
Abstract
Introduction:
To perform a systematic review of the diagnostic accuracy of point-of-care lung ultrasound, compared to chest radiography, in children and young people (0–21 years) who present to ambulatory settings with suspected community-acquired pneumonia.
Methods:
Registration: Prospero June 2021 CRD42021260552. Electronic searching performed on Medline, Embase, CINAHL and Science Citation Index from inception to 20 June 2023. Two researchers independently screened titles, abstracts, and full texts for study selection. Risk of bias was assessed using the Quality Assessment Tool for Diagnostic Accuracy Studies (QUADAS-2) tool. Meta-analysis of included studies.
Results:
The six studies included in this systematic review described point-of-care lung ultrasound performed primarily by paediatric emergency medicine clinicians on a total of 1099 paediatric patients, with a reference standard of chest radiography or chest radiography with clinical findings. The majority of included studies lacked clarity on training for the index test with potential bias around flow and timing of testing. Meta-analysis of the combined results of the included six studies calculated a pooled sensitivity of 90.9% (95% CI [85.5%, 94.4%]) and pooled specificity of 80.7% (95% CI [63.6%, 91.0%]).
Conclusions:
Point-of-care lung ultrasound has high sensitivity but lower specificity to diagnose acute pneumonia in children. Further research is needed which overcomes issues around training in point-of-care lung ultrasound, study design and reliability of the reference test (chest radiography) to better evidence the role of point-of-care lung ultrasound in diagnosing pneumonia in children in ambulatory and resource-limited settings.
Introduction
The British Thoracic Society (BTS) advises bacterial pneumonia is a likely diagnosis in a child presenting with fever, chest recession and tachypnoea, although viruses and more rarely fungi are also aetiological agents.1,2 Pneumonia accounts for 14% of all deaths in children under the age of 5, 3 with 90% of these deaths occurring in low-income countries. 4 There are still around 2.5 million cases of paediatric pneumonia in high-income countries each year, of which 30%–50% result in hospitalisation.1,5
BTS guidelines recommend against the routine use of chest radiographs (CXR) or blood tests to diagnose pneumonia in children, with CXRs recommended only when the diagnosis is in doubt, or if the child is severely unwell. 6 However, CXR is used in up to 73% of children with suspected pneumonia,7,8 potentially exposing them to unnecessary ionising radiation, despite being a cohort more radiosensitive when compared to adults. 9 CXR is also time-intensive for clinicians, quality dependent on child behaviour and posture, with interpretation susceptible to considerable intra- and inter-observer variation.8,10
Lung ultrasound (LUS) at the point-of-care, or POC LUS, could offer an alternative diagnostic approach and potentially reduce the number of CXRs in children. 11 It is effective in children who have a smaller lung volume and thoracic diameter, allowing easier visualisation of lung consolidation. 12
LUS can be performed concurrently with a physical examination 13 and can be taught relatively quickly to clinicians without ultrasound experience. 14 The International Liaison Committee on Lung Ultrasound considers LUS a basic sonographic technique 15 which clinicians can interpret accurately after 25 scans. 16 Point-of-care ultrasound is portable or handheld and can be done at the bedside by the attending physician, which allows for immediate interpretation and management, which would also be ideal for community and resource-limited settings.
Despite evidence supporting the use of POC LUS,17–19 no current guidelines recommend its use. The aim of this study was to perform a systematic review of the available evidence for the diagnostic accuracy of point-of-care LUS when performed by a clinician in an acute setting, compared to a standard CXR for pneumonia in children.
Methods
Reporting of this systematic review follows the diagnostic test accuracy extension of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-DTA) statement, 20 with the PRISMA checklist submitted with the manuscript. The review was registered with Prospero June 2021, number CRD42021260552.
Eligibility criteria and definitions
Studies were considered for inclusion if the study population included children and young adults between the ages of 0 and 21 (accounting for variation in age cut-offs of paediatric services globally) presenting with suspected pneumonia to ambulatory care settings including primary care clinics, hospital outpatient clinics, emergency departments, walk-in centres and acute clinics in resource-limited regions. If studies included adults and children, only studies that distinguished quantitative outcomes for children alone were considered.
The index test was any POC LUS used with real-time analysis to detect lung consolidation. The ultrasound could be conducted by any frontline clinician managing sick children who was not exclusively a professional sonographer or radiographer. We originally defined sufficient experience as a minimum of 25 scans, as recommended by the American College of Emergency Physicians 16 but found this made the inclusion criteria too narrow. The adjusted inclusion criteria considered studies that described clinician training had taken place, even in cases where the number of scans attempted before the study was not disclosed or the recommended 25 scan benchmark was not met. The reference standard considered was a CXR or CXR in combination with clinical findings. Studies that did not report individual patient-level diagnostic results were excluded.
