
Abstract
Objective
Behçet’s disease is a rare and incurable condition where the body’s immune system attacks healthy tissue. Behçet’s can cause blood clots and ulcerations to form in every organ and system in the body, including deep and painful genital ulceration. The psychological impact of the disease on intimacy and relationships is unexplored. This study aimed to explore how the disease impacts on female patients’ intimate partner relationships.
Methods
Participants were seven female, UK patients with Behçet’s disease who were in committed relationships. In depth, semi-structured interviews lasting approximately 80 minutes were conducted via video conferencing about participants’ sexual functioning and intimate relationships. Data was analysed using Interpretative Phenomenological Analysis.
Results
Patients’ sexual relationships and intimacy were impacted by issues due to lack of knowledge of symptoms (misdiagnosis of herpes), issues due to symptoms (genital manifestations, painful sex, exhaustion), difficulties communicating with medical professionals, medication, partner support, and support from fellow Behçet’s patients.
Discussion
Female Behçet’s patients are at risk of developing psychological problems with intimacy due to symptoms, lack of knowledge of symptoms, and negative impacts of medication. Intimacy needs to be discussed in medical consultations so these issues can be addressed before a lack of intimacy negatively impacts relationships.
Introduction
Behçet’s disease is a rare, complex and incurable condition that affects approximately 1000 people in the United Kingdom and 200,000 people in the United States. 1 The disease causes the body’s immune system to produce inflammation, which is manifested in the form of mouth ulcers, joint pain, headaches, gastrointestinal ulceration, vision threatening eye inflammation, cognitive impairment and painful genital ulcers which heal with scarring. 2 Approximately 70% of patients with Behçet’s will experience genital ulceration. 3
The pain caused by Behçet’s can be severe and has a negative impact on patients’ quality of life.4,5 Treatment often includes steroids, immune suppressants and anti TNF inhibitors, which may cause unpleasant side effects such as nausea, weight gain and increased risk of serious infections.6,7 Primary treatment consists of oral immune suppressants, often administered alongside prednisolone. If this fails or the disease is aggressive, biologics such as infliximab or Humira are recommended. 8 Behçet’s may be fatal if not identified quickly and it is often undiagnosed for many years, leading to increasingly severe symptoms. 9
For women with Behçet’s disease, ulceration can develop on both the external genital region and where it cannot be seen, such as on the cervix. 10 Ulceration may create a barrier to successful sexual relations due to pain. Even when there are no external ulcers, patients may be unaware of hidden internal ulcers until after penetration has commenced. This may lead to anxiety, avoidance of penetrative sex and potentially to vaginismus: a condition where the vaginal muscles involuntarily tighten in response to the anticipation of pain. 11
Previous research into the effects of sexual issues in female Behçet’s patients utilized a generic female sexual dysfunction scale and self-reported depression testing. This found female patients with Behçet’s are more likely to experience sexual dysfunction and depression relative to healthy controls.12,13 The link between Behçet’s and depression is also well established.14,15
Although sexual dysfunction is reported in many chronic diseases, research has ignored the impact of sexual dysfunction until recently. 16 Related to this, research suggests that the medical profession may not recognise that chronically ill patients are struggling with intimacy and often do not initiate discussions. 17 Society may view disabled and chronically ill women as asexual beings who are not desirable. 18 In a conceptual model of the relationship between chronic disease and sexuality based on a range of research, the interdependence between physical condition and psychological wellbeing is described as the ‘cornerstone’ of sexuality. 16 Behçet’s disease patients, in common with individuals with other chronic diseases, face many challenges which may undermine this cornerstone. 19
There is a lack of research into the ways in which patients with Behçet’s disease experience sexual function problems and intimacy issues, and how these impact on their intimate partner relationships. Since patients in the UK are seen at 3–6 monthly intervals, early identification and prompt treatment of these issues is important.
This research will explore how female patients of Behçet’s disease experience sexual relationships by considering both the physical symptoms of the disease and the resulting psychological effects.
