
Abstract
Objectives
Fibrous dysplasia is a rare bone disorder that causes deformity, fractures, and pain that typically manifests in childhood and persists as a chronic illness. This study evaluates adult patients with fibrous dysplasia and McCune Albright syndrome to determine whether their quality of life differs from the general population and varies in relation to disease severity and lesion location.
Methods
This study uses data from the online self-report Fibrous Dysplasia Foundation Patient Registry and operationalizes quality of life using PRO measures: SF-36, Hospital Anxiety and Depression scale, Neuro-Quality of Life Stigma scale, and the Brief Pain Inventory.
Results
One hundred and ninety seven adults, 90% white, 84% women, constitute the sample. Mean scores for all SF-36 domains and the Neuro Q stigma scale were significantly below population benchmarks. A large minority registered moderate to severe levels of anxiety and depression. Group differences were not significant across most of the SF-36 domains but were associated with experienced stigma.
Discussion
This study demonstrates a social psychological impact of fibrous dysplasia on adults, in those with and without craniofacial involvement and with mild and severe forms of the disease. Clinical treatment should encompass assessment of quality of life issues and ensure access to psychosocial treatment resources for all fibrous dysplasia/McCune-Albright syndrome patients.
Introduction
Fibrous dysplasia (FD) is a rare mosaic bone disease caused by mutation in the gene GNAS. Normal bone and marrow are replaced by fibro-osseous tissue, which may result in deformity, functional issues, and pain. Additionally, endocrine tissues may be affected, referred to as McCune-Albright syndrome (MAS). 1 FD/MAS can also result in unwanted negative attention, discrimination, and social exclusion and FD patients may internalize a sense of deviance, experience embarrassment,2,3 anxiety, and depression. 4
The location of lesions may differentially impact the social experience of living with FD. Distortion of the bones in the trunk and appendicular skeleton may bow and fracture affecting gait, stance, and ability to move fluidly or engage in activities typical for one's age and gender. Persons with craniofacial FD (CFD) may experience expansile bone grow leading to facial asymmetry, distortion of features, hearing or visual impairment, sinus, or dental problems. 5 Growth may be outward and visible or inward filling the sinuses and encroaching on the orbits, or both. Distortion of bones in the facial region may affect interaction more than lesions in the trunk and appendicular skeleton because the face is always accessible, not covered by clothing, and may be associated with assumptions about reduced intellectual capacity. On the other hand, individuals with inward and invisible growth who experience debilitating and chronic pain may experience challenges to their claims on the patient role.2,6
Quality of life (QOL) is a growing concern of medical investigators focused on FD.2,7–9 Recently published best practice guidelines for FD care from the International FD/MAS Consortium endorsed the evaluation of QOL in FD/MAS, and encouraged the use of the SF-36 and the Hospital Anxiety and Depression scale (HADS). 10
The purpose of this study is to apply a broad definition of QOL to a nonclinical sample of adult patients with FD/MAS to evaluate whether their QOL differs from the general population and varies in relation to disease severity (monostotic vs polyostotic/MAS) and location (craniofacial vs trunk and extremities). Specifically, it seeks to determine if monostotic CFD is a “unique patient subtype within the spectrum of FD/MAS patients” in the sample. 9
Background
Exploration of QOL in FD/MAS has primarily made use of the SF-36, which has eight domains that can be reduced to two summary scores. Four physical domains include: physical functioning, role limitations due to physical problems, bodily pain, and general health. Four social domains include: energy/fatigue (also called vitality), social functioning (the degree one's interactions are hampered), limitations on role performance due to emotional problems, and mental health, a measure of emotional well-being. National Institutes of Health (NIH) investigators found that a cohort of adult and child FD/MAS patients, including those with and without CFD, exhibited physical QOL outcomes that were significantly different from the general population. 7 Studies of Dutch patients treated at the Center for Bone Quality in Leiden found that disease seriousness was significantly associated with physical and mental health QOL measures. Patients with isolated CFD scored higher (better) on QOL measures for bodily pain and vitality than all other FD patient groups. They also scored better on measures for physical function, the impact of physical function on role performance, general health, and social functioning than others with CFD and lesions in other parts of the body or a MAS diagnosis. 9 Compared to patients with polyostotic FD and/or MAS, but no CF lesions, those with isolated CFD scored better on measures for physical function and mental health. 9
