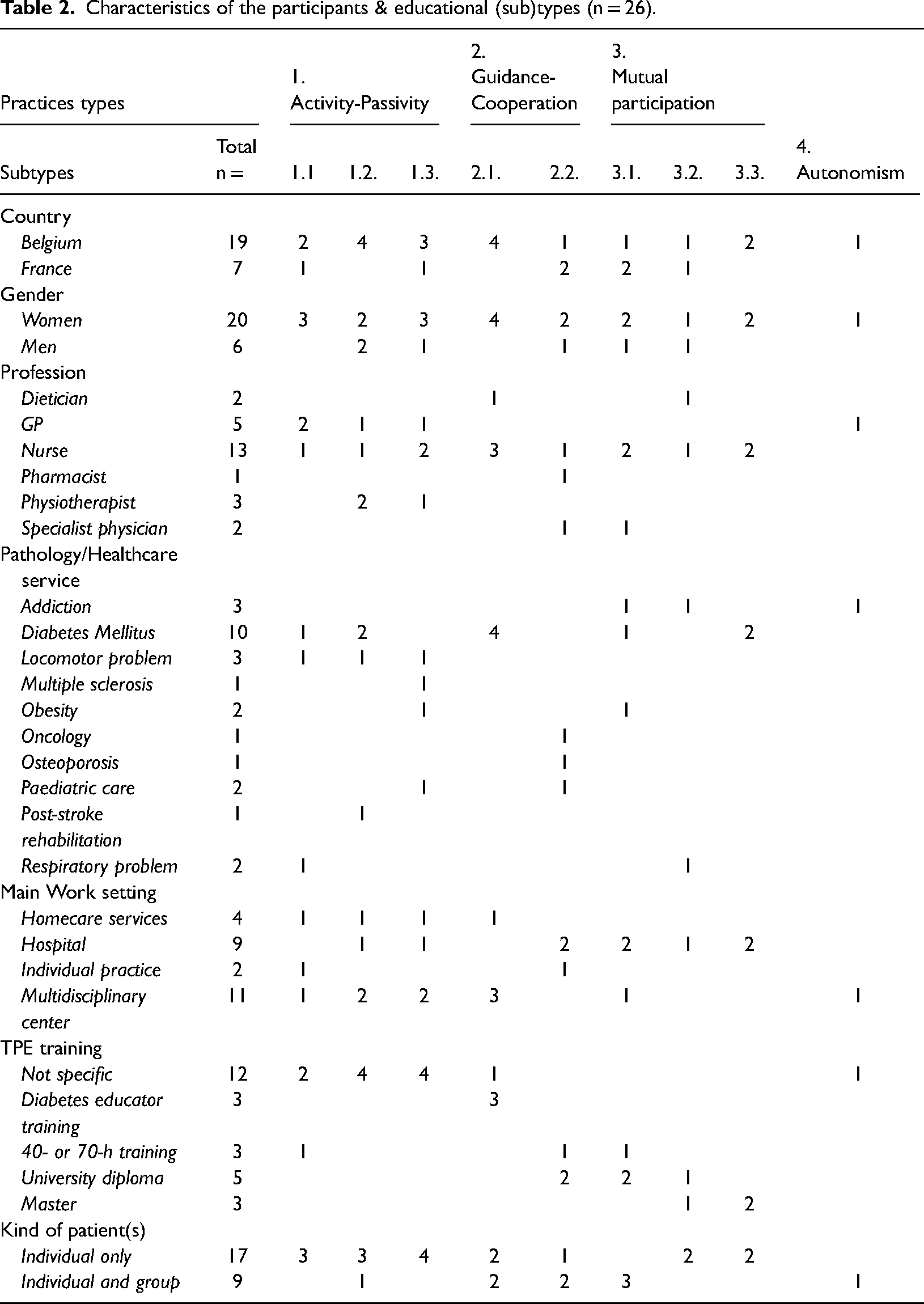
Of the forty-one HCPs contacted, thirty met the inclusion criteria. Three refused to participate in the research, four no longer had contact with patients and four others wanted to be interviewed in pairs. Twenty-six of the remaining thirty referred to an actual practice and were selected for an in-depth analysis; four could not report any. They had either no TPE training or a 40-h training course. Of the remaining twenty-six, nineteen worked in Belgium. Twenty were women. Thirteen were nurses, seven medical doctors, three physiotherapists, two dietitians, and one a pharmacist Experience in TPE was 12 years [3;26] on average. Training in TPE was diverse, ranging from no dedicated training (n = 12) to a master's degree (n = 3), a 40-to-70-h training course (n = 3), diabetes-educator training (n = 3), a 300-h university diploma (n = 5). TPE was mainly one-to-one, even though nine HCPs performed both one-to-one and with groups. While the most frequently reported practice concerned diabetes (n = 10), practices were varied (locomotor problems, multiple sclerosis, obesity, oncology, osteoporosis, pediatrics, post-stroke rehabilitation and respiratory problems). Interviews lasted 75 min on average.
