
Abstract
Objective
We explored the underlying mechanisms by which storytelling can promote disease self-management among people with type 2 diabetes.
Methods
Two, eight-session storytelling interventions were delivered to a total of eight adults with type 2 diabetes at a community health center in Toronto, Ontario. Each week, participants shared stories about diabetes self-management topics of their choice. Using a qualitative descriptive approach, transcripts from each session and focus groups conducted during and following the intervention were coded and analyzed using NVivo software. Through content analysis, we identified categories that describe processes and benefits of the intervention that may contribute to and support diabetes self-management.
Results
Our analysis suggests that storytelling facilitates knowledge exchange, collaborative learning, reflection, and making meaning of one’s disease. These processes, in turn, could potentially build a sense of community that facilitates peer support, empowerment, and active engagement in disease self-management.
Conclusion
Venues that offer patients opportunities to speak of their illness management experiences are currently limited in our healthcare systems. In conjunction with traditional diabetes self-management education, storytelling can support several core aspects of diabetes self-management. Our findings could guide the design and/or evaluation of future story-based interventions.
Introduction
The key to preventing diabetes complications is successful disease self-management, enabled through diabetes self-management education (DSME). It aims to teach problem-solving skills to facilitate day-to-day self-care, inform decision-making, and to support active collaboration with healthcare providers to improve health. 1 There is growing evidence that the short-term benefits of DSME can be sustained with ongoing self-management supports.2,3 Self-management support services address the ongoing needs of patients by leveraging expertise community, social-support networks and more frequent visits with various health professionals. 4 Evidence suggests that combining DSME with ongoing support can improve glycemic control, self-efficacy, and self-care behaviors and reduce diabetes distress and foot complications.2,3,5
Within this approach, story-sharing among peers shows promise in enhancing disease self-management. Peer to peer interventions can improve comprehension of the disease and facilitate reflection on illness and self-management experiences. Participants often engage in group problem-solving, and by listening to the experiences of others they are able to identify new self-management strategies and/or ways to integrate management recommendations. 6 Stories provide insight into what could be, and allow teller and listeners to reflect and make meaning within their own lives. 7 Storytelling interventions have been reported to motivate better management7,8 and to foster close relationships and peer support. 9
Storytelling interventions, the activity of telling or writing stories, have been evaluated in populations affected by diabetes,7,10–14 cancer,15,16 high blood pressure, 8 psychiatric disorders, 17 and mixed chronic diseases. 18 However, the heterogeneity in the intervention design, delivery, and assessment limits researchers’ ability to meaningfully synthesize evidence about the role of storytelling interventions in improving self-management. 19 Furthermore, little is known about the mechanisms by which storytelling is purported to enhance self-management behaviors. Our study, therefore, aimed to explore and explicate the underlying mechanisms that may promote diabetes self-management behaviors in adults with diabetes during a storytelling intervention.
Methods
We used a qualitative descriptive approach to understand the underlying mechanism at play during a storytelling intervention and content analysis was used to analyze the data (i.e. intervention sessions and focus groups).
Participant selection and sample
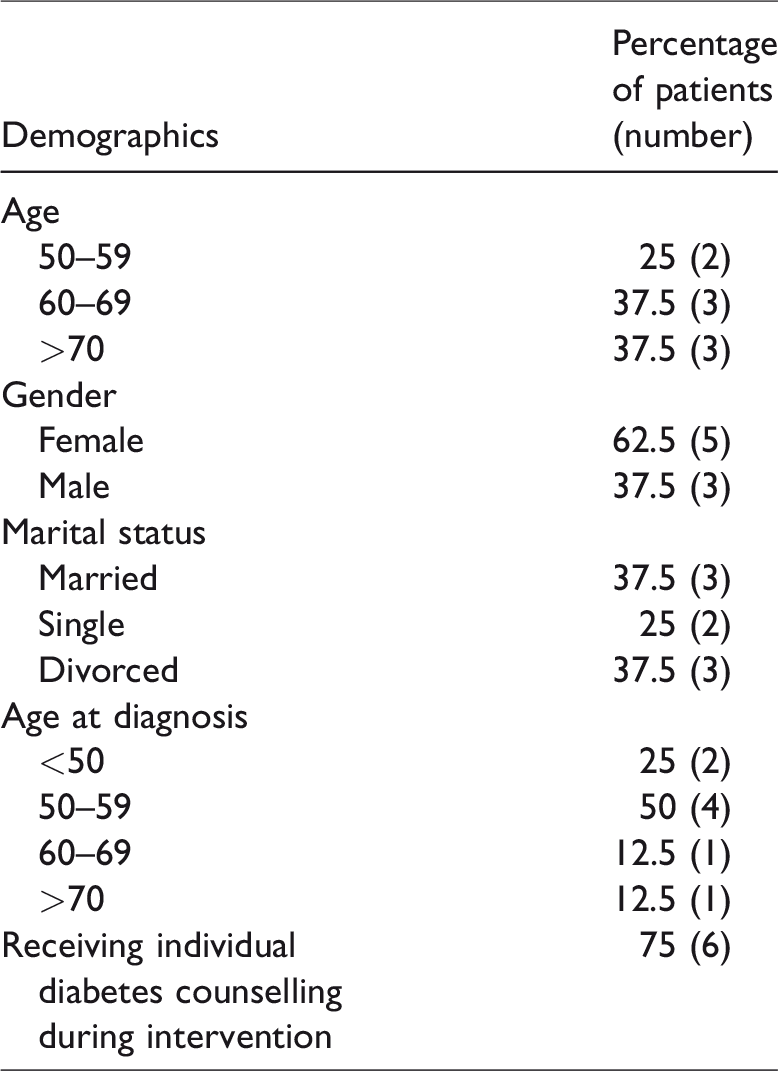