Researchers identify several types of stigma that are mutually reinforcing.2,11 Enacted/Experienced stigma includes discriminatory acts against individuals or groups. Perceived or felt stigma includes discriminatory acts absorbed or anticipated by a targeted individual that may overlap with but are independent of discrimination. Self-stigma occurs when prejudicial cultural ideas about ones’ attributes or behaviors are internalized. 11 Studies of a variety of illnesses have found that perceived stigma from others and self-stigma are associated with negative mental health outcomes, including depression, low self-esteem, and self-isolation.4,11
Facial appearance differences often prompt misperceptions and undesirable judgments from others. 12 CFD patients have reported discrimination, nonverbal recoil, verbal harassment, social isolation, and rejection as well as feeling deviant and self-isolation. 2
Methods
Study design
In June 2016, the Fibrous Dysplasia Foundation (FDF) (www.fdmasalliance.org), a nonprofit patient advocacy organization, opened a patient registry (FDFPR) for individuals with FD and McCune Albright Syndrome, from birth to age 70 (www.fdmasregistry.org/). The FDFPR consists of a battery of online surveys about respondent's symptoms, treatment, psychosocial condition, and demographics. The FDF recruited participants through emails, newsletters, its website, Facebook groups, and Twitter.
Consenting protocols for the FDFPR were reviewed by New England IRB (Needham, MA) and are consistent with the Declaration of Helsinki as amended 2008. The author's university IRB determined this study to be exempt from human subjects review due to use of deidentified data. The study population consists of 197 adult individuals (117 with CFD, 80 with trunk and axial involvement), who supplied demographic, bone involvement, and diagnosis information, and completed the selected QOL measures between July 2016 and December 2018.
This study tests two hypotheses. (1) FD/MAS patients will score significantly worse than population norms on QOL, including the SF-36, Neuro-QOL stigma, and HADS. (2) QOL scores for participants with isolated CFD will be significantly better than those with CFD and polyostotic FD/MAS, monostotic FD, and polyostotic FD/MAS.
Quality of life measures
The SF36, described above, is a 36-item validated adult patient report QOL measure. Higher scores indicate better health; normed scores above 50 indicate health that is better than the general population. 13 The FDFPR incorporates Version 1 of the SF3-6, normed to 1998 population values. 13
Two items from the Brief Pain Inventory were incorporated to document the interference of pain on mood and enjoyment of daily life.
The eight-item Neuro QOL stigma short form ascertains patient's “perceptions of self and publically [sic] enacted negativity, prejudice and discrimination as a result of disease-related manifestations.” 14 Scoring the full measure produces T-scores; scores above 50 indicate stigma greater than the reference population, a clinical sample of individuals with common neurological conditions. 15
The Hospital Anxiety and Depression index (HADS) consists of two seven-item subscales that may be converted to clinical levels: 0–7 non-clinical, 8–10 mild, 11–14 moderate, 15–21 severe. 16
Patient characteristics
The study incorporated FDFPR participant's self-reported age, gender, race, and educational attainment. Participants were directed to reference lists of bones to indicate which in their body and skull were affected by FD lesions. Patients who indicated CF involvement were also asked to report on whether they had a craniofacial “deformity.” Diagnosis was self-reported as monostotic FD, polyostotic FD or FD with McCune Albright syndrome. These self-reports were cross-referenced with the bones listed. For this analysis, information about the location of lesions and bones involved was condensed into Hagelstein-Rotman and colleagues’ four-type characterization of FD: isolated CFD, CFD with lesions in the trunk and extremities and/or MAS (CFD + PFD/MAS), monostotic lesions in the trunk and extremities (MFD), and polyostotic lesions in the trunk and extremities and/or MAS. 9
Statistical analysis
Statistical analysis was performed using SPSS for Windows, version 26. Results are presented as mean (SD) or percentage, for categorical data. T-tests were used to compare SF-36 domain scores and Neuro-QOL stigma scores to general population norms. Scores on SF-36 domains, Neuro-QOL stigma scale, and pain interference items were compared between different groups using a one-way analysis of variance, with post-hoc Bonferroni correction. Scores on the HADS were compared using a Kruskal–Wallis H-test. A p<0.05 level of significance was used in all tests.