The presentation of the results is as follows: TPE practices and possible related representation(s), followed by variations in practices and possible related representation(s).
TPE practices and their related representation(s)
Beyond the four practice types of the models of Szasz and Hollender 18 and Botelho, 19 adopted during the analysis, nine subtypes were highlighted. Each practice subtype came with its decisive representation (see Table 1). Table 2 provides an overview per practice subtype of the participants’ socio-demographic characteristics.
Typology of therapeutic patient education practices and decisive representations.
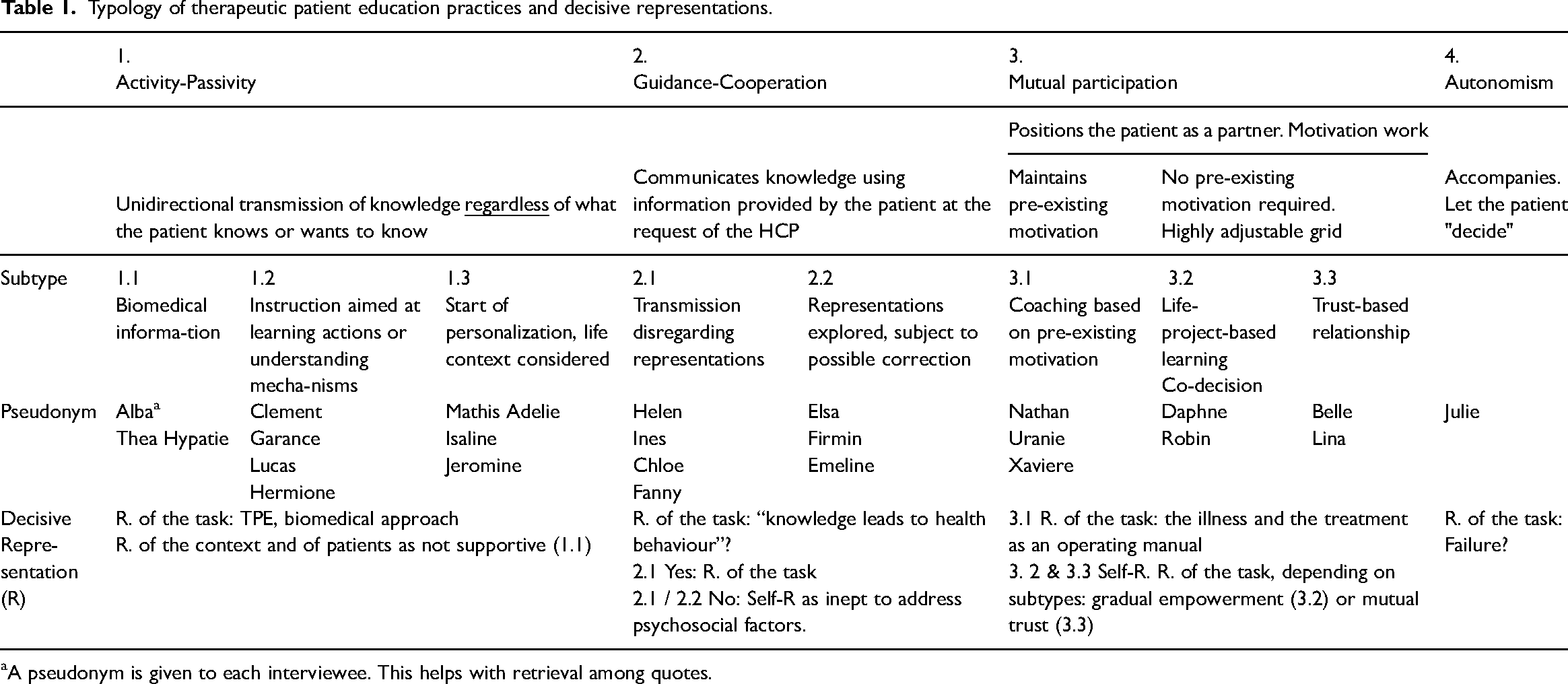
A pseudonym is given to each interviewee. This helps with retrieval among quotes.