Methodology
Design
This research used an interpretative phenomenological approach (IPA). IPA was selected as the most suitable method as it is concerned with participants interpreting their own lived experiences with intimacy and Behçet’s disease. 20 The researcher in turn – herself a Behçet’s patient – will seek to explore and understand the participant’s perceptions, thus fulling the double hermeneutic interpretation process of IPA. As there has been little previous research into the psychological impact of Behçet’s disease, an IPA approach is additionally suited as this is a novel, highly sensitive and complex topic. This study is presented in accordance with the COREQ criteria.
Recruitment
Following obtaining ethical clearance from the ethics committee (ref 22329), participants were recruited through a Facebook page run by Behçet’s patients for confirmed patients based in the UK. The first author, a woman living with Behçet’s obtained permission from the page Administrator to ask female members if they would be willing to participate in an interview regarding the effects of Behçet’s on intimate partner relationships. The research declared in this first post that she was a Behçet’s patient. Interested page members were asked to contact the first author directly via Messenger and not to comment under the original post to ensure anonymity. Using purposive sampling, the first ten respondents who confirmed that they were Behçet’s patients, female and in an intimate relationship were provided with an information sheet and consent form. On return of the signed consent form, the first author contacted the participants to arrange an interview. The first author had no previous knowledge of the participants and had not engaged with them on social media or met them at the Centre of Excellence.
Interviews
The questions were developed following consultation with the two of the specialist psychologists at the Behçet’s Centres of Excellence and by referring to previous research into intimacy issues caused by other auto-immune and inflammatory conditions. As a Behçet’s patient, the first author had experienced intimacy issues caused by the disease and therefore the question design was guided by this but was kept open and flexible to encompass all experiences.
Five of the participants were interviewed using video calls, one by telephone, and one face-to-face at her home by the first author. A discussion to establish rapport took place prior to the interview to establish a comfortable relationship between the first author and the participant. Only the first author and participant were present during the interview. Semi-structured interviews were conducted to maintain the flow of participant narrative but at the same time ensure the following topics were covered: a brief history of their journey to diagnosis, overall symptoms they experience, the genital manifestations of the disease, how the disease effects their intimate partner relationships and the effect of their medications on intimacy. The interviews were conducted between October and December 2018 and were recorded onto the Sonocent audio note taker program. All interviews were transcribed verbatim by the first author, then anonymised and the recordings deleted after transcription.
Reflexivity
The first author is a female Behçet’s patient who has lived with this disease for most of her adult life. Her diagnosis is fairly recent (December 2016), and she receives treatment at the Centre of Excellence in London. This was advantageous as the first author had experienced many of the same symptoms as the participants and was therefore able to identify with them. The researcher made every effort to minimize the effects of bias by consulting Behçet’s psychologists and the second author before commencing the research. However, as a female Behçet’s patient, she acknowledges that her own lived experiences of intimacy in the context of this disease may have led to her interpreting patient experiences in accordance with her own experiences.
Data analysis
Each interview was transcribed verbatim by the first author. References to personal details such as names of partners or consultants were redacted. To gain familiarity with the transcripts the first author read each of them 3 times and annotated the text with her interpretations. The first author then used NVivo software to continue the analysis. Selecting a transcript at random, the first author used initial interpretations as themes; comments and experiences relating to these were coded into parent nodes. The transcript was then examined to establish how the participant understood or perceived these experiences – these were coded into related child nodes. Each remaining transcript was coded in the same way and the themes selected for inclusion reflected those which the majority of participants had experienced. The second author checked and validated the coding.