Results
Patient characteristics (see Table 1)
The sample consisted of 44 CFD cases (22.3%), 73 CFD + PFD/MAS cases (37.1%), 41 MFD cases (20.8%), and 39 PFD/MAS cases (19.8%). Respondents included 165 women and 32 men, ages 18–69 who were distributed across the decades (mean 40, SD 13.1). Almost 90% (89.9) were white. Chi-square tests established no significant relationships between participant gender, age, race, education, and the case types.
Patient characteristics in total and by FD types with p values indicating significant differences.
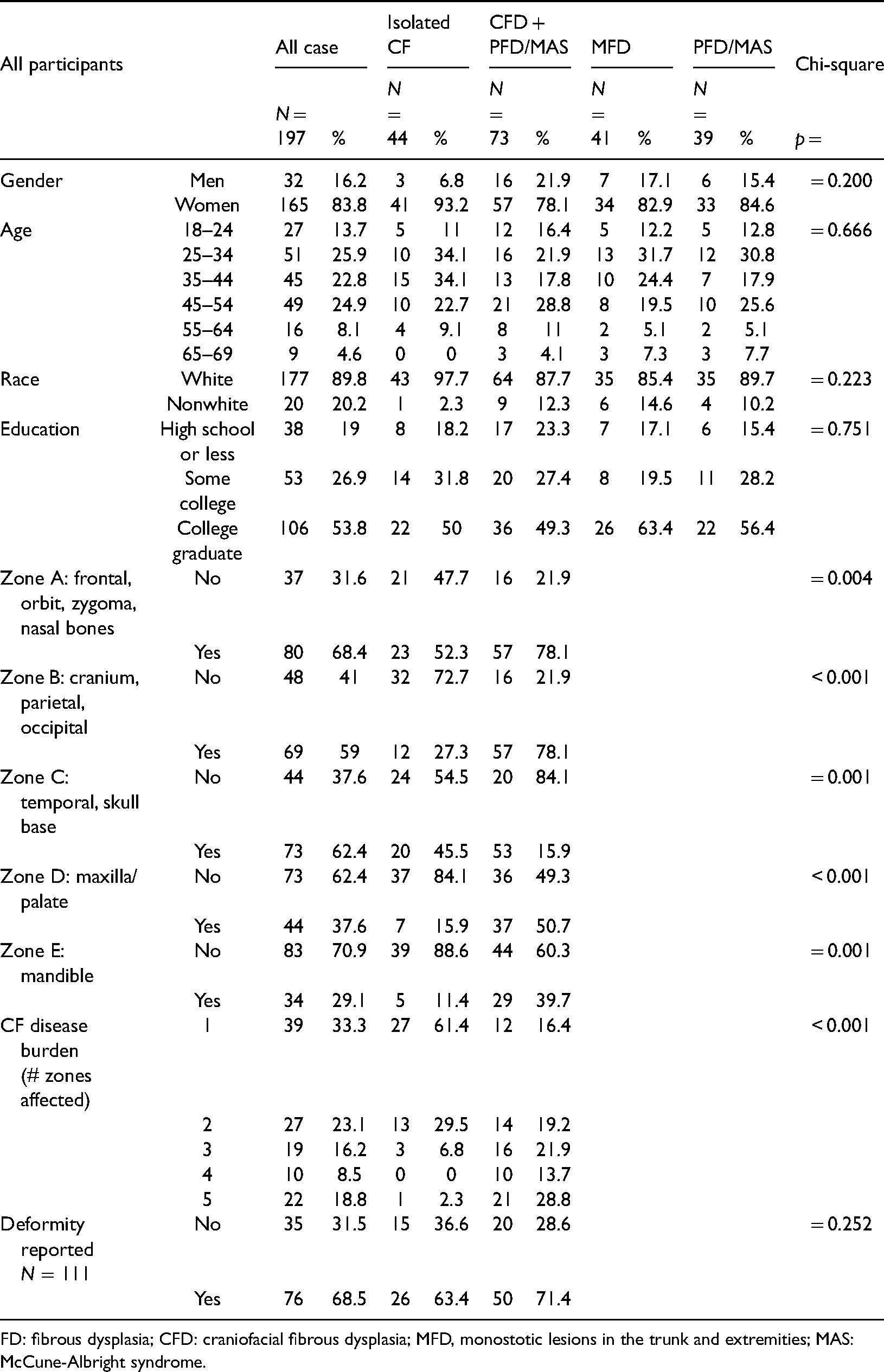
FD: fibrous dysplasia; CFD: craniofacial fibrous dysplasia; MFD, monostotic lesions in the trunk and extremities; MAS: McCune-Albright syndrome.