Characteristics of the participants & educational (sub)types (n = 26).
Type 1: Activity-Passivity and Decisive Representation(s)
The HCP delivered theoretical knowledge, regardless of what the patient knew or wanted to know. Transmission was unidirectional. Three subtypes were noted: information only (1.1), instruction (1.2) and start of personalization (1.3). Practitioners’ reflexivity was low. Many relaunch questions were necessary to prompt them to report an actual practice, a characteristic shared with the HCPs who could not report any.
Regarding representations, task representations were often linked to a lack of knowledge of what TPE is. Most of these HCPs had no training courses dedicated to TPE.
Subtype 1.1 information only and their representation(s)
The HCP displayed knowledge or listed behaviors to be adopted, but did not systematically include the rationale. Information was limited to physical health. She was relatively happy to learn that she could have epistaxis, that she could bleed much longer. (Alba, home nurse)
Regarding representations, two patterns were observed, depending on the HCP's experience of a patient-centred TPE and training profile. Without this experience, TPE representations prevailed. “TPE” was understood as either transmitting biomedical knowledge or facilitating the patient's health behaviors by carrying out administrative procedures on his/her behalf. Patient education is: I explain to you and I give you the shot. (Alba)
With a training in TPE and this experience, representations of the context and of patients, as not supportive of TPE prevailed. The context gradually discouraged the HCP from implementing TPE.
Subtype 1.2 instruction and their representation(s)
The HCP transmitted knowledge to help the patient learn an action or understand a mechanism. When teaching a technical action, the HCP demonstrated it, had the patient do it, and corrected it, until it was done properly. Starting from this subtype, knowledge delivery used various sensory channels. Metaphor or imaginary clinical cases were also reported. I showed them how to put on the immobilization scarf and how to transfer the patient (from a chair to a physiotherapist's table). They did it with me. I corrected them two or three times. Then, they understood, they were able to do it again the next day. (Clement, physiotherapist, post-stroke rehabilitation)
Regarding representations, representations of health behavior objectives and of the mechanism for achieving them (task representations) characterized these HCPs. So that the patient self-administers the treatment in day-to-day life, they transmitted knowledge or know-how “ready to be implemented”, as “knowledge leads to behavior”. I’ve won when I don't see them for years because they’ve understood how to cure themselves (…). It's ignorance in quotes that makes [it impossible]. (Lucas, physiotherapist)
Subtype 1.3 start of personalization and their representation(s)
The HCP used aspects of the patient's life context and lifestyle to communicate knowledge. Contextual information was, however, rarely collected for educational purposes.
Regarding representations, life context was factored in, thanks to long-term or home-based follow-up, which allowed it to be observed. Some HCPs reported being unsure of practising TPE or confused TPE with approaches such as pain management through medication.
Type 2. Guidance-Cooperation and Decisive Representation(s)
Prior to education, the HCP considered elements (knowledge, technical actions, lifestyle habits) provided by the patient, at the HCP's request Lifestyle habits and knowledge were addressed differently. Habits were used to personalize education. Knowledge was checked for accuracy and corrected, if necessary. Learning methods were collaborative and even game-oriented. Two subtypes can be distinguished depending on whether or not they explored patients’ representations.
Regarding representations, emotional or motivational aspects (task representation) might generate discomfort among these HCPs.
Subtype 2.1 transmission disregarding representations and their representation(s)
Rationales for health behavior were systematically set out.