Results
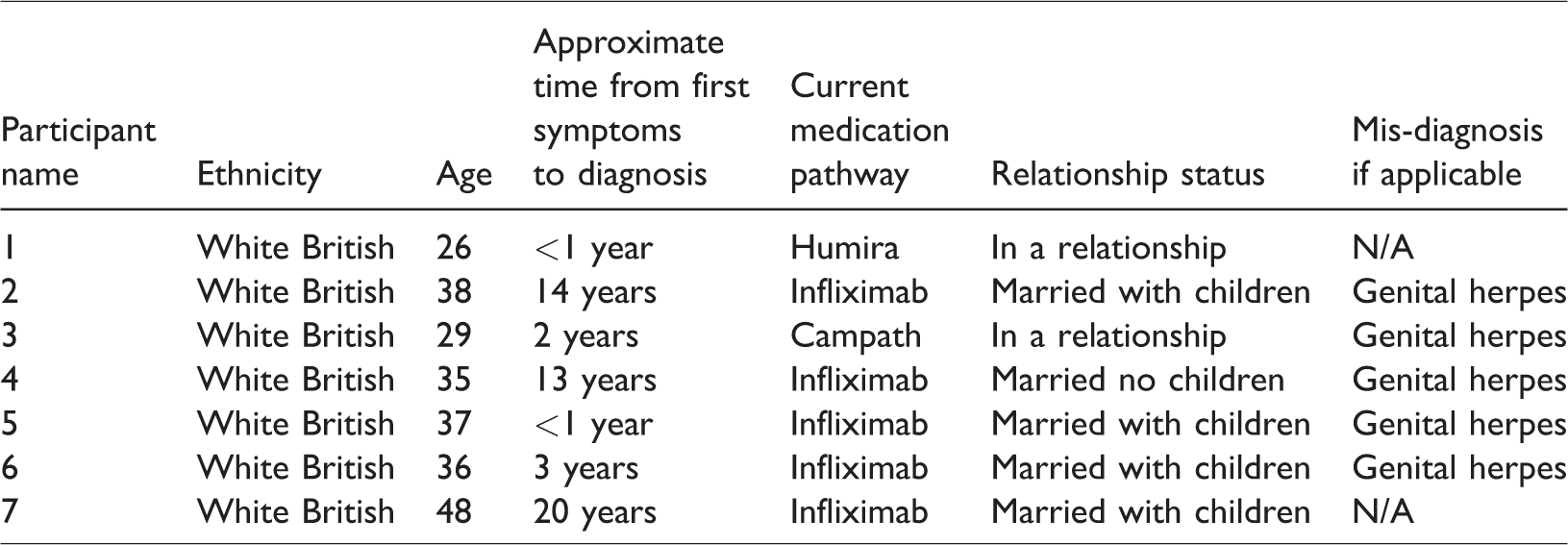
Participants were seven white, CIS gendered British female patients who had been diagnosed with Behçet’s and experienced genital manifestations of the disease. Table 1 presents the participant’s ages, relationship status, medication pathway and time to diagnosis – the mean diagnosis time was 7.7 years. The interviews were completed within 44 minutes to 1 hour and 31 minutes (mean 58.7 minutes, SD =15.43 minutes).
Relationship status, age, medication pathway and diagnosis time of participants.
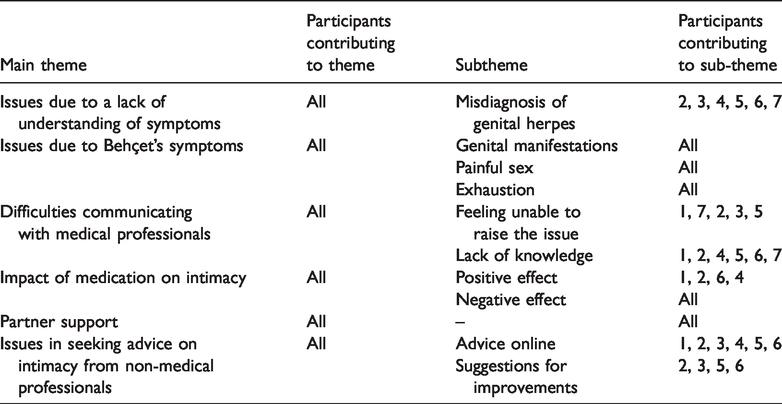
The six main themes and corresponding subthemes are presented in Table 2.
Themes and subthemes.
