
Abstract
Background:
There is growing evidence to support the use of ultrasound as a tool for the assessment and treatment of speech, voice and swallowing disorders across the Speech and Language Therapy profession. Research has shown that development of training competencies, engagement with employers and the professional body are vital to progressing ultrasound into practice.
Methods:
We present a framework to support translation of ultrasound into Speech and Language Therapy. The framework comprises three elements: (1) scope of practice, (2) education and competency and (3) governance. These elements align to provide a foundation for sustainable and high-quality ultrasound application across the profession.
Results:
Scope of practice includes the tissues to be imaged, the clinical and sonographic differentials and subsequent clinical decision-making. Defining this provides transformational clarity to Speech and Language Therapists, other imaging professionals and those designing care pathways. Education and competency are explicitly aligned with the scope of practice and include requisite training content and mechanisms for supervision/support from an appropriately trained individual in this area. Governance elements include legal, professional and insurance considerations. Quality assurance recommendations include data protection, storage of images, testing of ultrasound devices as well as continuous professional development and access to a second opinion.
Conclusion:
The framework provides an adaptable model for supporting expansion of ultrasound across a range of Speech and Language Therapy specialities. By taking an integrated approach, this multifaceted solution provides the foundation for those with speech, voice and swallowing disorders to benefit from advances in imaging-informed healthcare.
Introduction
The use of ultrasound (US) imaging outside of traditional radiology settings is an area of rapid growth. In the Speech and Language Therapy (SLT) profession, there is growing evidence to support its application as a tool for the assessment and treatment of speech and swallowing disorders.1 –4
There are fundamental constraints to integration of US into SLT clinical practice such as cost, availability of equipment and lack of focused training.2,5 There is, however, a drive among the profession to start adopting US into practice while research to establish reliability of data acquisition and interpretation continues. To do this, mechanisms to address concerns around competency and scope of practice are required.
US imaging is a modality that requires experience to use and interpret. The skill and experience required by Speech and Language Therapists (SLTs) will vary according to the purpose for which US is being used. The paper uses a framework to describe the scope of practice, education and governance requirements associated with application of US in the profession. This has been used in other allied health professional (AHP) groups in the emerging areas of lung 6 and pelvic health 7 to address concerns such as quality assurance and professional indemnity. This paper therefore shares some generic content with these publications,6,7 which in turn overlaps with relevant professional guidance.8,9
Speech & language therapists
In the United Kingdom, SLTs are autonomous clinicians who hold a formal qualification as a speech and language therapist. Typically, this will be a minimum of a BSc (Hons) Clinical Communication Studies/Speech Pathology and Therapy or post-graduate equivalent (e.g. MMedSci Clinical Communication Studies). Combined with their professional registration with the Health and Care Professions Council (HCPC), they can use the protected title of ‘Speech and Language Therapist’ and are eligible to join the professional body ‘The Royal College of Speech and Language Therapists (RCSLT)’.
SLTs work across a range of patient and client groups across the lifespan (the term patient will henceforth refer to both patients and clients). Their key responsibilities include the assessment, management and monitoring of swallowing and communication, including speech disorders. Assessment includes clinical history-taking alongside a combination of assessment procedures. For swallowing, assessments may include a clinical bedside assessment or instrumental assessment via videofluoroscopic swallowing study (VFSS) or flexible endoscopic evaluation of swallowing (FEES), whereas assessment of both speech and voice quality may include perceptual, acoustic, and instrumental analysis, for example, electropalatography 10 and vocal acoustic analysis. 11 Applying a combination of clinical reasoning and patient-centred care, SLTs independently formulate and apply treatment approaches such as exercises to target the underlying speech, voice, or swallowing disorder and/or strategies to reduce the functional impact of the impairment.
SLTs work closely with other professionals such as radiologists, audiologists, ear, nose and throat specialists, intensivists, neurologists, respiratory physicians and physiotherapists to enable interdisciplinary assessment and management of speech, voice and swallowing disorders. In this regard, there may be a degree of overlap with, and aspects of this framework may apply to, other professional groups.
Applications of US across SLT
There are several possible applications of US across the SLT profession. Some applications, such as use of US for biofeedback in speech disorder intervention, are an already established part of clinical practice in some areas of the United Kingdom. 12 Other applications, such as its use as a tool to assess dysphagia, remain solely in the research setting. Current and potential application of US across the profession, plus research evidence, have previously been described13,14 and are summarised according to SLT role across the full range of patient clinical presentations in Table 1.