Regarding representations, two patterns were observed, depending on their awareness that knowledge might not be sufficient to change behaviors (task representation). Without this awareness, the HCP communicated knowledge in the way he/she likes to learn (e.g. memos, handling, color codes) as “knowing leads to acting accordingly”. When patients did not implement what they learned, HCPs were unable to work out the reason why. “When you eat French fries, does it raise your glycaemia, your sugar level?” “Yes, Ma’am”. They always say: “yes”. “Why?” “Because they’re greasy!” (…). 8 times out of 10 they’re wrong. Even though I’ve just explained, and they’ve understood that there was sugar in potatoes. (Chloe, dietitian, diabetology)
With this awareness, self-representation as unskilled in psychosocial factors (e.g. self-efficacy, perceived social support) was decisive. This might be reinforced by unsuccessful experience of training intended to remedy this. Professor Z talked to us about metaphors. He really likes metaphors. But I don't know how to make them (…). He gave us an example. Coversyl®, the blood pressure medication, “is the rose of a watering can”. (…). I’m still trying to figure it out. (Helen, nurse, diabetology)
Subtype 2.2 transmission “with awareness of” representations and their representation(s)
After their collection, representations were confronted with scientific facts in order to be “corrected”. We have to try to reframe people's beliefs. (…) About milk, there are a lot of beliefs, more or less false. (Firmin, rheumatologist, osteoporosis)
Negotiation was limited to dimensions (e.g. lifestyle habits, alternative treatment) that were not deleterious to the proposed treatment.
Regarding representations, emotions and motivation were found to be relevant in TPE (task representations). However, the HCPs did not feel competent to address them (self-representation). A very ambiguous back and forth, about the disease (which is not my field) and “I’m screwed”. I delivered all the messages I had to (…). I left the room and told one of the assistants: “I feel bad, I’m afraid she’ll do something stupid.” (Elsa, pharmacist, oncology)
Context representations might increase or decrease this discomfort, depending on the representation of being part of an interdisciplinary team. If so, emotional/motivational aspects were seen as other HCPs’ task (doctors, psychologists). If not, the HCP reported acting “like a wart” (Elsa), an interloper who is not part of the team.
Type 3. Mutual participation and Decisive Representation(s)
Education started from pre-existing knowledge, skills and representations. Active methods (e.g. reformulation, echoing, questions left opened, silences) were used to support the patient's expression and mental elaboration. Motivation and psychosocial factors were part of education. Some HCPs developed strategies to implement Type 3 despite contexts that gave little room for personalization (e.g. standardized procedure, penitentiary settings). Strategies were: initiating personalized sessions after a standardized diagnosis or group sessions, meta-communicating on the context, … Three subtypes were noted. They constituted the shift from HCP-centred approaches (3.1) to patient-centred approaches (3.3). The patient's objectives gradually took precedence even if the HCP had their own.
Regarding representations, self-representation was key in 3.2 and 3.3, but peripheral in 3.1.
Subtype 3.1 “coaching” based on pre-existing motivation and their representation(s)
Methods were “predefined” by the HCP. Pre-existing motivation could be assessed to estimate whether the conditions (e.g. internal motivation, Prochaska's “contemplation” stage) were in place to optimize the TPE success rate. Negotiation applied as long as the vital prognosis was not engaged. Metaphors tailored to the patient can be used. The forklift driver, I’m going to tell him: “Listen, your lungs are like the oil filter, you put in good quality oil, but you’ve never changed the oil filter, after a while it doesn't work anymore”. (Uranie, nurse, tobaccology)
Regarding representations, the task representation that “a technique addresses a health problem” was decisive (e.g. emotional awareness for eating disorders, Prochaska model for smoking cessation).
The Prochaska wheel is wonderful, isn't it? Based on his/her motivation, we act differently. (Uranie)
Subtype 3.2. Life-project-based learning and their representation(s)
The HCP assisted the patient to gradually gain autonomy including in making health choices. The HCP helped the patient's “life project/objectives” to emerge through interrogative methods. Education was structured based on the life project. Motivation was stimulated in this way. Knowledge and know-how transmission were not a priority unless the patient asked for it. Representations could be deconstructed by encouraging the patient to adopt dissonant behavior. “What does oxygen mean to you?” “A thread.” “A thread. But what will it do for you?” The guy says: “Dig my grave” (…) “You’re at stage 4, that's true, but you might still want to do something… this month, this week, or this year, whenever you like…. What would it be?” “I’d really like to play the drums again!” “That's a great goal, let's go for it! What would be needed so you can play the drums again?” “I’ve got no strength left” “OK”. At that point, you really have to dig down, to rephrase: “How could you get more strength?” “I’d have to lift weights.” “Not weights, they’re a bit heavy at the moment. (..) First, it would be walking.” “Yes, but I can't walk anymore!” “Why can't you walk anymore?” “Because I walk 2 metres and I’m exhausted!” (…) “Do you think it's a need for air or for oxygen?” “I don't know the difference!” “Do you want us to experience the difference?” “Yes!” So, I get my oxygen tank and say: “Here we go, we’ll do two tests. One with oxygen, one without. We’ll see when you’re best”. (Daphne, nurse, COPD).