Issues due to lack of understanding of symptoms
Misdiagnosis of herpes
Five out of seven participants were mis-diagnosed with genital herpes during the early stages of their illness. One diagnosed herself with genital herpes in the absence of an alternative diagnosis. Three were referred to Sexual Health Units where despite their insistence that they had not contracted herpes and/or all tests were negative, were disbelieved. In three cases, where participants were in relationships, misdiagnoses led to accusations of infidelity. ‘I was constantly going to doctors and asking, ‘are you sure this is herpes?’ as it’s not going away, and nothing is happening to them.’ Participant 3 ‘But the doctor accuses one of us of cheating on the other! … I was furious because if I hadn’t been in that secure relationship, what could that have done to our relationship?’ Participant 4 ‘Sometimes I think about how I was treated in hospital when I was misdiagnosed with herpes. When it was really bad, they had me on an examination chair, legs in stirrups, naked from the waist down. I felt totally exposed and vulnerable. Then they bring in a load of students and they are all just looking at my vagina and commenting on it and I just sobbed and sobbed in this chair. They just ignored my distress and I just felt completely debased, like I was not important or even worth asking if I was ok. I clearly was not ok. Every time I have to have a vaginal examination, I freak out about it. They look at me like I’m crazy, but I can’t bear that feeling of exposure and think of how traumatic it was being in that bloody chair being looked at and crying and crying.’ Participant 2 The ulcers would be the first thing I thought about when I woke up in the morning and the last thing I think about before I went to bed at night. Seriously, it is not an exaggeration, it completely took over to my life. The first eight years, I thought I had herpes. It consumed nearly my every waking thought.’ Participant 7 ‘With the herpes diagnosis, it made me feel dirty. It makes you feel dirty and that you are a liar. You’re not made to feel that with Behçet’s. You’re not made to feel dirty as it’s a medical condition.’ Participant 4
Issues due to symptoms
Genital manifestations
In addition to the typical ulcers associated with Behçet’s, all participants also described swelling, internal ulcers, tissue tears, post coital bleeding and fluid filled blisters. The pain impact of these manifestations on everyday functions such as urination was described by six participants. One participant reported having to take saltwater with her to work to keep her ulcers clean. Five participants were left with scarring from their genital ulcerations, but this did not appear to cause distress or embarrassment. ‘I was in absolute agony! I couldn’t even go to the toilet; it was that bad. I had to wee in a bath. It was so kind of extreme: they just didn’t heal up.’ Participant 3
Painful sex
All participants reported vaginal pain during intercourse. This was either due to genital ulceration, either internal or external, or less commonly reported features of Behçet’s such as tissue tearing. For six participants, the levels of pain either prevented them from having sex or meant they would have to stop once they had started. This led to them being anxious about pain before intercourse and concerned over aftereffects such as swelling, and bleeding. Five participants reported feelings of frustration and guilt when they were unable to complete intercourse with their partner. ‘I just physically couldn’t, I just physically couldn’t hide the pain….it’s as though someone is tearing your vagina with razor blades.’ Participant 4 ‘I’d like the idea (of sex), but I would find it painful and I’d be worried. I was just worried that I’d find it painful, so I’d try and make sex really quick’. Participant 6
Exhaustion
In addition to vaginal pain, other symptoms of Behçet’s such as fatigue and joint pain created issues with intimacy. Six participants worked and/or had caring responsibilities; finding the energy to have sex at the end of the day was impossible. For one participant, the ulcers had eroded her nerve endings and as a result, did not experience the same levels of arousal she once had. ‘It’s like someone has sucked all the energy out of your body and you can barely walk, you can barely move, you certainly don’t feel ready for the physical pressures of having sex……I just cannot dredge the energy out to have sex with him.’ Participant 2
Difficulties communicating with medical professionals
Feeling unable to raise the issue
Five participants had not discussed their intimacy issues with health care professionals. This appeared to be in part due to never being asked and their reluctance to raise the issue. At the same time, these participants felt they needed help and support and would have spoken if a medical professional had asked. In one case, the husband of a participant raised intimacy issues with many of his wife’s doctors, yet the problem was not explored further. ‘It’s very much symptom-based or medication based. If it had been broached and I’d been given the opportunity to say, ‘we haven’t had sex for 18 months.’ I think in my mind I just assumed that because I was so unwell, we wouldn’t be having sex. Intimacy was never discussed. If it had been discussed, I could have said what the problems were, and I could have said, ‘it’s just not a physical thing, it’s becoming a psychological barrier now.’ Participant 5 ‘I find that if it’s a male versus female doctor: I think that a male doctor just isn’t good at understanding in the same way just because of their anatomy. It’s nothing personal but I don’t think it’s something I’d ever feel comfortable asking a male doctor because I just don’t think that they would be able to give me advice in the same way as a female.’ Participant 1