Search strategy
Medline, Embase, CINAHL and Science Citation Index were searched from inception to 20 June 2023 with no language restrictions. The search, which also included ultrasound for diagnoses other than pneumonia, included the following terms: (children OR adolescent OR infant) AND (ultrasonography) AND (point-of-care OR hand-held OR portable). The full search strategy can be seen in Supplemental Online Material 1. From this broader search we identified studies that met our inclusion criteria for this study focused on LUS for pneumonia.
Study selection
We included retrospective and prospective cohort studies meeting our inclusion criteria. Two independent reviewers identified the relevant studies by reading titles and abstracts (H.H.-D., C.B.). Disagreements were arbitrated by a third reviewer (U.U.). Full text for the studies was retrieved when both reviewers agreed a study was relevant or if there was insufficient information in the abstract to form a judgement. The full text of the studies was reviewed to judge eligibility.
Data extraction and quality assessment
One reviewer extracted data from the selected studies using a data extraction form (H.H.-D.), which was then checked by a second reviewer (U.U.), with any disagreements adjudicated by a third reviewer (C.B.). Extraction included study characteristics, participants, index and reference test and results. Contact was attempted with authors whose studies did not provide all the required details. Both reviewers used the QUADAS-2 tool21,22 to assess the quality of studies. Disagreements were decided by the third, independent reviewer.
Data analysis
Data for diagnostic accuracy was summarised in a 2 × 2 classification table, where LUS was the index test and CXR the reference test, to categorise patients with or without pneumonia. A random effects bivariate meta-analysis model 23 was fitted using the R package ‘mada’ to calculate pooled sensitivities and specificities, with a continuity correction of 0.5 applied to studies with zero counts. 24 The primary analysis used all studies. We planned to perform a subgroup analysis using only studies that reached the threshold for sufficient clinician experience, but this was not possible because too few studies were found that met this threshold.
Patient and public involvement (PPI)
The planned systematic review was presented to the NIHR Community Healthcare MIC, Oxford’s PPI group for acute paediatrics in 2021 who deemed the research was relevant to diagnostics used in the delivery of acute child health.
Results
Study characteristics and definitions
The search identified 6461 studies, of which 3698 were excluded due to being duplicates, case reports, conference abstracts or animal studies (Medline – 2006, Embase – 1919, CINAHL – 948, Science citation index – 1588). Of the 2763 studies then screened, six were eligible for inclusion in the systematic review8,25–29 (see PRISMA flow diagram, Figure 1). 30
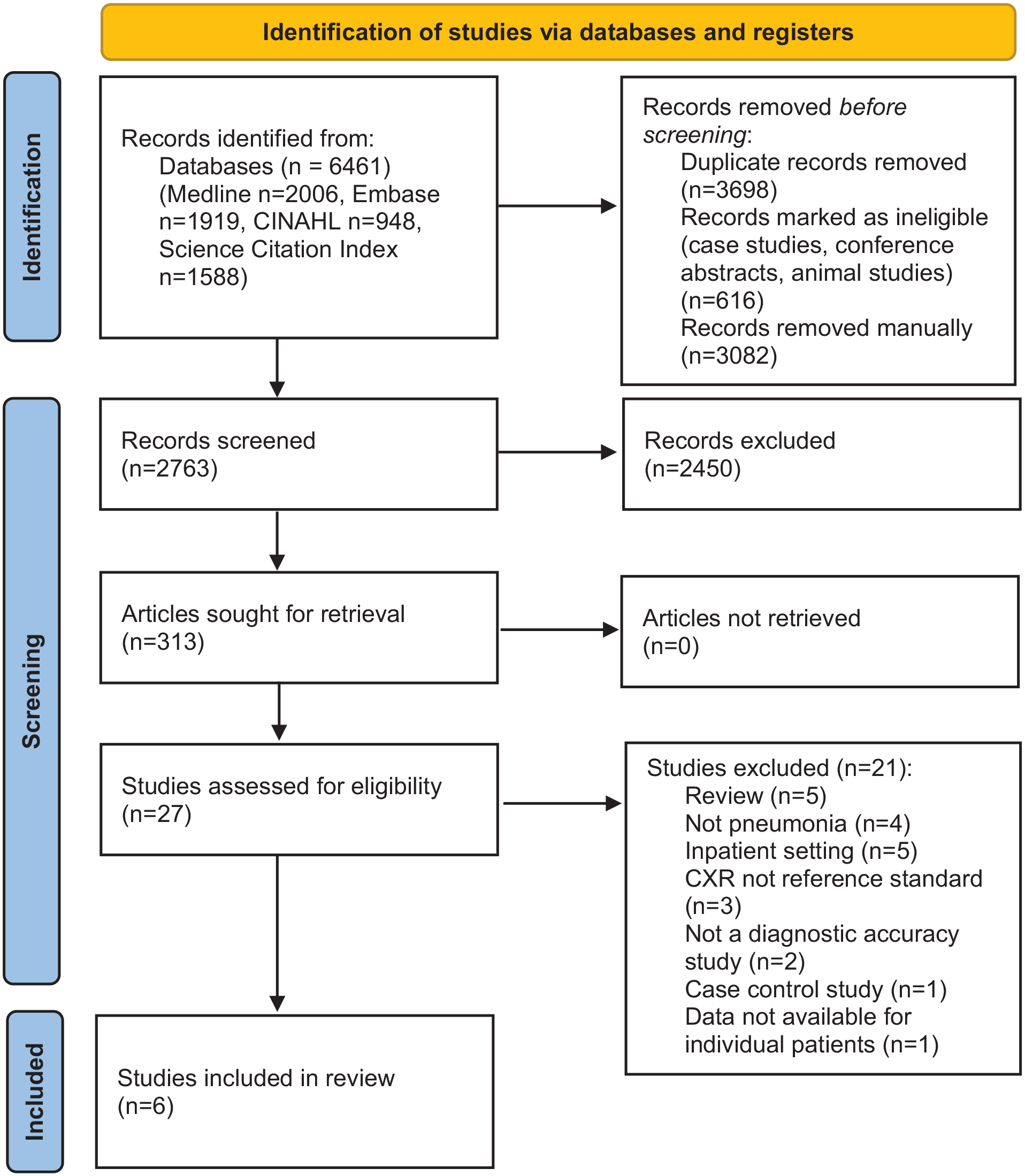
PRISMA 2020 flow diagram for diagnostic accuracy of point-of-care lung ultrasound for community-acquired pneumonia in children in ambulatory settings: a systematic review and meta-analysis.