A convenience sample was used to recruit participants. Recruitment was performed by posters distributed in the community health center’s catchment area and through referral by the center’s healthcare providers. Eligible participants had to be at least 18 years of age, have type 2 diabetes, and speak English. A total of eight participants were interested in the intervention and enrolled in the storytelling intervention; three attended the first set of sessions, and five attended the second. All intervention participants were present for the focus groups. The eight participants ranged in age from 50 to 74. Most participants were females (5/8), and all were Caucasian. Equal numbers reported being married or divorced. The length of time participants had been living with diabetes before the intervention varied widely, from 1 to 24 years. During the intervention, most participants reported receiving individual diabetes counseling from a doctor, nurse, and/or dietitian (see Table 1).
Demographics of patients.
Intervention
The intervention was delivered in a community health care setting that primarily delivers a wide range of primary health care services to its catchment area. The center also hosts a diabetes education center. The participant- directed intervention involved eight sessions (two hour long) over 16 weeks. The intervention was offered twice between November 2013 and July 2014. Each session was about 1½ h to 2 h long and offered every two weeks. In the first session, participants developed group norms (e.g. respecting opinions and experiences of others without judgement, one person speaking at a time, participation from all group members) and chose the weekly discussion topics for all eight sessions. Participants also received a handout on how to prepare a story in the first session. They were also instructed that each story should have a clear purpose with a beginning, middle, and end, which all related back to the weekly topic. Participants were encouraged to describe themselves, their emotions, the situation, and/or a challenge and to break down their experience into the description, interpretation, and outcome. Participants were asked to come prepared with a story on the weekly topic for every session and received a notebook they can use to write their stories, in addition to any other personal notes.
The first two sessions began with 15 min of social time and icebreaker activities to increase patients’ comfort. Facilitators then introduced the session’s topic and asked participants to tell their stories. Participants were given an opportunity to discuss and respond to others’ stories. After they participated in activities such as ‘post-it notes’ brainstorming sessions and case scenarios to reflect upon thoughts and feelings associated with the session’s topic. Educational resources were discussed in small groups to facilitate collaborative learning.
A nurse and a dietitian facilitated the sessions. They were each trained in the storytelling process through a half-day in-person workshop and by reviewing online materials that required the completion of mandatory quizzes. This training was based on findings of a systematic review of storytelling interventions for chronic disease 19 and training manuals and information obtained from other researchers who have conducted storytelling interventions (unpublished). The facilitators’ role was to ensure that sessions progressed smoothly, validate and correct information discussed, share stories when relevant, and follow the intervention manual.
Data collection
The intervention was delivered in the community health center. After participants provided written informed consent, all intervention sessions and focus groups were audio-recorded by a research assistant and focus group facilitators, respectively. Recordings were transcribed verbatim. Focus groups were held with participants and intervention facilitators separately: midway through and on completion of the intervention by GK. The focus group facilitator (author GK) was female, had previous experience in conducting focus groups, was a Master’s student in Nutrition, and her credential at the time was Bachelor of Science. The focus group was approximately 1 h long, and questions pertained to participants’ experience and satisfaction with the intervention. The study protocol was approved by Ryerson University Research Ethics Board (REB 2013–258).