Lack of knowledge
Six participants reported lack of knowledge of Behçet’s disease amongst non-specialist doctors. In many cases, participants were sympathetic to this given the rarity of Behçet’s, as they did not expect to see expert knowledge outside of the Centres of Excellence. However, this did cause issues with obtaining appropriate treatment when participants were in-between specialist appointments and was a cause of frustration. ‘It’s kind of difficult because even though I like most of the GPs at my surgery and they can be quite sympathetic. Every time I do have a problem, they just say ‘go to the centre of excellence’. Well, yeah, I can’t just make an appointment and go next week. I have to wait six months before I go again!’ Participant 2 ‘This disease is a dangerous game and unfortunately some doctors just don’t know about it.’ Participant 4
Impact of medication on intimacy
Positive effect
Three participants reported that their Behçet’s medication was positively impacting their intimate relationships. Where the medication promoted faster healing of ulcers or alleviation of pain, the participants felt able to have sex with less anxiety. Topical creams such as Vagisil and Lidocaine had been prescribed to two participants, both of whom found this helpful during sex. However, the unpleasant smell of lidocaine was a negative point as well as waiting for it to take effect. One participant commented that although her medication had improved her symptoms, it had no effect on her sex life. ‘In general, the immunosuppressants that I’ve been taking have been helpful in managing my symptoms, so I have less ulcers on the drugs that I take. This is good, but I can’t see that its actually improved my sexual relationship with my husband.’ Participant 2 ‘They make me more able to have sex, put me in less pain so medication if anything, is made better for me rather than worse. I get prescribed numbing cream which I put in the fridge so it’s cold and that I found really helps.’ Participant 1
Negative effect
Unfortunately, all participants reported that their medication was having a negative effect on their intimate relationships both through changing physical appearance and side effects such as nausea, fatigue and loss of sensation. In terms of changing physical appearance, steroids appeared to be causing the biggest issue. Four participants reported putting on weight and becoming irritable, which in turn affected their self-esteem and promoted anxiety about their bodies and concerns that their partners would no longer find them desirable. Three participants noticed an increase in body hair when on steroids which impacted their self-esteem and prompted concern that others would not find them attractive. ‘… I was on a lot of medications and some of the side-effects of those meant I was gaining weight. I felt unattractive and the more he didn’t touch me the more I thought that he didn’t fancy me.’ Participant 6 ‘I can’t even bear to look at myself in the mirror and I’m so worried my husband won’t want to look at me. I remember saying to the doctor actually, that I don’t even look like myself anymore’ Participant 7
Partner support
Six participants described their current relationships as being loving and supportive. For five of them, their current partner or husband had watched them become unwell and in effect, had taken the journey to a Behçet’s diagnosis with them. Two had to explain what Behçet’s was and how it affects them to their current partner. Feeling that their partner took the time to understand the disease was important, as well knowing that their partner was willing to look after them. ‘He’s a really nice patient person. He understands what the symptoms are, I know that he understands. He sees me when I’m at my worst and he takes care of me and he looks after me.’ Participant 2 ‘I know that I’m very lucky to have her and that she accepts me overall especially as she didn’t have to be with me’ Participant 1
Despite this, four participants reported that intimacy issues caused by Behçet’s disease had a negative impact on their partner. One participant reported a suspicion that her husband was using pornography and might have had an affair due to her inability to have sex. In one case, the husband of a participant was so profoundly affected by his wife’s severe pain on intercourse that he now needs Viagra to have sex. The five married participants felt an emotional distance and detachment from their partners caused by the lack of intimacy. These participants were anxious about being physically affectionate with their partners in case it led to sex and their partners were anxious about initiating sex in case they caused pain or were rejected. ‘He lost confidence in the bedroom completely. I think my hysterectomy kind of gave him reassurance because I wasn’t bleeding all the time. We tried for a long time, but he now has to take Viagra. That had a profound effect on him, more than I realised at the time’ Participant 4 ‘You don’t want them to come near; you don’t want to initiate any kind of sexual contact because you just can’t deal with it. You can’t have sex for a start, I think I struggled to reassert that kind of spontaneity and intimacy and affection towards him. It does impact on him for sure and I think now he doesn’t know whether to instigate it in case he is rejected.’ Participant 5