Craniofacial bones that FDFPR participants indicated were affected were assigned to zones in a modified version of the classification system created by Chen and colleagues: Zone A—frontal/orbit/zygoma/midface/cheek (zygoma)/nasal bones, Zone B—cranium, parietal, occipital, Zone C—temporal, skull base, Zone D—upper jaw (maxilla)/palate, Zone E—lower jaw (mandible). 17 The zones affected were summed to create a craniofacial disease burden score (1–5). Thirty-nine respondents were affected in one zone (33.3%), 27 in two zones (23.1%), 19 in three zones (16.2%), 10 in four zones (8.5%), and 22 in all five zones (18.8%). When compared, the two types of CF cases were significantly different (p < 0.001): the majority of isolated CF cases involved one (61.4%) or two zones (29.5%), while the majority of CFD + PFD/MAS cases involved more than two: three zones (21.9%), four zones (13.7%), and five zones (28.8%). Reports of perceived “craniofacial deformity” were not significantly different between CFD + PFD/MAS than CFD patients.
Quality of life outcomes (see Table 2)
Means for all domains of the SF36 were significantly (p < 0.01) below the general population reference of 50 for the sample as a whole and for all but one domain score for isolated CFD (physical function, p = 0.103). Individuals with isolated CFD scored significantly better than all other types on physical function (a mean of 47.28 vs 37.17, 39.79, and 37.51). Individuals with isolated CFD also scored better on bodily