Analyses
The data collected from the intervention and the focus groups were analyzed concurrently. The intervention transcripts provided data on the processes that occurred and dynamics developed during the intervention. The focus group data highlighted participants’ experience with the intervention. Qualitative content analysis, as described by Sandelowski20,21 and Elo and Kyngäs 22 was performed on the transcripts. The process was inductive, as the two researchers independently read and re-read the data in order to create codes that organically arose from the data.22,23 Next the research team came together to discuss similar codes and were grouped together to form sub-categories. 22 From these sub-categories, the researchers engaged in abstraction, in which a coding diagram was created to collapse subcategories into generic categories, and then generic categories into main categories to develop a schema of the results including key category labels and working definitions. 22 A coding scheme was agreed upon. All transcripts were then reviewed again using the schema in NVIVO 10 by one of the researchers (ER). Examples (verbatim quotes) were identified for each sub-category. The team reviewed and finalized the categories, sub-categories and quotes. To maintain methodological rigor and trustworthiness of the data analysis, we kept detailed notes of our initial definitions of categories, sub-categories and schema, and our discussions during these meetings. Both data from intervention session and focus group were analyzed which enhanced the credibility. We obtained a high degree of congruence across both sources. Furthermore, our preliminary findings were shared with one of the intervention facilitators to ensure further credibility. Participants’ quotes are labelled by the letter P, intervention delivery (ID1 or ID2) and type of data (intervention sessions [IS] or focus group [FG]); for example, P1D2IS stands for participant one (P1), second intervention delivery (D2), intervention session (IS). Facilitators’ quotes are labelled by the letter F, intervention delivery; and type of data, FD2FG stands for facilitator (F), second delivery (D2), focus group (FG).