Table 1 provides a summary of study characteristics. All were prospective observational studies (total sample size 1099 patients). Five of the six studies were conducted in children’s EDs,8,25,26,28,29 one of which was in a resource-limited setting, 29 while the remaining study took place in primary care. 27 Participant recruitment methods included convenience sampling8,26,28 and consecutive sampling, 27 although sampling methods for two studies were unclear.25,29 The average age (reported as either mean or median) in the included studies ranged from 1.3 to 8.9 years. The percentage of male participants was close to 50% in all studies, where reported, and the prevalence of pneumonia ranged from 18% to 92%.
Summary study characteristics.
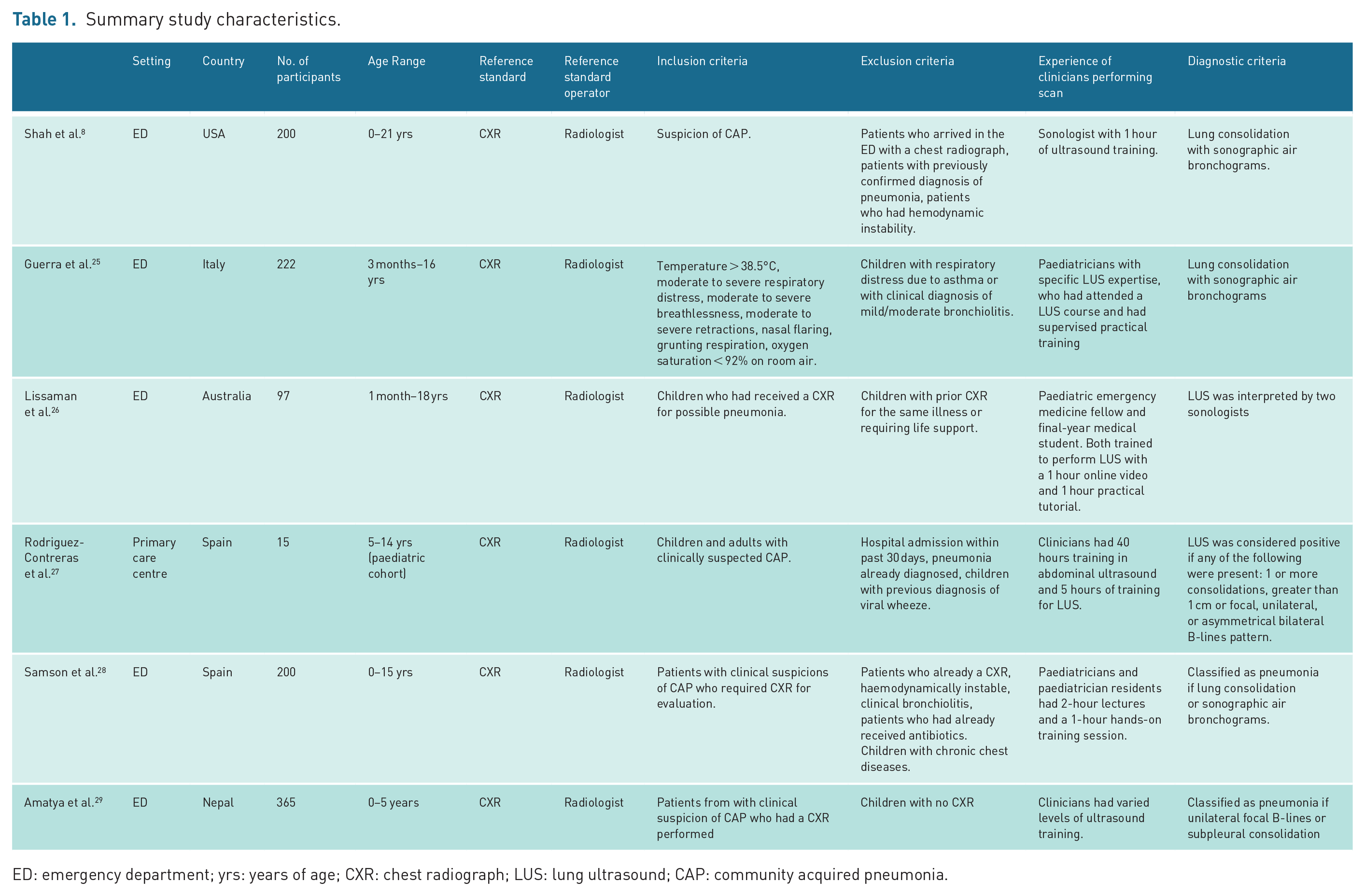
ED: emergency department; yrs: years of age; CXR: chest radiograph; LUS: lung ultrasound; CAP: community acquired pneumonia.