Regarding representations, self-representation was central in subtypes 3.2 and 3.3. TPE values were perceived as matching those of the HCP. The freedom to determine life choices was a central value for subtype 3.2. TPE contributed to it through gradual empowerment (task representation). Whereas values were perceived as defining the HCP, the training equipped him/her. These HCPs completed the longest TPE training courses. I think it comes from one's value system: it would be very arrogant to claim I know what others need to do. (Robin, dietitian, addictology).
Subtype 3.3. “Trust-based relationship” and their representation(s)
The prior health problem was the one the patient considered as such. His/her reading grid of a phenomenon was accepted as “true”. The HCP tried to get to the root of the problem by questioning. Health behavior objectives and possible learning were “co-decided” in light of what was possible for, and desired by, the patient. Those were her goals, the goals she felt she could achieve. I didn't come along and say: “You’d have to stop after 3-4 drinks”. (…) It was a discussion. (Lina, nurse, diabetology)
Regarding representation, the specificity of subtype 3.3 is that trust was key, to achieve a successful follow-up (task representation). Given the trusting relationship that has been established, if there was another major problem with diabetes (…) the fact that we know each other well would facilitate the follow-up. (Lina)
Type 4. Autonomism and Decisive Representation(s)
Education was put on hold. The HCP suggested health behaviors based on her/his feelings and representation of the patient's feelings. She/he discussed them with the patient and let her/him decide. The HCP stood alongside the patient. His blood test, it's true that's something I don't always bring up because I know it's going to tire him out, that he knows that (laughs) and I know he knows it. (Julie, general practitioner)
Regarding representations, task representation seemed to be decisive. Mobilizing the patient failed; the HCP redefined the objectives as well-being and maintenance of the patient's connection to the health care system. I believe that by maintaining this dialogue and leaving the door open, maybe one day he’ll be ready and he’ll come back. (Julie)
Practice analysis highlighted a range of educational practices, differing in terms of HCP-Patient power distribution, but also on other aspects, namely: communication mode, consideration for patients’ representations, motivational approach, personalization, complexity of methods and learning contents, and practice reflexivity (see Table 3). Specific representations were related to each (sub)type which might shed light on this practice diversity. Regarding patient-centredness, mutual participation – the patient-centred approach in which the HCP still has a role to play – was not mainstreamed among our participants.
Characterization of educational practices subtypes .
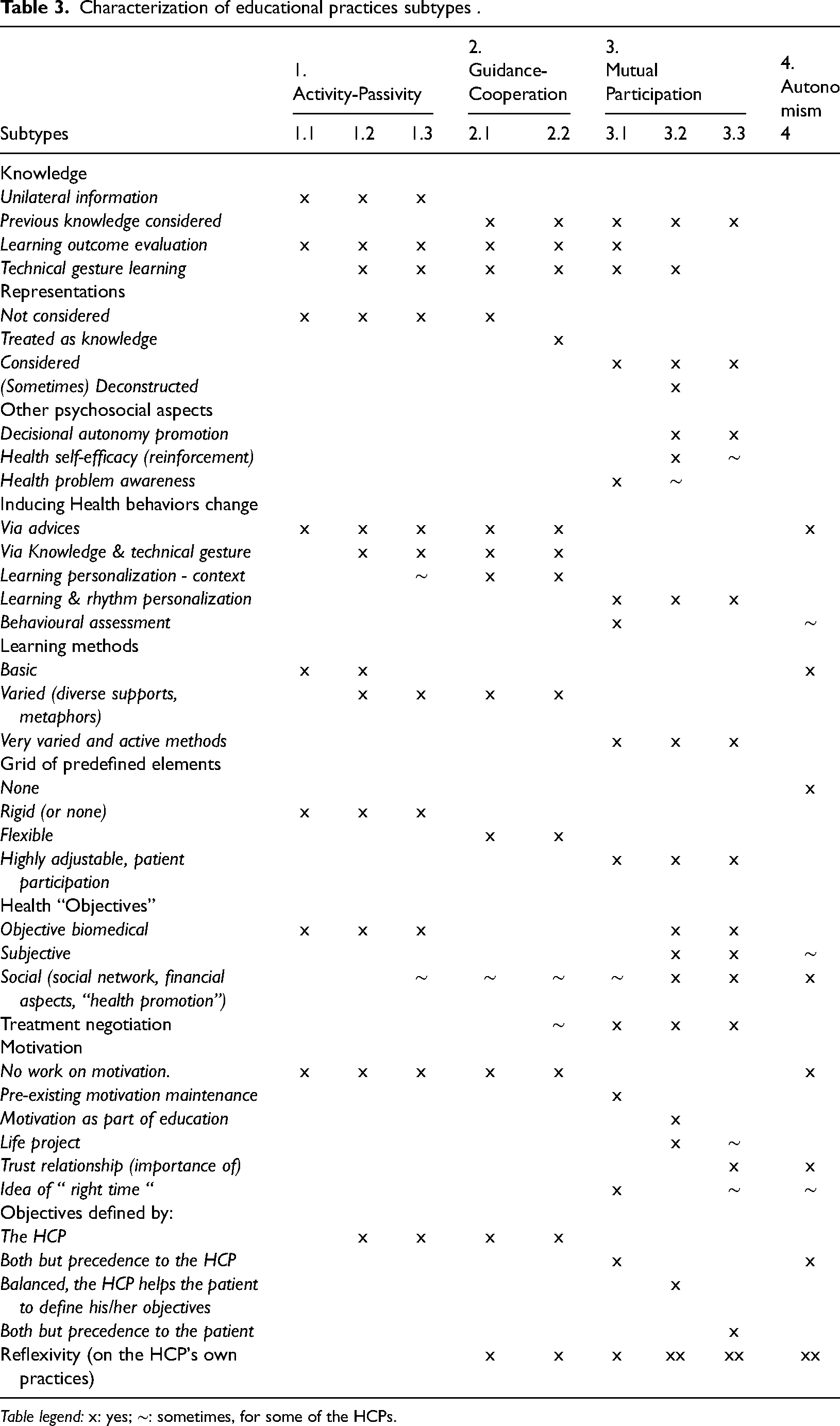
Table legend: x: yes; ∼: sometimes, for some of the HCPs.
Were these practice (sub)types immutable? Abric 12 suggests practice variations should be considered. Given that a representation becomes predominant in a given situation, the decisive representation might vary and so might the related practice.