Data and findings
A total of eight participants were interested in the intervention and enrolled in the storytelling intervention; three attended the first set of sessions, and five attended the second. All intervention participants were present for the focus groups. The eight participants ranged in age from 50 to 74. Most participants were females (5/8), and all were Caucasian. Equal numbers reported being married or divorced. The length of time participants had been living with diabetes before the intervention varied widely, from 1 to 24 years. During the intervention, most participants reported receiving individual diabetes counseling from a doctor, nurse, and/or dietitian (see Table 1).
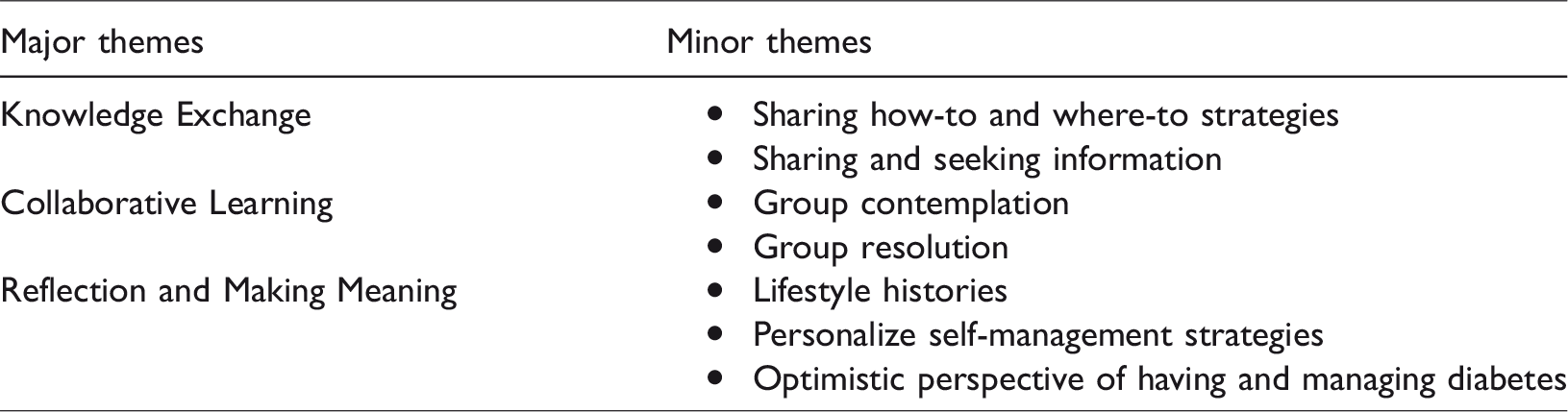
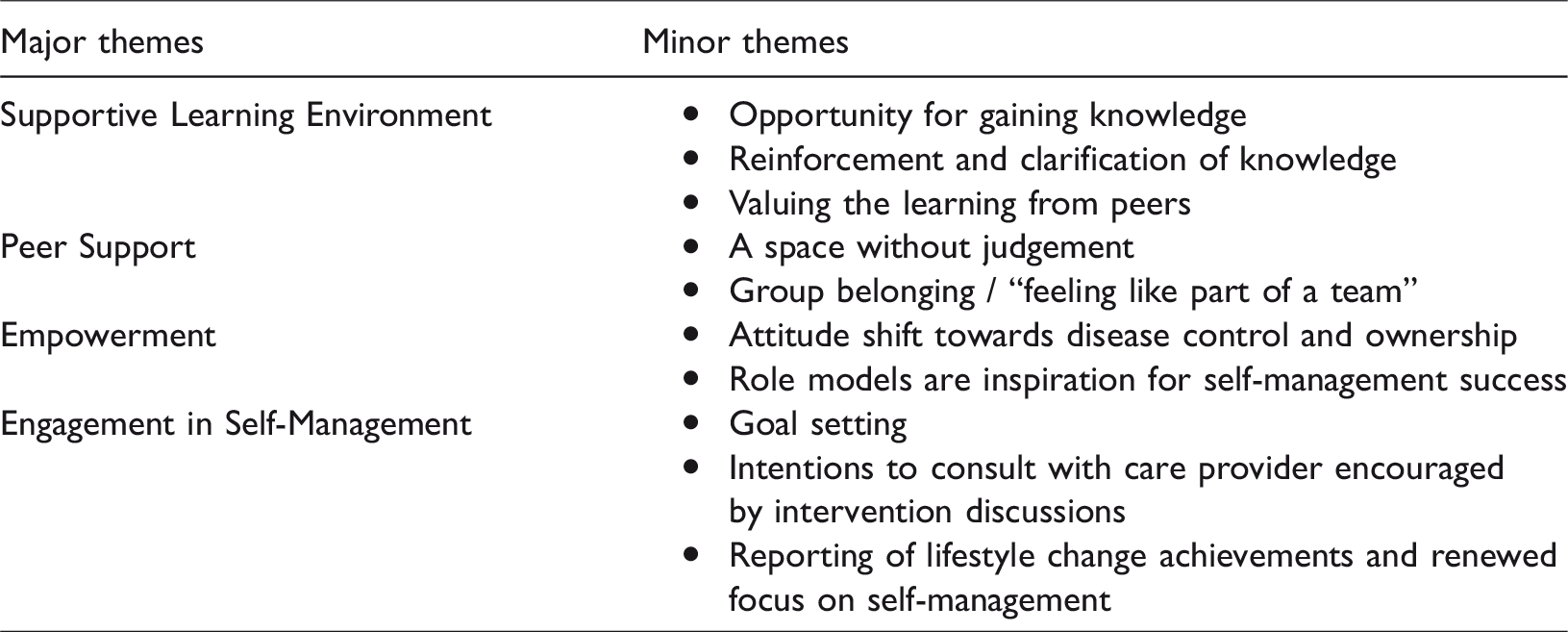
To understand how storytelling might affect diabetes self-management, we organized emergent categories by group processes reflecting happenings during the storytelling intervention, and perceived benefits addressing what participants’ felt they gained from the intervention. Group Processes included four main subthemes identified as knowledge exchange, collaborative learning, and reflection and making meaning. Perceived benefits included five main themes identified as supportive learning environment, peer support, empowerment, and engagement in self-management. Minor themes are further elaborated in Tables 2 and 3.
Processes of the storytelling intervention.
Perceived benefits of storytelling.
Processes of the storytelling intervention
Processes of storytelling describe participants’ actions, interactions and experiences observed during the intervention that may enhance diabetes self-management (see Table 2).