Training for frontline clinicians varied from an hour-long programme (consisting of a lecture and practical session) to 5 hours of training, although two studies provided insufficient detail around LUS training and experience.25,29 Ultrasound probe type and frequency varied between studies and included the use of a curvilinear probe, 29 convex probe 25 or a linear probe with 3.5–5, 25 7.5–10,8,25 8–14 27 and 6–15 MHz range of frequencies reported. 28 Two of the included studies were unclear about the range of the frequency of the transducer26,29 (see Table 4). All studies used real-time evaluation and defined lung consolidation (an area where air is replaced by fluid and presses on the pleural surface) as a sign of pneumonia on CXR. For all studies, the reference test was CXR interpreted by either a radiologist or a patient-facing clinician.
Study quality
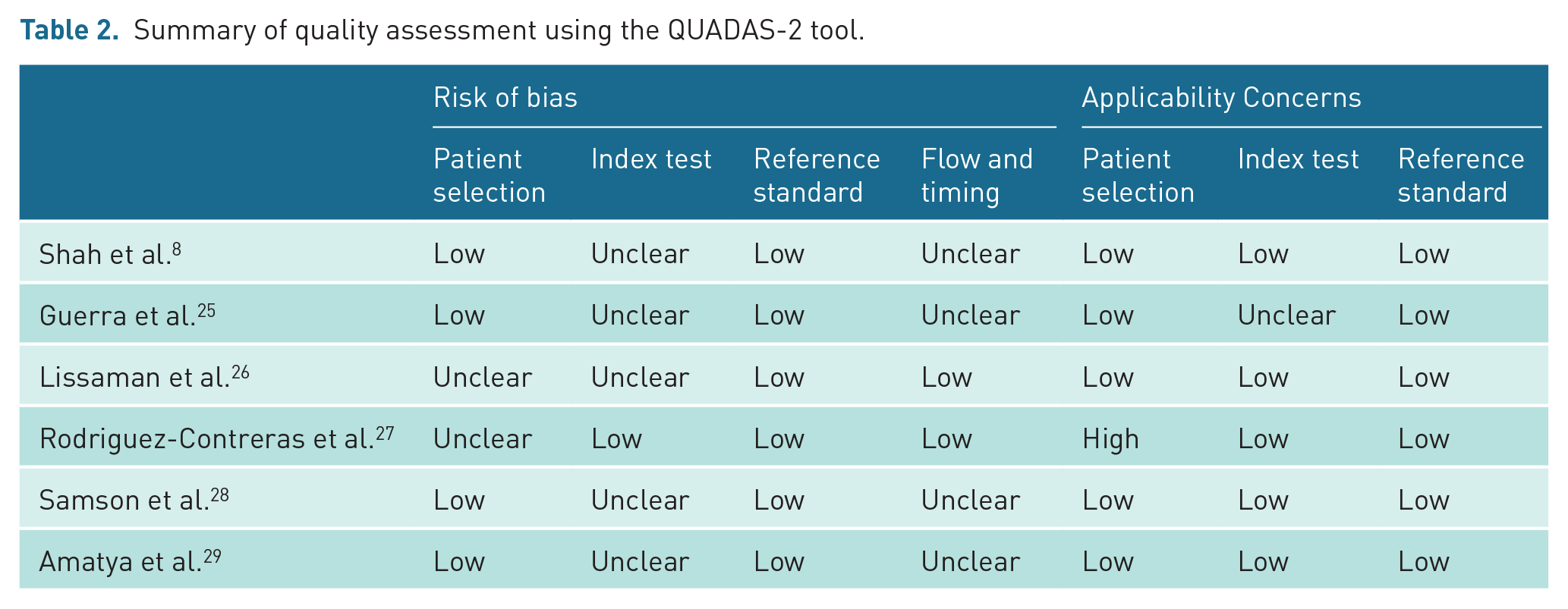
Table 2 summarises the QUADAS-2 quality assessment (full review can be found in Supplemental Online Material 3). One study excluded children under 5 years of age, a cohort who commonly present with pneumonia, meaning applicability concerns were high for patient selection. 27 Five of the six included studies did not meet our review’s original 25-scan experience threshold for inclusion (results for diagnostic accuracy are separated out by experience in Table 3).8,25,26,28,29 Rodriguez-Contreras et al.’s study was the only one at low risk of bias for the index test as it detailed sufficient experience with scanning (> 25 scans). 27
Summary of quality assessment using the QUADAS-2 tool.