Variations in Practices and their Related Representations
Practices could vary within an HCP in three ways: within a subtype, between the subtypes and between technical care and education. Some decisive representations seemed to be related to these variations.
Variations within a subtype and decisive representations
All participants except Firmin, Hermione, Isaline, and Nathan reported such variations. It consisted in using different contents/methods while remaining in the same practice subtype. These variations were related to representations of the patient experiencing learning difficulties. Difficulties were perceived as being associated with patients’ characteristics: eagerness to learn, intellectual level, ethnic origin, age, vehicular language mastery, illiteracy, social class, prior knowledge, psychiatric disorders and precariousness. Adaptations were made to enable learning: simplified vocabulary, information quantity adjustment, pictorial aids, content reordering, … Sometimes I only use pictures. I’ve a food plan in pictures, because I’ve illiterate persons. (Chloe)
The availability of the HCP (in terms of physical condition and time available) was also associated with information quantity adjustment. If I’ve slept well, if I’m on top form, I’ll explain everything (Laughs). (Alba)
Variations between Subtypes and Decisive representation(s)
Some HCPs (Belle, Firmin, Hermione, Julie, Lina, and Xaviere) reported variations between practice subtypes. These were related either to representations of the context or to representations of patients.
Shifts from 1.1 to 2.2 aimed to compensate for the usual length of consultations; HCPs engaged in group education to go into further explanation. Here, we have to do things quickly. We tell them if their treatment is appropriate or not, it's a whole process: X-rays, blood tests… Once we’ve done all that, the time is almost up (…). There, we spend a whole afternoon with them so that they can ask any question they like. (Firmin)
Shifts from 1.2 to 2.2 were linked to the availability of another HCP who provided this kind of education. Once we realized it was a total misunderstanding, I suggested the nurse go to his home every day to observe what was going on, how he pricked his fingertips, how he understood his illness and how he administered his treatment. (Hermione, general practitioner)
Shifts from 3.3 to 2.2 were linked to the prescriber's request to meet the objectives quickly or to an influx of patients, preventing the HCP from taking the necessary time. When there are three patients in the waiting room, it's sometimes harder to take the time. (Lina)
Shifts from 3.1 to 2.1 consisted of temporarily adopting a “directive style” to meet the patient's wishes. “I have to take my Lantus® when I go to bed, around midnight.” So, we need to make sure learning takes place because schedules are incompatible with normal nursing care (…) The question was: “What's essential right now?” (Xaviere, nurse, diabetology)
Shifts from 4 to 3.1 were linked to the patient's possible remobilization (e.g. Type 4 and their representations).