pain (44.45) than those with CFD + PFD/MAS (37.32) and those with PFD/MAS (37.24), but not those with monostotic FD in the trunk and extremities (40.14). Outcomes for the other six SF36 domains were not significantly related to the severity/lesion location grouping.
Means by FD type for SF-36 domain, stigma and pain interference with p values indicating significant differences.
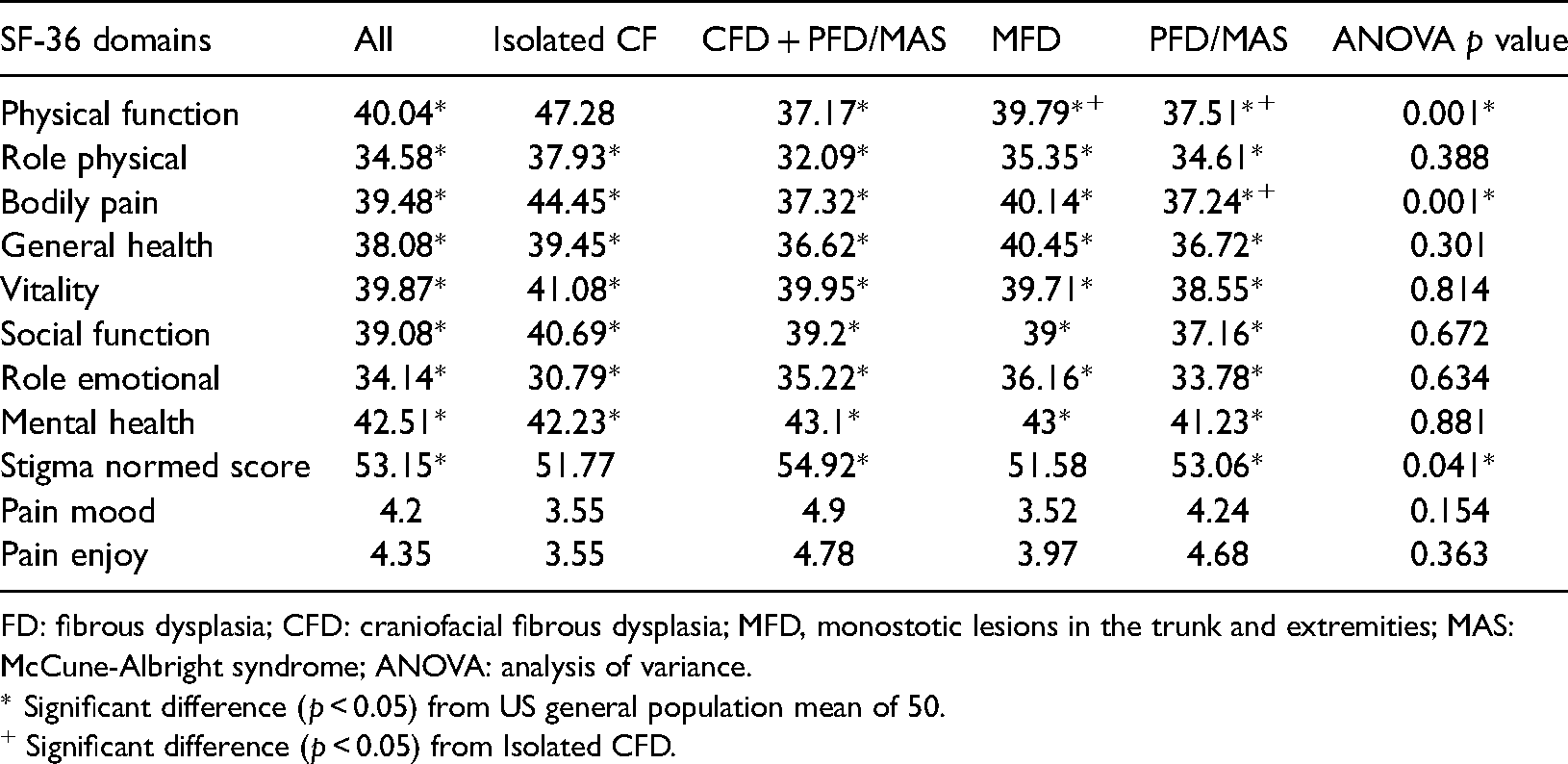
FD: fibrous dysplasia; CFD: craniofacial fibrous dysplasia; MFD, monostotic lesions in the trunk and extremities; MAS: McCune-Albright syndrome; ANOVA: analysis of variance.
* Significant difference (p < 0.05) from US general population mean of 50.
+ Significant difference (p < 0.05) from Isolated CFD.
The mean level of stigma for the entire sample (53.15) was significantly different (worse) than the clinical population reference score. Means for CFD + PFD/MAS and PFD/MAS were also significantly worse than the clinical population reference, (p = 0.001 and p = 0.006, respectively) but not for isolated CFD or MFD (p = 0.156 and p = 0.127, respectively). While stigma T-scores were significantly related to the grouping variable (p = 0.041), Bonferroni tests did not reveal significant mean difference among the types of FD.
Type of FD was not significantly related to the interference of pain on daily life among those who reported pain.
Fifty seven percent of the entire sample expressed clinical levels of anxiety, of which 35.5% were moderate or serious (Figure 1).