Diagnostic accuracy results from included studies, with data presented to differentiate between clinicians experienced in POC LUS and inexperienced clinicians.
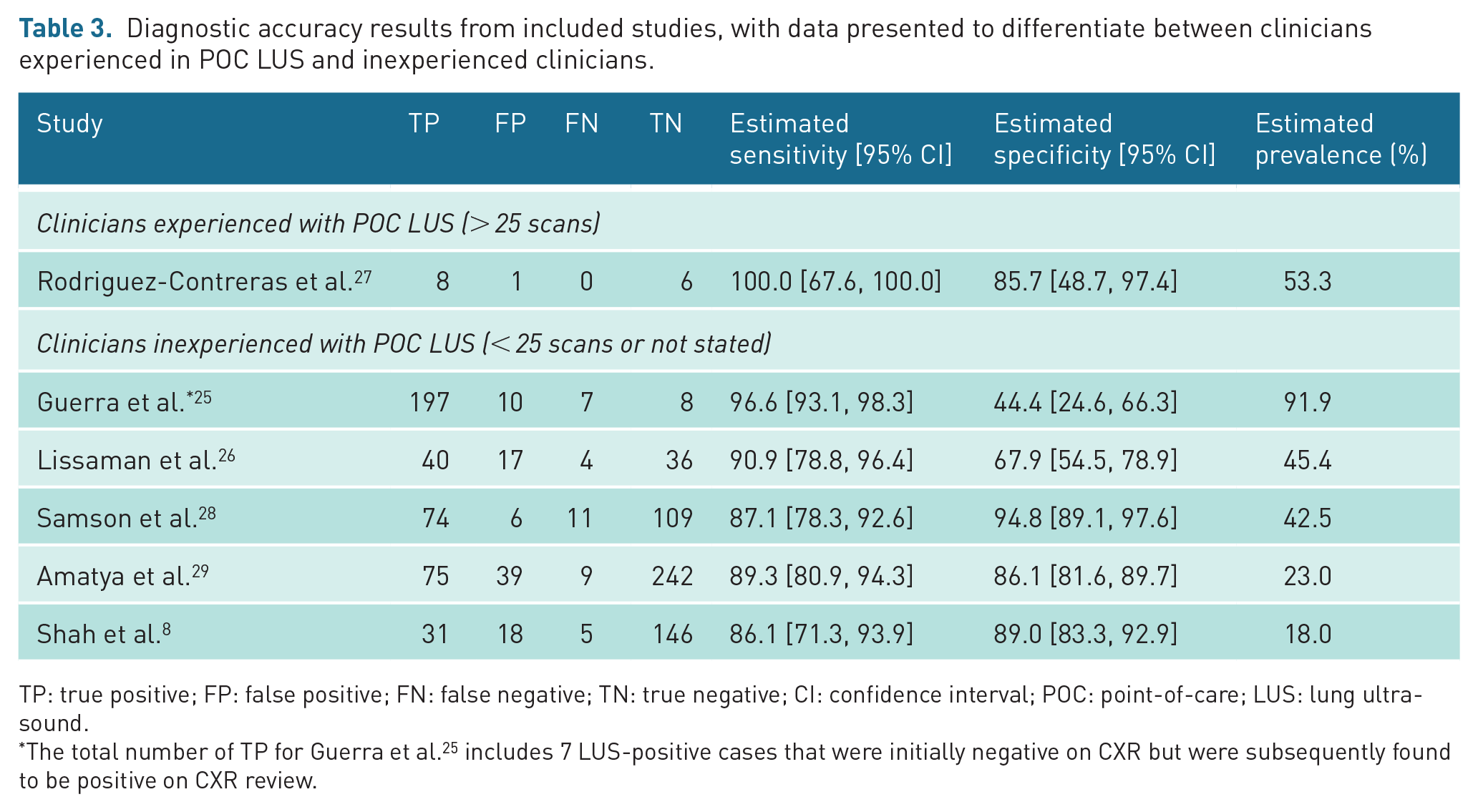
TP: true positive; FP: false positive; FN: false negative; TN: true negative; CI: confidence interval; POC: point-of-care; LUS: lung ultrasound.