Knowledge exchange
Participants shared knowledge, resources, and diabetes self-management strategies with each other. Participants often shared practical how-to and where-to strategies, such as where to buy healthier food alternatives and how to cook certain foods. They also shared experiences about various health services and professionals, as well as reputable self-management resources. For example, one participant conveyed information on how much fruit to eat, provided to her by her dietitian, and further explained how to access a dietitian. The knowledge exchange among participants became a valuable and trusted source of information for participants as described by this participant, … I trust you guys. So, if you’re telling me these are good resource information, I would trust you, and go with that (P2D1IS).
Knowledge exchange often resulted from participants sharing and seeking information from the group. Some participants were considered ‘experts’ or ‘newbies,’ based on years living with diabetes. The ‘experts’ shared experiences and insights with those who had been recently diagnosed. Many looked to each other for answers and strategies, and engaged in both teaching and learning at various times throughout the intervention. When storytellers shared information, questions posed by other participants encouraged them to elaborate, which helped ensure clarity. For example, one participant questioned a participant about his experiences with low blood sugar.
P4D2IS: People do get low blood sugar?
P1D2IS: Yes, yes…and it’s very nasty, it feels awful.
P4D2IS: Do you all have that feeling? Have you all had that feeling of low blood? I don’t-don’t even know quite what it is…
P1D2IS: I can get it. If I’m not careful…and you feel faint and I actually feel nauseated, I often want to vomit. Um, and you just feel horrible, it’s just awful.
P4D2IS: And it just comes on out of the blue?
P1D2IS: No no no, it’s when you know that you haven’t eaten properly and you’ve and you’ve not given yourself enough and if my blood sugar goes below 7, I can count on it. And I hate it.
Collaborative learning
Throughout the intervention, participants tried to understand and clarify information together. For example, they were often unclear about certain topics, such as why the glycemic index for fully cooked pasta is higher than for pasta cooked al dente, or whether a quarter can of tuna provides a small or large amount of protein. They would speculate, using phrases like “maybe…” and “I think I’ve heard”. This speculation often progressed into group contemplation, with other participants adding their thoughts on the issue. In this way, participants jointly made sense of what was being discussed. During these reflections, participants also provided lay interpretations of certain concepts that helped the rest of the group. For example, one participant used the terms ‘sticky’ and ‘rough’ to describe blood and circulatory damage.
P1D2IS: Can I ask, why is it that high blood sugar leads to circulatory damage? …
P5D2IS: It gets rougher and does damage - more damage to the other cells in the walls. That’s basically it, isn’t it?
P1D2IS: It’s just thicker and it doesn’t move as fast.
P5D2IS: I think it’s more the roughness.
P1D1IS: Basically, the way I understand it is, the harder it is, the less your system [body] will take out of it.
F1D1IS: Thank you. That was actually, a really nice explanation of that.
Reflection and meaning making
Sharing stories allowed participants to reflect on their lifestyle histories and current self-management strategies. Having the opportunity to discuss the disease with others, many reflected upon the risk factors of diabetes and how their lifestyle behaviors prior to their diagnosis may have impacted their current disease state.
P2D1IS: I don’t think it’s one single thing, right? It’s uh…to me it seems like it’s a combination of a lot of things, which I just happened to do, all of them. Lifestyle was terrible, I smoked, I was overweight, still am, umm, yeah, sugar galore, I mean, I did everything. And sat on the couch and watched TV for years [murmurs of agreement throughout].
P3D1IS: I think you’ve got the average Canadian profile.
P2D1IS: I mean none of my other family, so it’s not genetic, and I look back on how I lived my life and it, it was like writing my own personal book about how to get type 2 diabetes
P1D1IS: Yeah. Yeah, me too.
P3D2IS: I’ve learned that sometimes to just cut, before I start eating, to just cut the serving in half, and then, put it out there for the rest of the people to share or something like that. Cuz, that’s my challenge. So, I have to be very careful, that there’s not too much food available to eat.
Perceived benefits of the storytelling intervention
Participants described the benefits they experienced by participating in the storytelling intervention such as: a supportive learning environment, peer support, and changes in attitude and actions that support self-management (see Table 3).
Supportive learning environment
Regardless of how long they had been living with diabetes, all participants felt the intervention was an opportunity to gain knowledge. One newly diagnosed participant said, This has been just a fantastic opportunity for information (P2D1FG). Some participants who had been living with diabetes for many years commented that the intervention reinforced self-management information and clarified information that was previously misunderstood.