Technical care versus education and decisive representation(s)
Some HCPs of (sub)types 1.2, 2.1, 3.3 and 4 (Garance, Hermione, Fanny, Helen, Lina, and Julie) reported practising education on some occasions and purely technical care on others. Various representation type could be at work:
Representations of the patient as meeting the educational criteria (physical or intellectual abilities, motivation, vehicular language fluency); Sometimes we provide only care because people don't ask for education (…). When people start to know us better and ask questions, we start educating them. (Garance, nurse, diabetology)
Representations of the context: the policy of the health care service regarding education or a medical prescription that specified “education”; On Thursdays I’m in charge of the diabetic foot clinic. We do very little education because it's basically wound care. It's therapeutic. Even though we should also provide education (…) On Fridays, I have a small office close to the doctors’. (…) If there is an issue with their diabetes, no matter what, the door is open. (Lina)
HCPs’ self-representations as being “on top form”, which is perceived as essential to educate. Care takes… I wouldn't say very little energy… but less energy than educating the patient. You need energy to repeat the same thing sometimes 3 to 4 times. Whereas I can visit patients with 40°C [104°F]. I tell them: “I’m not well today”. They leave me in peace. (Helen)
Discussion
Main findings and existing literature
This research aimed to explore representation-practice interactions in TPE in order to understand the difficulties in shifting towards more patient-centred practices in a mutual participation perspective. Of the thirty HCPs interviewed, four were unable to report any actual educational practice. This trend is also mentioned in the literature, by Vigil-Ripoche, 20 who identifies the lack of reflexivity as a barrier to practice conceptualization (i.e. putting practices into words), which in turn impedes a shift towards more patient-centred practices.
The typology of practices emerging from this study reflects the “power distribution in the HCP-Patient relationship”.18,19 At one extreme (Type 1), the power is held by the HCP who tells the patient what to do; at the other end (Type 4), the power is left to the patient. While the typology of TPE practices is not, as such, novel, its originality lies in offering an empirical exploration of the theoretical models of Szasz and Hollender 18 and Botelho. 19 Besides the types, the proposed typology also includes many subtypes. According to Szasz and Hollender, 18 the HCP should adapt his/her relationship to the patient in the light of the patient's health condition. They pointed to “mutual participation” as the appropriate type of relationship for chronic conditions, to “help the patient to help himself/herself”. Most of the practices reported were HCP-centred, however, and limited to knowledge transfer (18 out of 26 are at best type-2 practices). These results are consistent with the literature on representation-practice links in TPE. 10
The training profile of the HCPs in TPE seems to play a decisive role in this low rate of patient-centred practices. In Type 3-Mutual participation, six out of seven had a university diploma, whereas those who had no specific training were mainly in Type 1. However, training is not the whole story. The same kind of training (40-to-70 h) was linked to different practice types (1, 2, 3, and even a failure to report practice). So, apart from training, what characterized the various practice types?
Results showed that each educational (sub)type was linked to a decisive representation. Representations related to mutual participation (Subtypes 3.2 and 3.3) did not contribute much to understand difficulties in implementing TPE: they were self-representations which may have been reinforced by a feedback loop. Representations related to other (sub)types help more: a fragmented representation of what TPE is (Type 1), the representation that knowledge leads to behavior change (Subtype 2.1) or the self-representation as incompetent in approaches that go beyond transmitting knowledge (Subtype 2.2). Subtype 3.1 was therefore enlightening: the first stage of mutual participation was linked to task representations setting out a procedure to be used to manage a specific health problem. Context representations had a particular status. They were at work in practice variations only.
Practices were not stable over time. Three kinds of variations were uncovered: variations within a subtype, variations between subtypes, and the presence/absence of educational practice. The variation phenomenon has previously been highlighted in the TPE literature on representation-practice links among HCPs. 10 Previous research, however, concerned a single kind of variation: either variations within a subtype 8 or variations between subtypes. 9 Variations between educator and caregiver in TPE have also been highlighted in the past. 21 The spectrum of variations observed in this research was hence more comprehensive. Variations seemed to be related to specific representations. Comparison with previous research is, however, challenging for two reasons: (1) The diversity of variations emerged from the present research. It could not be systematically explored with all the participants; (2) One single piece of research 9 analyzed actual practices and their related representations, and therefore allows of a comparison. Karlsen 9 analyzed variations between two (sub)types (standardized information transmission vs. personalized education). Although the number of types differs, both Karlsen 9 and this research point to the importance of context and patient representations in variations between (sub)types.