The total number of TP for Guerra et al. 25 includes 7 LUS-positive cases that were initially negative on CXR but were subsequently found to be positive on CXR review.
All six studies had low risk of bias and low applicability concerns for conduct and interpretation of the reference standard as they ensured the clinicians interpreting the CXR were blinded to the results of the LUS. However, four of the six studies had unclear risk of bias for flow and timing as they did not specify time between performing ultrasonography and chest radiography.8,25,28,29
Diagnostic accuracy
Table 3 and Figure 2 (forest plot) detail the diagnostic accuracy estimates for the six included studies. All studies had an estimated sensitivity above 86%. The range was from 86.1% to 100%, although the highest sensitivity came from a study including only 15 children. 27 Specificity varied more than sensitivity, with a range from 44.4% to 94.8%. Prevalence of pneumonia in the included patients also varied from 18% to 92%.
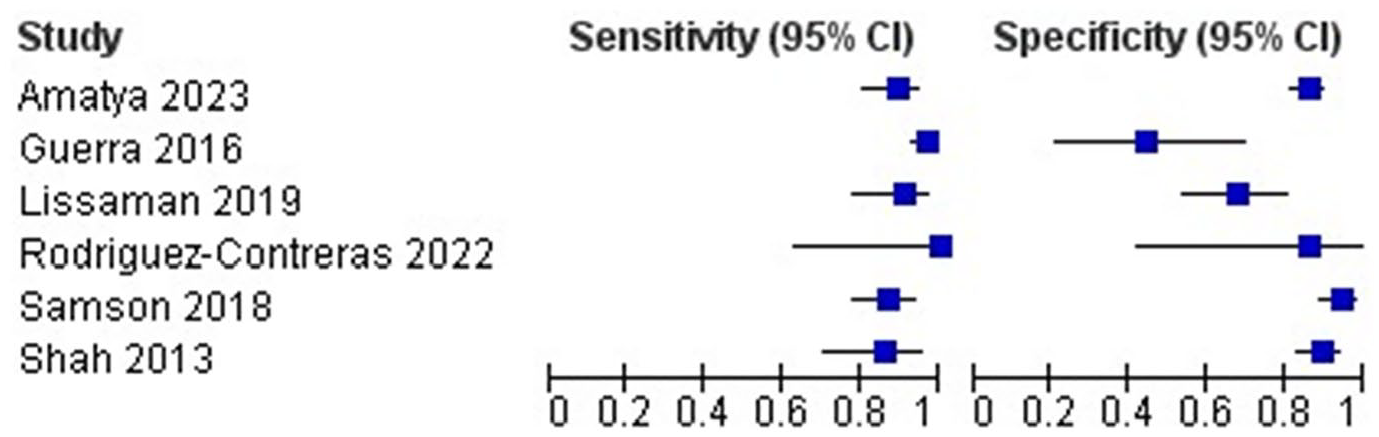
Forest plot of included studies.
Meta-analysis
We pooled all six studies that met our inclusion criteria. The pooled sensitivity was 90.9% (95% CI [85.5%, 94.4%]) and the pooled specificity was 80.7% (95% CI [63.6%, 91.0%]). As a meta-analysis of diagnostic accuracy studies, there is no widely used measure of heterogeneity, although this study found high heterogeneity in the pooled specificity estimate while we also observed considerable methodological heterogeneity in the different study designs.
Discussion
Summary of results
In six studies compromising 1099 children with suspected pneumonia attending EDs (one in a resource-limited setting) and one primary care centre, LUS had high sensitivity but lower specificity for diagnosing pneumonia as identified by CXR. The high pooled sensitivity (90.9%) suggests POC LUS, even with the small amount of training provided to clinicians involved in these studies, could be an effective tool for frontline clinicians to identify community-acquired pneumonia (CAP) in children instead of CXR. However, our pooled specificity is lower (80.7%). Depending on how often a CXR result is believed by clinicians to confirm the absence of bacterial pneumonia 31 low specificity could lead to more children receiving unnecessary antibiotics.
Strengths and limitations
Strengths
This prospectively registered review was conducted following best practice with a thorough search of the literature. The study protocol screened for studies in ambulatory, acute settings, with POC LUS carried out by non-radiologists/sonographers, whereas previous studies have focused on inpatient and intensive care settings, often with radiologist/sonologist operators, making this study more relevant to a wider patient population, particularly for resource-limited settings.
Limitations
The main limitation of this review is the quality and number of studies available on this topic. Only six studies met our inclusion criteria. Only one of the included studies evaluated the use of POC LUS in a resource-limited setting 29 where the need is greatest and only one small study was set in primary care, where imaging could help avoid onward referrals. 27 Our results are best interpreted in the context of a well-resourced children’s ED.