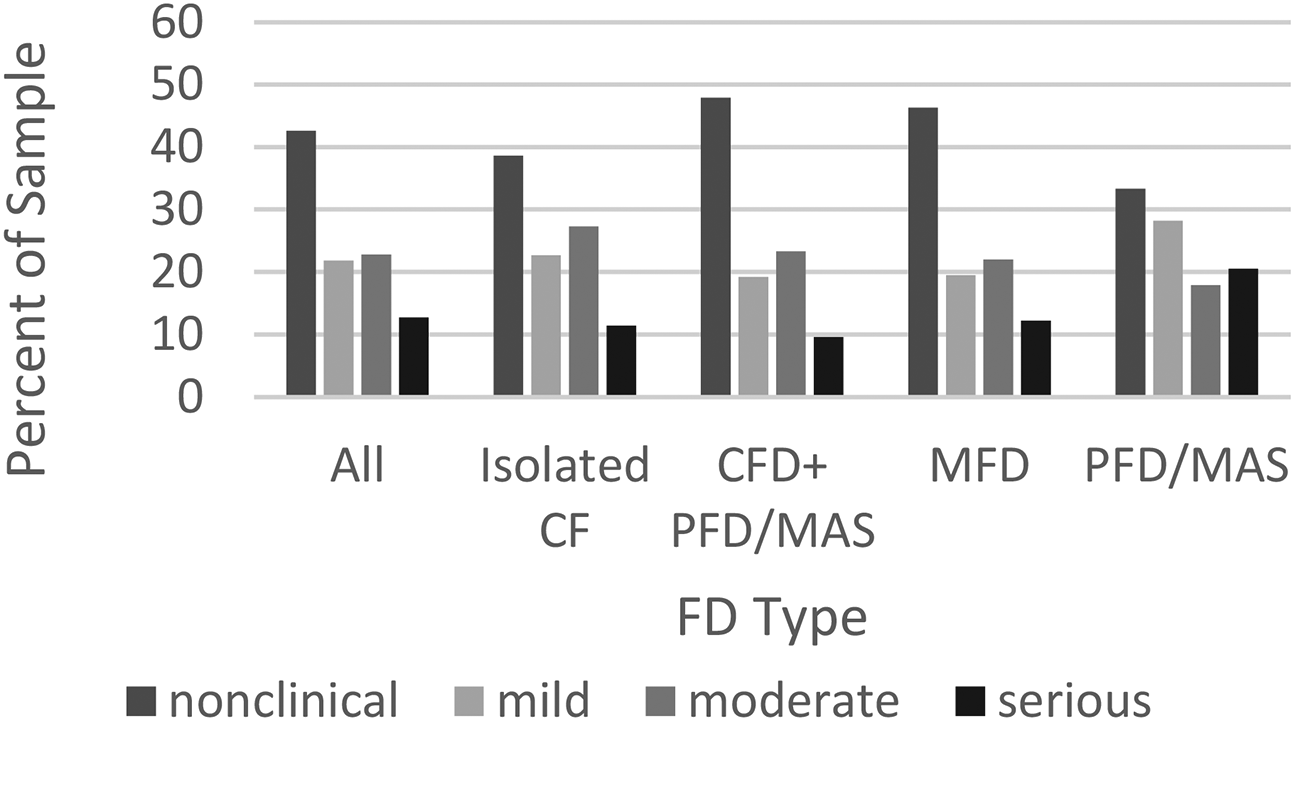
Percentage of population exhibiting clinical levels of anxiety by fibrous dysplasia (FD) types percentage.
Fewer, 44.5%, expressed clinical levels of depression, of which 15.3% were moderate or serious (Figure 2).
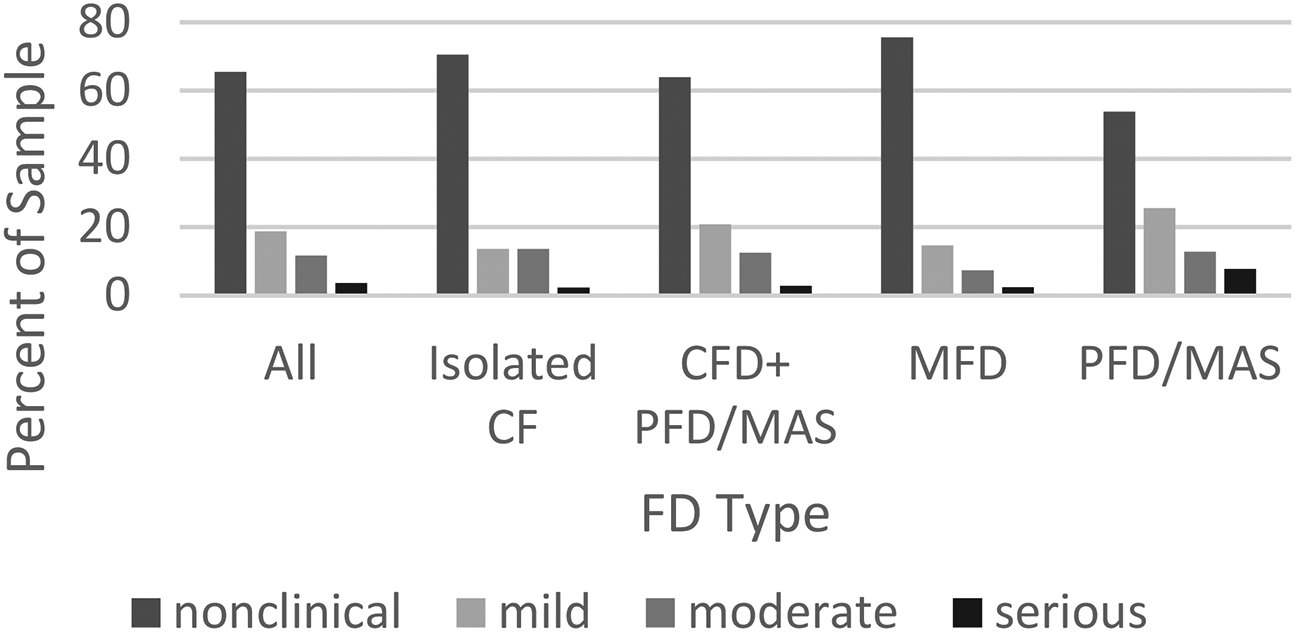
Percentage of population exhibiting clinical levels of depression by fibrous dysplasia (FD) types percentage.
Kruskal–Wallis H tests established that mean differences between the types of FD were not statistically significant for either anxiety (p = 0.489) or depression (p = 0.198).
Discussion
The first hypothesis, that the patient sample would differ significantly from the general population was supported. Scores for all SF-36 domains and stigma were significantly lower than the population benchmark. A sizable minority of the population also registered treatable levels of anxiety and depression.
The NIH study of adults and children 14–17 years of age with FD, which was normed to the same SF-36 values as this study, did not find significant differences with the general population for mental health measures. 7 Three alternative explanations address this difference. First, compared to the NIH sample, FDFPR respondents are more likely to have received care from physicians unattached to comprehensive teams of specialists, and to have received a wider range in quality of care. Lower FDFPR scores may accurately reflect the mental health burden associated with the uneven access to and quality of care. Second, participation in the NIH protocol, which involves multiple interactions with clinicians and opportunities to be considered for experimental treatments, may elevate hopefulness and feelings of support. Third, including patients 14 to 17 in the NIH study may shift means for SF-36 domains upward in comparison to this study of patients 18 and above.