Aims and role of speech and language therapy for speech, voice and swallowing presentations, including ultrasound role.
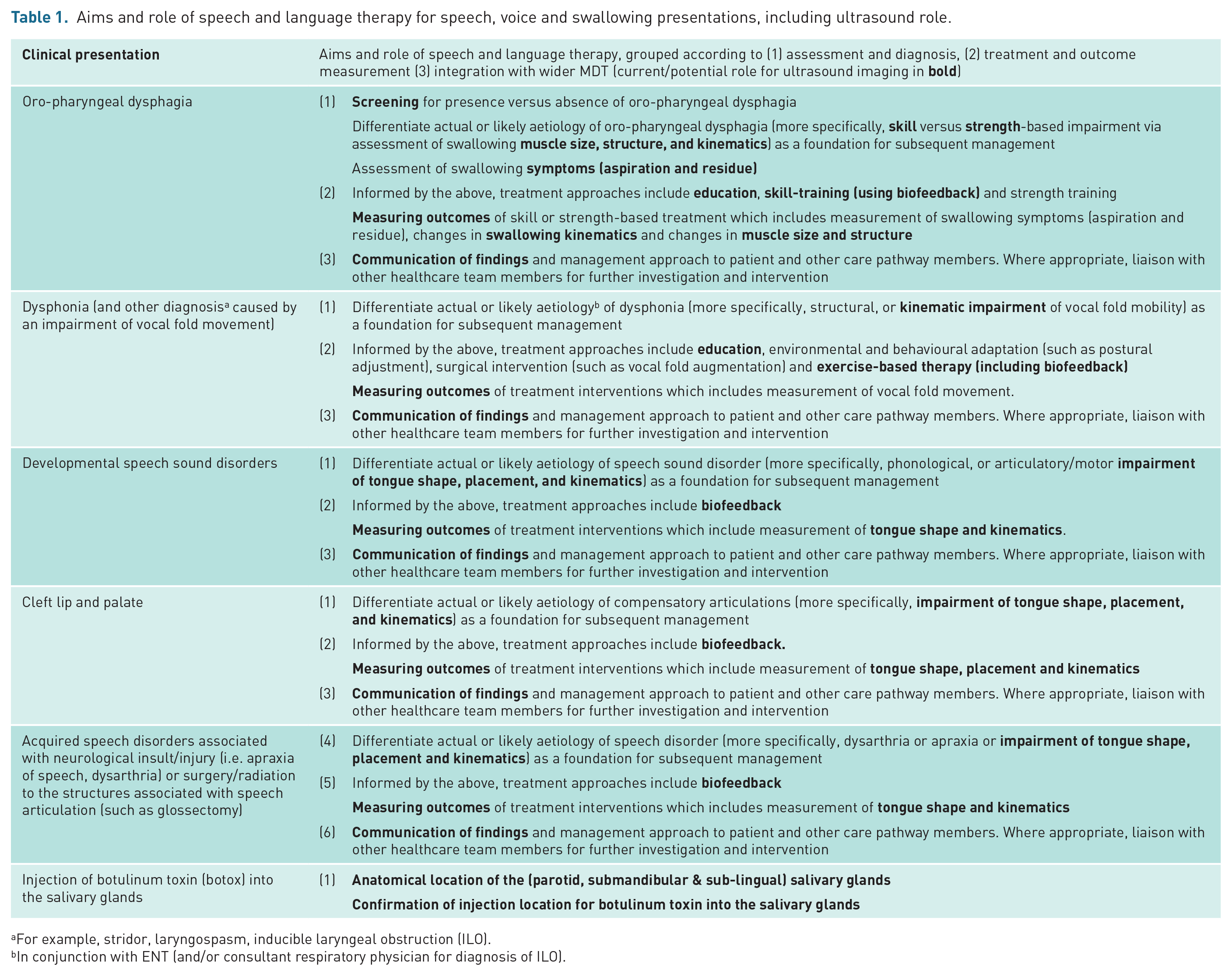
For example, stridor, laryngospasm, inducible laryngeal obstruction (ILO).