The pooled specificity was lower than the pooled sensitivity, with heterogeneity between studies. One explanation could be the limitations of the CXR as a reference standard. CXRs cannot identify small consolidations, which may have resulted in POC LUS identifying smaller consolidations which were subsequently classified as false positives when compared to CXR. 7 When Shah et al. 8 performed a subgroup analysis excluding lung consolidations less than 1 cm in diameter, sensitivity remained the same at 86% but specificity increased from 89% to 97%. Furthermore, while traditionally epidemiology and diagnostic accuracy studies for CAP have used CXR as the reference standard, many national guidelines no longer advocate CXRs routinely in the diagnosis of CAP, relying more on clinical findings. 1 Reali et al. 32 combined CXR with clinical findings as the reference standard for patients already admitted to hospital. This study did not meet our inclusion criteria as it included patients admitted to hospital. It found a specificity of 96%, higher than our pooled specificity, but admitted patients would be more likely to have positive findings on CXR.
The studies included in this review used varying ultrasound devices with different probe types and associated frequencies, further contributing to heterogeneity between studies. The range of frequencies determines the depth of penetration as well as image quality (with low frequencies penetrating deeper with the caveat of lower image quality), while the shape (curvilinear or linear) can determine the shape of image captured (see Table 4). 33
Ultrasound device used, transducer frequency and probe type.
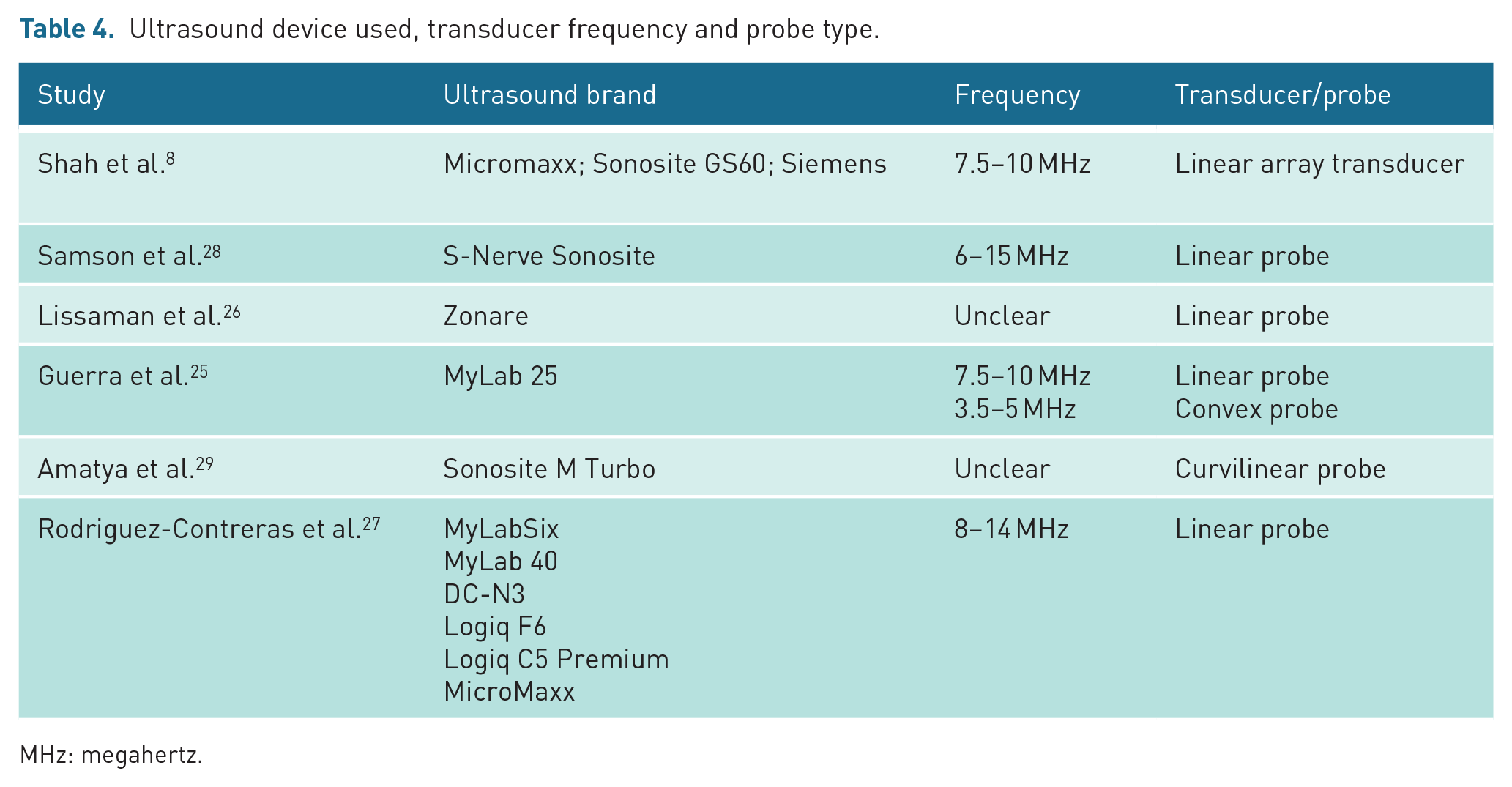
MHz: megahertz.