P2D1FG: It helped reinforce, you know, reinforce things that I thought I had understood but kind of misunderstood and the third time it got clearer, the fourth time it’s even more clearer, and you know, um and I think this is what this group does for me.
P3D1FG. This one [intervention]……you’re going to get information that you won’t get from a doctor, or from a nurse, I mean they just can’t cover everything, and we’re all different. Everybody is different. And I learn so much from these guys. Yeah.
P2D1FG: No but I think you’re right. I think it’s a non-medical environment [agreement]. Right, and so where you talk to a doctor or a nurse, they have that professional sort of response, that’s not necessarily everything you want to hear. It’s like out in the open, we’re comfortable with each other.
P1D1FG: Unless the doctor actually has diabetes, them talking to you about diabetes is textbook. What they’ve learned, not their experience.
Peer support
Over time, participants established a sense of camaraderie amongst each other. They felt comfortable sharing their experiences and opinions without worrying of judgement from others. As mentioned by one participant, having diabetes can be an isolating experience and being able to share personal stories and recognizing themselves in other’s stories nurtures a sense of community and feeling that they are part of a team, that they are in it together on this journey of managing diabetes, which may lead to a more positive attitude toward self-management.
P3D1FG: I think what has been said there that there is a growing camaraderie, that you won’t get from the education workshops, obviously, because you’re always sitting with strangers around the table, and it’s the education workshop where you’re being instructed. But here - there’s something going on and I haven’t put my finger on…
P2D1FG: Like a bond?
P3D1FG: Like a bond forming, a feeling of, I could say a lot of things and it would be received well, that you wouldn’t be attacked.
P2D1FG: No judgment. Right, absolutely none.
P3D1FG: Right. Because I think we all recognize ourselves in what everyone else is saying.
P5D2FG: There's a certain degree of isolation, working as a diabetic. I mean, as human beings we don't, we don't like, particularly as guys we don't like portraying weaknesses, so having people to share these things is not quite like going to an AA meeting, but seriously makes you feel a little, you know, a little more positive about things
P2D1FG: This is my support group. Again being, um, newly diagnosed, I mean I got a great family support, I got a good support at work, but to [P1D1], or [P3D1]’s earlier point, they’re not diabetics, so uh yeah, it’s more sympathy than anything else. Here it’s like I’m part of the team. Right, we’re a team, and I’ve learned so much off these two guys, it’s been phenomenal. So, do I feel better? Yeah, absolutely.
Empowerment
Participants referred to an attitude shift about what it means to live with diabetes and described being more in control of their diabetes. They spoke positively about a future where they would not be defined by diabetes or be passive observers. They primarily identified the intervention and its participants in fostering this feeling of empowerment over their management.
P3D1FG: So – it’s so important, I mean I think this is about empowerment, we’re not just the victims of circumstances or of our lifestyle, this [intervention] gives us a chance to empower yourself and take back control.
P2D1FG: Without this workshop I would have found it hard to find ownership on the control of my diabetes. And it’s a key component and it’s a key word, ownership, um. Without this team ethic and seeing what lies ahead and what doesn’t, um, yeah, I don’t think that I would have taken ownership and I don’t think that I would be in the position that I am today. And I consider myself not to be in a bad position.
P2D1FG: This group showed me what success looks like…yeah, so I was starting to question that…you know, why am I beating myself up for not eating the things I like to eat, and just take pills to get rid of the spike, you know? And this group kind of turned it around.
Engagement in self-management behaviors
Participants reported that the intervention improved their diabetes management, including their intentions to make changes and set goals. Examples of goals set included portioning food, counting calories, and increasing exercise. Furthermore, participants felt accountable to other each other, which they said felt different from attempting to meet goals independently. One said, Saying it out loud, there’s a difference (P4D2IS), and another agreed Yeah, it stiffens your resolve when you’re actually sharing it with people so that’s one good thing about being here (P5D2IS).
P1D2IS: So, I guess my goal for diabetes, part of it is, um, that I need to add the walking on –actually, to add walking everyday on top of the swimming. Because I need to drop 20 pounds just to start off with the 20 pounds I put on two years ago, which I really bitterly regret.
P4D2IS: Well it’s a good time of year to do it!
P1D2IS: ……So that’s my goal.
The intervention also enabled participants to reflect on the lifestyle changes they had made during the intervention and report their achievements.