In conjunction with ENT (and/or consultant respiratory physician for diagnosis of ILO).
In order to define SLT scope of practice, education and governance, the applications described in Table 1 have been categorised into three domains. These are
Static imaging of speech, voice, and swallowing structures
Qualitative evaluation of speech, voice and swallowing movement
Quantitative analysis of speech, voice and swallowing movement
The three domains are described in Table 2.
Applications of ultrasound across speech and language therapy divided into three domains: (1) static imaging of speech, voice and swallowing structures; (2) qualitative evaluation of speech, voice and swallowing movement; (3) quantitative analysis of speech, voice, and swallowing movement.
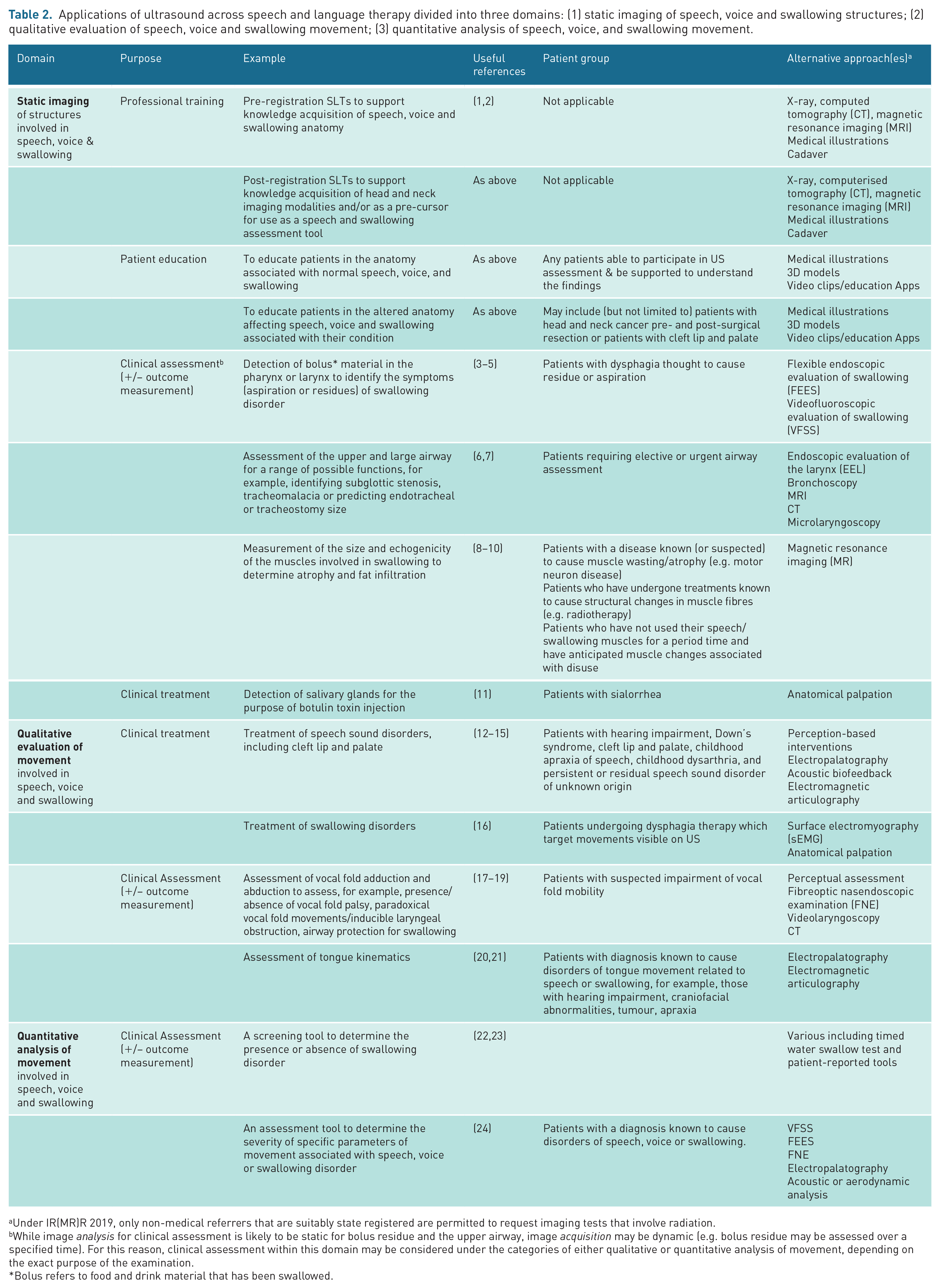
Under IR(MR)R 2019, only non-medical referrers that are suitably state registered are permitted to request imaging tests that involve radiation.