Issues in seeking advice on intimacy from non-medical professionals
Advice online
A commonly cited source for external support (six participants) were the various Behçet’s Facebook support pages. There are several UK based pages, the most popular of which is managed by a small number of Behçet’s patients. As there are so few Behçet’s patients in the UK, many use a popular US run page which has nearly 1500 members. Being able to discuss intimacy with fellow Behçet’s patients and to know that others shared their experiences was comforting. In three cases patients were given advice on lubricants to use for sex without seeking medical advice. A negative impact of this was that the advice given not only made the issue worse but more often proved ineffective. ‘I think someone once recommended that I tried coconut oil to help in terms of lubrication I guess in that it was soothing. So, I bought some and when we tried it, I can’t say it made a massive difference.’ Participant 1 ‘I have always used spit as a lube and lots of people do apparently. It is designed to begin to break down your food before it goes into your gullet. The spit I was using was helping break me down and made the problem worse. ‘Participant 4
Clinical improvement suggestions
Participants also made suggestions regarding how the medical profession could improve when delivering their care. These included having a proper box or shelf for clothing storage during internal examinations at the Centre of Excellence– currently; it must be left on the floor or a chair. Others suggested doctors might be able to offer topical creams to either assist with lubrication or to increase desire to have sex. It was also raised that the online information about the genital manifestations of Behçet’s disease could be improved to include a wider range of symptoms.
Discussion
Misdiagnosis of genital herpes
A misdiagnosis of genital herpes was of particular significance during this research. For those who experienced genital ulceration as a first symptom, treatment at a Sexually Transmitted Infection clinic was the usual pathway to treatment. The disbelief and treatment with anti-viral medication when tests were negative and no history of unprotected sex with a herpes sufferer are concerning. It may be that denials of this nature are commonly seen in STI clinics due to the stigma of sexually transmitted diseases however, it did not appear that an alternative diagnosis was considered even when participants developed other symptoms such as erythema nodosum and mouth ulcers.
It is possible that the experience of a herpes misdiagnosis has had a negative effect on the participant’s future intimate relationships, as anxieties over infecting partners and accusations of infidelity were reported. In support of this idea, Foster & Byers 21 found severe manifestations of genital herpes and the Human Papilloma Virus predicted higher levels of sexual anxiety, lower self-esteem and sexual satisfaction.
Genital herpes is rarely misdiagnosed but there are some conditions which can cause similar ulceration such as Varicella Zoster and aphthous genital ulcers; both conditions being linked to viral activity.22,23 Maia et al. 10 advise that practitioners should consider Behçet’s when a patient presents with genital ulcers and other symptoms such as oral ulcers and uveitis.
This finding may provide opportunities for change. The mis-diagnosed patients were all told they had herpes in the early stages of their disease; effectively delaying a correct diagnosis of Behçet’s. There is potential for greater awareness of Behçet’s within practitioners who work in STI clinics, particularly when a patient repeatedly tests negative for herpes. A debrief process could also be considered for individuals who have been mis-diagnosed to provide reassurance that they do not have genital herpes and to establish at an early point if this misdiagnosis has or is causing psychological issues.
Difficulties with maintaining intimacy due to both the disease and medication
Participants were found to be experiencing difficulties in maintaining a satisfactory intimate relationship with their partner due to a combination of physical and emotional factors. Common symptoms of Behçet’s such as fatigue and joint pain reduced the ability to engage in regular sexual intercourse. Every participant had experienced vaginal pain when having intercourse and many reported feelings of trepidation, fear that intercourse would hurt and anxiety about partner expectations to have sex. This may suggest that Behçet’s patients are at risk of developing vaginismus, however further research would be needed to confirm this. Binik’s 11 proposed diagnostic criteria for vaginismus may provide a potential basis for this as it includes both experienced pain and fear of pain with an underlying medical condition.