Comparison with the literature
Our pooled sensitivity is supported by recent meta-analyses of POC LUS which report sensitivities of 94% 17 and 96% 18 in paediatric populations. Compared to our results, these reviews reported slightly higher specificities of 93% and 90%, respectively, although some of these studies used LUS performed by radiographers rather than POC LUS performed by front line clinicians and included hospitalised, neonatal and critically ill patients, who have a higher likelihood of positive findings for CAP on both CXR and POC LUS.
Implications for research and practice
Our results demonstrate a potential role for LUS to diagnose CAP in children in ambulatory and resource-limited settings. While CXR remains the current reference standard in most clinical settings, it has limited sensitivity and specificity. Ultrasound devices offer greater agility as they can be deployed at the bedside, avoid risks associated with ionising radiation, which are notably higher for paediatric populations, and are an inexpensive diagnostic modality when compared to CXR.29,34 However, our lower pooled specificity means further study is required in populations of patients where POC LUS is likely to add most value. Further investigation is needed before use in children with acute respiratory infections, to ensure robust evaluation of POC LUS’ effect on antibiotic prescribing (e.g. POC LUS’ greater sensitivity might lead to unnecessary antibiotic use for viral infections) and hospital referral/admission.
Particular attention in new studies should be given to defining appropriate training in LUS for clinicians and defining a reference standard more closely representative of clinical practice in primary care and resource-limited settings. In these contexts where there may be greater emphasis on clinical findings alongside CXR, recruiting an appropriate sample size to detect a meaningful effect, and using inclusion criteria that better reflect undifferentiated acute respiratory illness in children will provide research findings that are more able to be practically applied.
Studies of children presenting to primary care and resource-limited settings could lead to wider adoption of POC LUS outside well-resourced hospital settings.
Conclusion
POC LUS for diagnosing paediatric pneumonia has a high pooled sensitivity but lower specificity in ambulatory settings, including a resource-limited setting. Better designed studies are needed to understand performance and likely impact of this new technology across frontline paediatric settings, particularly on antibiotic stewardship.
Supplemental Material
sj-docx-1-ult-10.1177_1742271X241289726 – Supplemental material for Diagnostic accuracy of point-of-care lung ultrasound for community-acquired pneumonia in children in ambulatory settings: A systematic review and meta-analysis
Supplemental material, sj-docx-1-ult-10.1177_1742271X241289726 for Diagnostic accuracy of point-of-care lung ultrasound for community-acquired pneumonia in children in ambulatory settings: A systematic review and meta-analysis by Helena Hughes-Davies, Umasha Ukwatte, Thomas R Fanshawe, Nia Roberts, Philip J Turner, Gail N Hayward and Chris Bird in Ultrasound
Supplemental Material
sj-docx-2-ult-10.1177_1742271X241289726 – Supplemental material for Diagnostic accuracy of point-of-care lung ultrasound for community-acquired pneumonia in children in ambulatory settings: A systematic review and meta-analysis
Supplemental material, sj-docx-2-ult-10.1177_1742271X241289726 for Diagnostic accuracy of point-of-care lung ultrasound for community-acquired pneumonia in children in ambulatory settings: A systematic review and meta-analysis by Helena Hughes-Davies, Umasha Ukwatte, Thomas R Fanshawe, Nia Roberts, Philip J Turner, Gail N Hayward and Chris Bird in Ultrasound
Footnotes
Contributors
G.N.H., P.J.T. and C.B. conceptualised the study and contributed to the study protocol written by H.H.-D. N.R., the study librarian, performed the literature search. H.H.-D. and C.B. screened abstracts and then with U.U., extracted relevant studies and performed quality assessment on included studies. T.R.F., the study statistician, calculated the diagnostic accuracy and forest plots in the results section. C.B., H.H.-D. and U.U. drafted the manuscript. All authors contributed to subsequent drafts and all contributed to analysis and interpretation of the study’s results.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work received funding from the NIHR Community Healthcare MedTech and In Vitro Diagnostics Co-operative at Oxford Health NHS Foundation Trust (MIC-2016-018). T.R.F. also received funding from the NIHR Applied Research Collaboration Oxford and Thames Valley at Oxford Health NHS Foundation Trust. No funding party had a role in the design of this study, interpretation of the data, or decision to submit results. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health and Social Care.
Ethics approval
As this was a systematic review and meta-analysis of previously peer-reviewed and published studies, ethical approval was not required.
Permission from patient(s) or subject(s) obtained in writing for publishing their case report
No – not applicable as not a case report.
Permission obtained in writing from patient or any person whose photo is included for publishing their photographs and images
No – not applicable.
Confirm that you are aware that permission from a previous publisher for reproducing any previously published material will be required should your article be accepted for publication and that you will be responsible for obtaining that permission
No – not applicable.
Guarantor
Christopher Bird.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.