The finding of significantly greater stigma in the FD patient population than a population of individuals with a variety of common neurological conditions population is important. The finding that FD patients with and without CFD experience high levels of stigma points to the need to incorporate screening into the structure of early care 18 and to consistently refer patients and families to support groups and patient organizations.19,20 Such communities can help normalize the patient identity, offer coping strategies, and provide a disability rights orientation to discourage stigma internalization through online and face-to-face interaction. Studies have established that a combination of psycho-social education and cognitive behavior therapy can reduce the self-stigmatization among the chronically ill 18 and narrative practices can help reduce self-stigma. 21
This study did not support the second hypothesis. We cannot conclude from these results that isolated CFD is unique. Scores for isolated CFD were significantly less than PFD/MAS for the physical function domain; however, this may be a result of the SF-36 lacking functional items that are relevant to craniofacial problems. CFD + PFD/MAS had greater stigma than MFD, but not isolated CFD or PFD/MAS. Lesions in isolated regions outside the skull may not be noticed by others because they impede normal movement to a lesser extent and any disfigurement is covered by clothing. In comparison, individuals with visibly distorted bodies and skulls are more likely to both move differently and appear different and attract more attention and negative reactions. The CFD group had a higher percentage of cases that involved the skull base, an area that is not visible to others, which may account for its lower mean for experienced stigma in comparison to CFD + PFD/MAS.