But were variations detrimental to, or supportive of patient-centred approaches? Variations consisted primarily in either an adjustment to the patient's level of understanding (variations within a subtype) or the implementation of an education approach aiming at more mutual participation (variations between subtypes). In this latter case, the practice itself could be closer to mutual participation, or temporarily more directive in order to achieve co-decided objectives. As a result, part of variation tended towards more patient-centred practices. There were, nevertheless, two notable exceptions: when the context is perceived as not supportive of TPE and when TPE is perceived as requiring more effort and specific implementation conditions (in the framework of HCP-centred practices).
Strengths and limitations
The two main contributions of this exploratory research were: (1) to propose a typology of actual educational practices and related representations; and (2) to highlight three types of practice variation, which also appear to be related to specific representations. It also has some limitations. Practices were self-reported and therefore subject to social desirability. Being qualitative in nature, the findings cannot be generalized. In addition, the study's cross-sectional design excludes causal relationship.
Implications for research and clinical practice
This research offers new perspectives both for research and for TPE implementation.
Regarding research, examining representation-practice links did help to better understand what hinders the deployment of patient-centred practices. Explanatory interviews were also pointed up as a valuable technique for exploring TPE practices, since they help to solve problems of lack of reflexivity. Further research, on a larger scale, is needed to address the following questions: What is the prevalence of each (sub)type? What is the status of Type 4 (a progress in power distribution, a fallback position)? Data collection methods also need to be diversified (pair/group interview, observation, document analysis) to go beyond self-reported practices.
Regarding TPE implementation, both representations related to practices and those related to variations offer perspectives. Firstly, when the HCPs’ practices were not in line with mutual participation, neither were their decisive representation(s). However, the representation(s) at work differed from one subtype to another. There is therefore no panacea to achieve/maintain patient-centred approaches. The practice (sub)type needs to be borne in mind to provide accurate support (e.g. For Types 1 and 2, training on knowledge and representations regarding TPE. For Type 2, training on patients’ representations and motivational levers. For Type 3, intervision). Secondly, the variations towards less participatory approaches emphasized the importance of the context representations. Addressing HCPs’ competencies is not enough; organizational contexts promoting patient-centred education are essential.
Footnotes
Acknowledgements
We would like to express our gratitude to all the research participants and their institutions for their enthusiasm and sincerity. We are most grateful to Bertrand Gollion (BG) for his valuable contribution to the data analysis, particularly the development of the practice typology. We also thank Jonathan Dedonder for his methodological input advice to ensure proper terminology in qualitative research and validity throughout the research.
Contributorship
SR and MF contributed to the conception of the study. SR and MF held regular meetings and each key step was discussed and agreed upon. Selection of the conceptual framework and development of the typology of practices were carried out collaboratively by SR and MF. SR developed the study protocol (and the interview guide) and conducted the interviews. She carried out data analysis (with the assistance of BG - see acknowledgement - in case of doubt regarding attribution). SR wrote the first draft of the manuscript. All authors reviewed and edited the manuscript. They approved its final version
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The research programme was approved by the Ethics Committee of the Research Institute of Psychological Sciences, from the Université catholique de Louvain (project 24/2012). It also received the approval of the Hospital Care Direction whenever necessary.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent and individual details
Based on a document sent in advance, verbal informed consent was obtained from each professional before the interview for their anonymized information to be published. They also provided verbal consent to be audio-recording. The authors confirm that all personal identifiers have been removed or disguised so that the persons described are not identifiable and cannot be identified through the details of the story.
Materials and data availability
The interview guide is available on request (in English and French). The action sequence analysis of the practices (words files) and the data analysis tables (excel files) are available from the corresponding author on reasonable request All this material is in French. The full data sets and transcripts are not publicly available. Due to the small number of patient education practitioners in Belgium, individuals could be identified, even if the data are anonymised. It would not be possible to guarantee the confidentiality of the data.
Trial Registration
Not applicable, because this article does not contain any clinical trials.