Unfortunately, for most participants, the medication negatively impacted their intimate relationships through both changing physical appearance and side effects such as nausea, fatigue and loss of sensation. In terms of changing physical appearance, steroids caused the biggest issue. Participants reported an increase in weight, body hair and becoming irritable, which in turn affected their self-esteem and promoted anxiety about their bodies and concerns that their partners would no longer find them attractive. Similar negative physical changes and resulting reductions in self-esteem have also been reported by patients with Rheumatoid arthritis and Inflammatory Bowel Disease who are treated with steroids.24,25 Patients need to be fully informed about the risks of their medication and how medications such as steroids may alter their appearance.
Difficulties communicating with medical professionals
Patients mentioned reluctance raising intimacy issues in clinic appointments but said they would discuss such issues if they were raised by healthcare professionals. However, this is not always the case. Similar findings have been reported in relation to older adults living with chronic illness, fibromyalgia and multiple sclerosis patients.26–28 To overcome this barrier consultants may consider inquiring about sex and relationships with their patients. If there are topical medications which might assist with the numbing the pain of intercourse or providing additional lubrication, these could be prescribed early on; before the issue becomes psychological.
The fact that some patients were seeking advice on lubrication to use for sex via Facebook and other non-medical sources is a source of concern. The advice given to patients in this matter does not consider the severity of their disease or interactions with other medications. Similar issues around seeking medical advice from non-medical sources have been reported by patients with other chronic illnesses such as asthma. 29 Further research is required to determine the best way to inform patients about the risks of using non-prescribed medication.
Given the range of symptoms reported by participants in this study, future considerations may include updating the information available to patients and their families on the wider range of genital manifestations. This may provide reassurance to those who are experiencing symptoms other than genital ulcers. In addition to this, an information sheet on how Behçet’s may affect intimacy might benefit patients.
Limitations and implications for further research
The primary limitation of this research is the small sample size and lack of diversity of participants. Every participant was on a biologic medication; meaning that they were suffering from a more severe form of Behçets. Therefore, women with less severe symptoms were not represented in this research. During the recruitment phase, those with more severe symptoms might have been more likely to want to take part as their condition was impacting more on their lives than those whose disease was well controlled or less severe. Participants were recruited from a Facebook group, which meant it was not possible to reach those who don’t use Facebook or may also be less aware of technology. The sample included only women participants, meaning the results cannot be applied to male patients. Although many commonalities were found between participants, there was also a vast amount of experiences unique to each individual’s disease, relationships and diagnostic path which would be impossible to explore fully.
Further studies on groups of participants with less severe disease should be considered to expand on these findings. A similar study on male patients with Behçet’s disease is also recommended as well as inclusion of the partners of Behçet’s patients, to determine the impact of the illness on them. Research with consultants would also be helpful in order to identify barriers to discussing sex and relationships in appointments.
Conclusion
The intimate partner relationships of the Behçet’s patients in this study were all affected by both the symptoms of the disease and the effects of medication. Painful sex caused by the genital manifestations of the disease was compounded by fatigue and joint pain. Where medication was controlling patient’s symptoms, side effects and changes in weight and appearance decreased desire and ability to have sex. Patients are often unable to communicate these issues to doctors and sometimes seek advice from non-medical sources. Most patients had experienced an incorrect diagnosis of genital herpes which caused them emotional distress and led them to question the loyalty of their partners. It is recommended that intimacy is discussed in medical consultations so these issues can be addressed before a lack of intimacy negatively impacted relationships. The introduction of a debrief process to allow patients to discuss the impact of previous misdiagnosis is also recommended.
Footnotes
Acknowledgements
I would like to thank the doctors of the Behçet’s Centre of Excellence for their support. To the participants: thank you from the bottom of my heart for your bravery and candour. All of you told me that your reason for taking part was to improve the lives of other patients; a testament to your strong characters and selflessness. I wish you all the best of everything.
Contributorship
FS wrote the first draft of this manuscript. EAC reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report these cases was obtained from Bournemouth University Ethics Committee under reference number 22329.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patients in the form of participant consent forms for their anonymised information to be published in this article.
Guarantor
FS.