Feelings of deviance and devaluation are not tied to objective features of bodies. Rather, they stem from how individuals have learned to give meaning to their bodies and reflect their varied histories of interaction with family members, experiences in institutional settings, and consumption of media. The consistent levels of clinically moderate to severe anxiety and depression found in this sample across the types, may reflect the chronic nature of FD/MAS, lack of access to effective treatments, especially for pain, and the general isolation of being an FD/MAS patient, as well as stigma. 20
From the standpoint of understanding QOL of those with FD/MAS, the widely deployed SF-36 has limitations, lacking items addressing craniofacial issues such as sight, hearing, chewing, and speaking and the impact of the quality of social interactions affected individuals have. It is critical to develop QOL measures for FD/MAS that capture the full spectrum of its symptoms and the ways in which they affect daily life. 22
Limitations
To compensate for lack of clinical data in the FDFPR and the self-registration of participants, reported bone lesion data was cross-referenced to establish support for reported diagnostic categories. However, a small chance remains that an individual reporting monostotic CFD might have some other bone disorder. The sample, which is predominately white, educated, and female is not representative of a disease that is not sex related or limited to an ethnic group. The greater participation of women may reflect greater concerns about illness and might elevate scores. Alternatively, gender norms may lead men to be less comfortable reaching out to an advocacy organization and/or reporting on their emotional state. The history of coercive research involving racial minorities may also contribute to the low rate of participation by nonwhites. Additionally, internet access needed to complete the multiple surveys in the FDFPR is possibly a barrier to the participation of those of limited income.
Conclusion
Understanding the illness experience of FD/MAS in the United States requires acknowledging that its rarity has shaped and continues to shape access to medical care and the social lives of patients. Prior to the late 1990s, when Dr Michael T. Collins began to supervise the natural history study of FD/MAS at NIH, there was little attention to the disease outside of case studies. Accurate diagnosis was often delayed in many cases and ongoing care was provided by clinicians who had not seen prior cases. Although off label clinical trials conducted at NIH and elsewhere found some drugs to be therapeutic, lack of clear clinical recommendations and FDA approval limited health insurance coverage for desired medical treatments and surgical procedures well into the 21st century. The first comprehensive set of clinical recommendations for the treatment of FD/MAS was published in the Orphanet Journal of Rare Diseases in 2012. 23
Prior to the 2000's, few FD/MAS patients met others with a similar diagnosis. In 2004, FD/MAS patients who participated in a disease focused listserv and met each other through the NIH study created the FDF. The FDF developed written resources about FD/MAS diagnosis and effective treatments for patients to share with their primary medical providers and identified physicians experienced in treating various aspects of the disease. The FDF also developed a website and held conferences to bring clinicians, patients, and caretakers together in person. Two Facebook groups now enable thousands of affected individuals and their supporters to communicate about living with the disease despite distance. It is important to keep in mind when studying long-term QOL that FD/MAS patients living far from teaching hospitals still find it difficult to locate experienced medical providers, and those age 40 or older experienced the growth stage of their disease when well-informed physicians were least accessible, and patients were most isolated.
Results of this study demonstrate that the QOL impacts of FD are significant, when compared to the general population, and extend to the experience and internalization of stigma, depression, and anxiety. They are not limited to individuals with craniofacial lesions or to polyostotic/MAS disease. Addressing these psychological and social issues should be a focus of care and research.
Footnotes
Acknowledgments
Tovah Burstein assisted in piloting the Fibrous Dysplasia Foundation patient registry data. Dr Andrea Burke collaborated in acquiring and cleaning the craniofacial data and developing the craniofacial typing and burden score. Lydia Capicotto assisted in cleaning the noncraniofacial data. Lisa Heral and Catherine Fairchild provided commentary on the manuscript.
Contributorship
All authors contributed equally to the data analysis and development of the manuscript.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data acquisition and initial analysis of the craniofacial data was supported by the Oral Maxillofacial Surgery Foundation.
Ethical approval
Data collection protocols for the Fibrous Dysplasia Foundation Patient Registry (FDFPR) were reviewed by New England IRB (Needham, MA) and are in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Deidentified data provided for this study by the Fibrous Dysplasia Foundation was deemed exempt from further review by the author's institutional IRB.
Guarantor
AK.
Informed consent
Informed consent/assent was obtained from all individual participants included in the study by the Fibrous Dysplasia Foundation, from which the data was obtained.