While image analysis for clinical assessment is likely to be static for bolus residue and the upper airway, image acquisition may be dynamic (e.g. bolus residue may be assessed over a specified time). For this reason, clinical assessment within this domain may be considered under the categories of either qualitative or quantitative analysis of movement, depending on the exact purpose of the examination.
*Bolus refers to food and drink material that has been swallowed.
A framework approach to supporting use of US in SLT
The movement towards use of US as an SLT assessment or diagnostic tool necessitates the need for quality assurance and clarity of the SLT role. Recognising this, we propose the use of a framework to support application of US in SLT (Figure 1), comprising the elements of (1) scope of practice, (2) education and competency and (3) governance for each of the uses of US in the SLT profession. The framework uses each element to ensure robust delivery of US across the profession. The same approach has been utilised by other professional groups6,7 and therefore ensures application of US in SLT is consistent with other AHP groups. In the same way, new areas of US activity can be established by developing or revising one or more of the elements, thereby ensuring alignment across the framework.
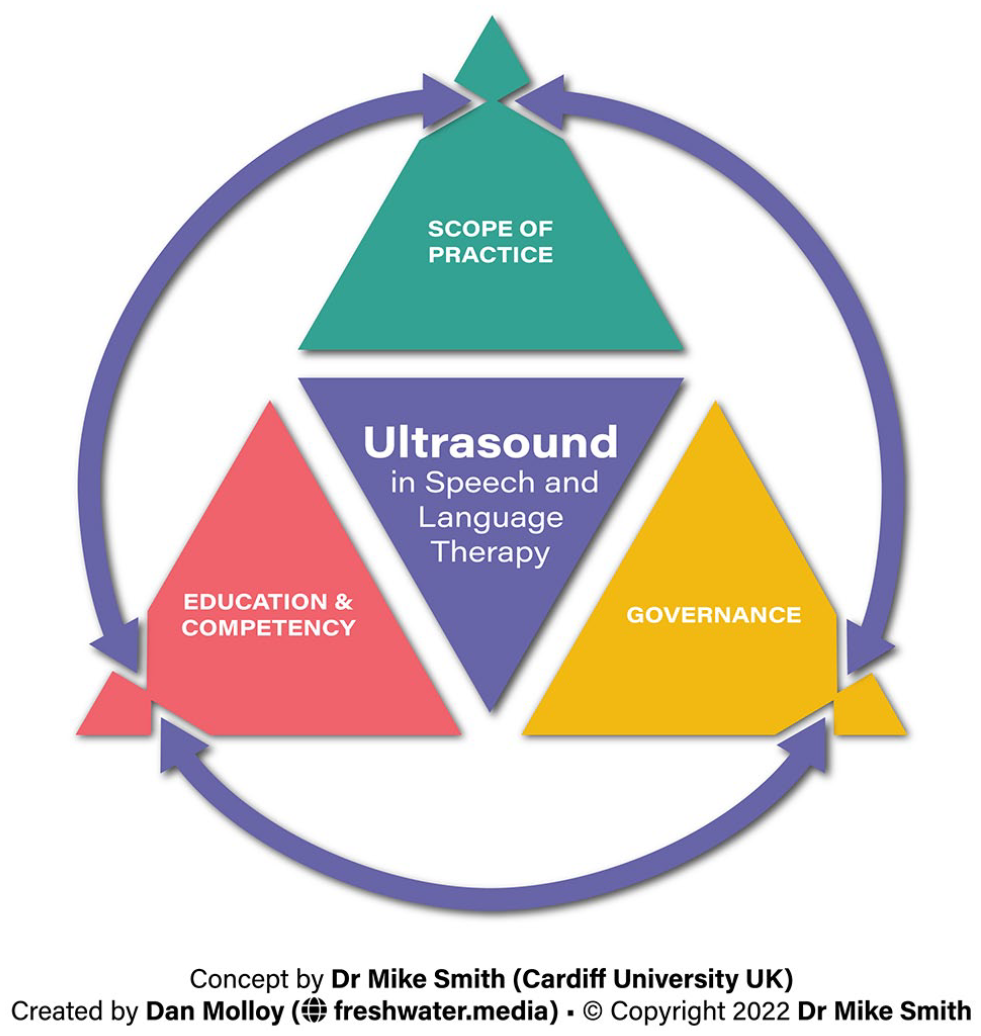
A framework approach to supporting use of US in SLT comprising the elements of (1) scope of practice, (2) education and competency and (3) governance.