P5D2FG: Well, uh, as I said earlier, in fact, that, uh, having gone off coffee actually reduced my blood sugar levels in the mornings significantly. [That] was both surprising and pleasing and, um,… it may have come out of the fact that I was looking at more things in general about what I can do. I was, you know, we all want to come in with success stories, and the fact that it actually makes me feel good.
Discussion
The healthcare system currently offers few opportunities for individuals with diabetes to talk each other about their experiences and concerns. Venues to share stories, learn from, and connect with others living with the same disease may enhance chronic disease self-management. The categories identified in our study provide plausible mechanisms of how storytelling may lead to better self-management. Knowledge exchange, collaborative learning, reflection and making meaning all served to facilitate sharing information, experiences, and strategies of living with diabetes, which created opportunities for participates to learn from each other. Participants greatly valued peer-to-peer learning and through these processes a sense of community and peer support was nurtured, and participants felt a sense of trust and belonging with each other. In turn, these processes may shift attitudes towards empowerment, as participants discussed taking ownership of their disease management, and increasing engagement in self-management behaviors.
Processes of the storytelling intervention
People with chronic conditions are better self-managers if they know about their conditions, treatment options, medications, and how to prevent further deterioration.24,25 Throughout the storytelling intervention, participants often pooled their knowledge to better understand diabetes management and tried to solve problems they had encountered. Personal stories afford insights into real-world solutions that may not be offered by healthcare providers and that better reflect the complex experiences and contexts of peoples’ lives. 26 Storytelling interventions encourage participants to reflect on issues that they consider important, rather than those chosen for them by healthcare providers. 12 Practical, experience-based knowledge (e.g. the ‘how-to’ and ‘where-to’ strategies that our participants discussed) may be easier to implement. Greenhalgh et al. 20 reported similar results in their evaluation of a storytelling intervention and distinguished between abstract knowledge (‘knowing-that’) and practical understanding (‘knowing-how’) gained from sharing stories. Greenhalgh et al. proposed that nonadherence with diabetes self-management may relate to ‘not knowing how to’ rather than ‘not knowing what to do.’ Exchanging practical knowledge through storytelling may be more effective in improving self-management 12 than didactic or persuasive messaging in changing health behaviors. 27
In our study, hearing stories about varied participant experiences and perspectives helped them make sense of diabetes-management concepts and strategies. Like our observations, it has been noted that in both online and face-to-face diabetes support groups, the process of sharing information goes through a negotiation process before the participants arrived at an agreement. This process can result in an enhanced understanding of the topic. 28 The process of generating shared knowledge may help reinforce information for some, 29 and give new knowledge to others. Knowledge is noted as being most meaningful when discussed, repeated, reframed, or challenged by others. 7 The knowledge exchanged and the common understanding that is created becomes a reference and trusted experiential knowledge repository for participants. 28
Over time, participants began to show genuine commitment to making the sessions meaningful for themselves. This was evident in their level of enthusiasm and openness through self-reflection in telling their stories. They discussed their past lifestyle histories up to current management strategies that work for them. Reflections often help people realize or confirm that they need to make certain lifestyle changes 6 or examine how others’ stories can apply to themselves. 9 As participants collectively reflected, they construct their own understanding around an ideal way of managing diabetes. 28 Similarly, Goddu et al. also found that their storytelling intervention shaped participants’ perceptions of social norms about diabetes self-management. 11
Perceived benefits of the storytelling intervention
The intervention facilitated the creation of a community facilitating peer support, another common outcome reported in storytelling interventions.14,19,30 Sharing stories connects people9,11,12 as stories validate the common experiences of living with the disease. Providing participants with an opportunity or forum to recognize their experiences in other people’s stories instilled a sense of belonging, nurturing a ‘team’ outlook, a team that participants frequently used as they banded together to share, learn, discuss, and set goals toward better self-management. They differentiated this support from that received from family members and friends, as many did not want to burden their families with their concerns, as such some participants described feeling isolated in managing their diabetes before the intervention. The intervention left participants with a more optimistic attitude towards self-management as they felt they were not it in alone.