Scope of practice: clinical and sonographic
Scope of practice refers to numerous elements, including the tissues to be imaged, the clinical and sonographic differentials, subsequent clinical decision-making and reporting.
As the uses of US in SLT are at different stages of development, scope of practice will depend on the specific area in which the SLT wishes to practice and the multidisciplinary support available to them. The combined (1) clinical usability and (2) clinical utility of US imaging according to the literature are key determinants of the scope of practice in this area.
Table 3 provides an indicative list of imaging that may be performed according to the domains described in Table 2. How the device is used depends on the purpose for which US has been selected by SLT clinicians. Emphasis is currently upon static imaging of structures involved in speech, voice and swallowing as part of staff and patient education as well as qualitative evaluation of structures involved in speech, voice and swallowing for the purpose of biofeedback therapy.
Indicative imaging performed and how this information is used by US SLT clinicians.
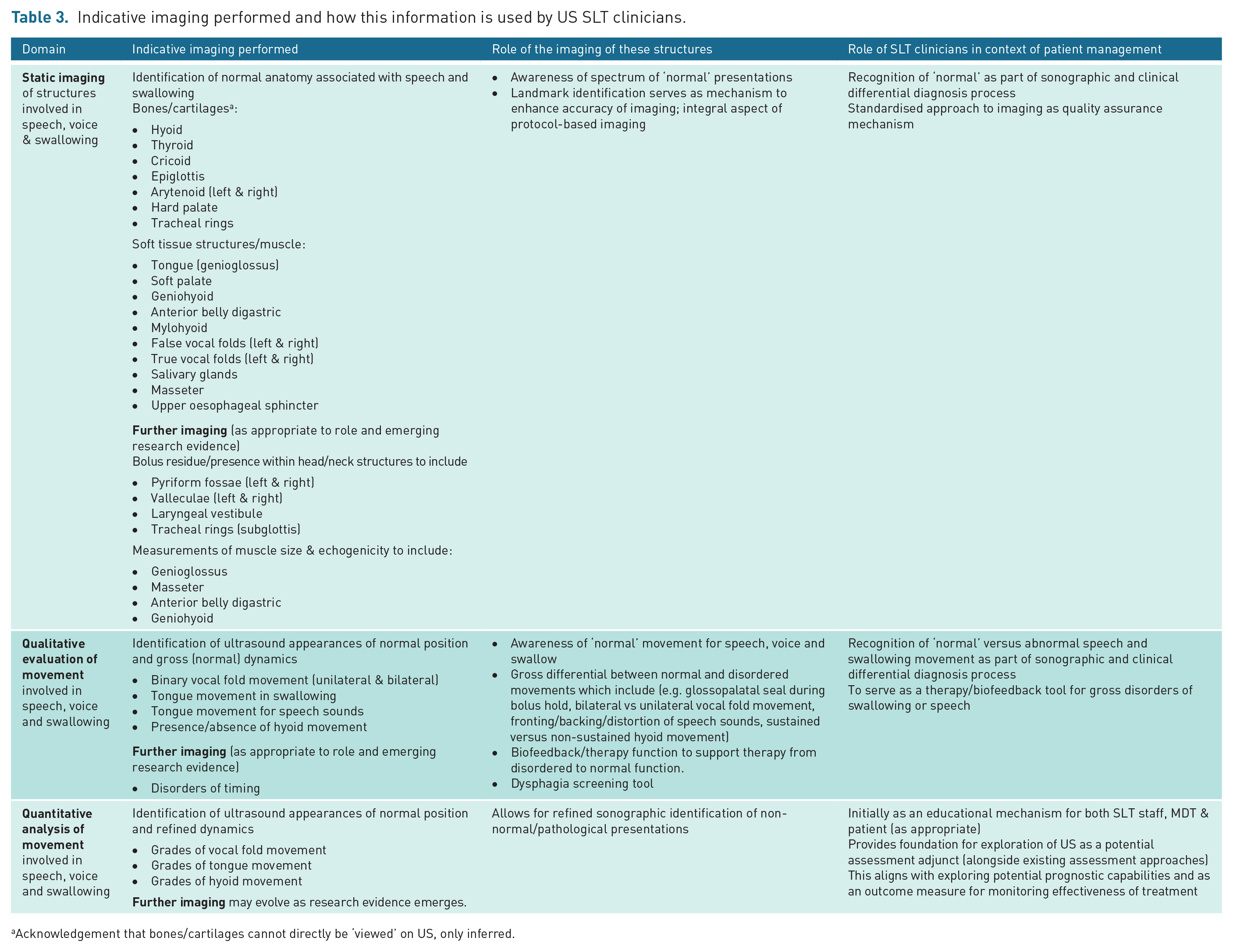
Acknowledgement that bones/cartilages cannot directly be ‘viewed’ on US, only inferred.