Participants also constructed a positive collective identity of living with the disease. 31 These findings resemble those of Stuckey et al., who reported that their participants often put a positive spin on their disease and its management. 27 Similarly, Koch and Kralik also found that some of their participants viewed living with diabetes as a positive turning point in their lives, because the diagnosis motivated them to take better care of themselves and change their lifestyles. 18 Furthermore, storytelling interventions can accelerate this positive change in attitude through construction of healthy self-identity by adopting the self-care behaviors modeled in people’s stories. 32
Storytelling may be more effective than traditional approaches to changing health behaviors, 26 given the peer modeling that naturally occurs. According to Bandura’s theory of observational learning, people use others as models in developing their knowledge, forming new attitudes, and changing their behaviors,33,34 particularly when referents are similar to themselves. 35 Hearing from experienced participants overcoming similar challenges can inspire patients to become more proactive in their management.28,36 Our participants said they were inspired by others’ successes and that the intervention encouraged and enabled them to better manage their diabetes. As in our results, Goddu et al. found that peer support changed participants’ attitudes and beliefs, about diabetes self-management. 11
Loss of motivation is common over the years after diagnosis of a chronic illness 37 and effective self-managers need to actively manage their illness, feel confident in their ability to do so, and interact with their care providers to solve self-management problems.24,25 Our participants reported focusing more on self-management as the intervention progressed. For those who had lived longer with diabetes, the sessions renewed motivation. Participants took initiative to set and share their management goals and report back on their challenges and achievements. Although goal-setting, an effective strategy for diabetes management, 38 is not unique to storytelling interventions, the group setting may have enhanced participants’ motivation to complete goals because participants felt accountable to the group. We also found, as did Goddu et al., 11 that storytelling interventions may increase participants’ intent to discuss issues that arose during discussions with healthcare professionals.
Self-reported positive changes in weight and blood glucose during the intervention were noted by participants. Likewise, Goddu et al. found that participants reported that sharing stories boosted their self-confidence and encouraged them to make diabetes-related behavior changes. 11 Storytelling interventions can empower and encourage more self-awareness to make lifestyle changes, take ownership of diabetes, and seek professional advice when needed. These benefits can help participants not let their diabetes define them, but rather, give them confidence in managing while living their everyday lives. 24
Overall, greater understanding of diabetes and its management can enhance management control, leaving individuals better able to focus on real, rather than perceived or unknown, components of their disease. 39 However, given that our intervention was patient led, it may not have covered all topics clinically relevant to self-management, 13 and not all the information shared was accurate or applicable to others. Therefore, it is important that patient-led interventions include clinical facilitators who can answer questions and correct clinically inaccurate information.
Limitation
Our study included a small sample of eight people with homogenous demographics which may have enhanced the cohesiveness and willingness to share among participants. However, themes we have identified and are also supported by other published storytelling interventions.11,12 Although our research participants were all English speaking, older than 50, predominantly female and Caucasian, and may not reflect experiences of younger people of different racial backgrounds; other published storytelling interventions discussed11,12 represent primarily older female of various racial minorities in their samples. Therefore, further research with male or younger participants would be helpful to support the transferability of our findings to a larger population. Yet, not all people will be attracted to this type of intervention as people may not be willing to share their personal stories with others. For example, women are more likely to use diabetes resources that are socially interactive such as support groups while men favor more self-directed and independent resources. 40
Conclusions
Health systems need to be held accountable for helping people learn how to self-manage diabetes and for providing ongoing support after initial self-management education. Our study provides insight into the attributes of group storytelling, that may enhance disease self-management. The identified processes and perceived benefits provide the mechanisms of how storytelling may lead to better self-management. Knowledge of the processes involved in storytelling could be helpful in supporting health care professionals in offering such interventions by facilitating or creating opportunities for collaborative learning. Whereas the perceived benefits could help in directing the design and evaluation of future storytelling interventions, by identifying potential outcomes to measure and evaluate.
Footnotes
Acknowledgements
Anna Richardson, Stephanie Arresta and Iana Mologuina assisted with data management and analysis. Margaret Oldfield and Linn Clark edited the paper.
Contributorship
The following are the contribution of the authors to this study: Conceptualization: EG, GK, SS, HB; Funding acquisition: EG, GK, SS, HB; Project administration: EG, GK; Methodology: EG, SS, HB; Formal analysis: EG, ER, SS, HB, SE; Writing – original draft: EG, ER; Writing – review & editing: EG, ER, GK, SE, HB.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study protocol was approved by Ryerson University Research Ethics Board (REB 2013–258.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ryerson University Health Research Fund and the University’s Faculty of Community Services Writing Week program.
Guarantor
EG.
Informed consent
Written informed consent was obtained from the participants.