US can support the likely differentials generated from the SLT clinical assessment, providing a foundation to move towards the use of US as a ‘rule in’ screening or assessment tool. For example, poor oral containment of a liquid bolus may be hypothesised from the SLT clinical swallowing assessment and further supported (or confirmed) with US when the soft tissue structures of the tongue-base and soft palate are not observed to contact during the oral phase of swallowing. This contrasts with a ‘rule out’ approach (more typically employed by imaging professionals such as radiologists and sonographers) where a range of potential sonographic findings (and subsequent clinical differentials) may be ruled out via the imaging. In the example above, US would/could not be used to ‘rule out’ other swallowing deficits, such as delayed initiation.
Describing US scope of practice for SLT clinicians also determines which imaging practises should not be performed. Examples of imaging not listed in Table 3 and therefore considered outside the SLT scope of practice might include
space occupying lesions in the head and neck;
vascular imaging of the head and neck;
musculoskeletal or maxillofacial issues related to the head and neck, such as temporomandibular junction (TMJ) disorders;
head and neck movements outside that of speech, voice and swallowing, such as blepharospasm and fasciculations.
While the above lie outside of SLT scope of practice, they may be identified as either incidental or concurrent imaging findings. Just as an SLT has a duty of care to escalate patient elements that may be strictly out of remit such as evidence of abuse or risk of self-harm, it is also necessary that they can act upon any unexpected imaging concerns. 15 In this regard, a clear protocol must be in place for the clinician to be able to discuss concerns and for the clinical assessment and/or imaging of the patient to be escalated. A precedent for this has been established in other emerging SLT service models16,17 and could include lines of established communication with those who have more specialist US imaging expertise, access to other imaging modalities and/or surgical or medical opinion. The benefits of SLTs undertaking their US imaging as part of a wider clinical and/or imaging team become apparent in such situations.
The US report should be written and issued by the SLT undertaking the US activity and viewed as an integral part of the process or examination. 15 Findings should be clearly and accurately communicated to the patient and other care pathway members either orally and/or via a written report. The format and nature of the reporting will vary according to the purpose for which US has been used; however, a formal written report is required where US has been applied for assessment or diagnostic purposes.18,19
Education and competency
As per Figure 1, the education and competency elements must align with, and should be reflective of, the scope of practice. In this regard, a description of SLT-specific components is outside the remit of this paper, but would include both formal and informal training, supervision and support from an appropriately trained individual in this area, mentoring and feedback regarding pathology, clinical reasoning and clinical management.
A core consideration for any area of US is that while the scope of the scan may be limited, the standards must be the same as for imaging professionals such as radiographers and sonographers. 15 Certified training courses specifically for SLTs do not currently exist; however, best practice guidance for the acquisition and maintenance of SLT competence can be developed via expert consensus, utilising occupational training standards19 –22 and those developed for other professions as appropriate. 8
A ‘foundation’ US curriculum is initially proposed in Table 4. Levels 1 (foundation), 2 (intermediate) and 3 (advanced) have been used to guide the level of skill required for each application (or scope of US practice) described in Table 2.
Proposed curriculum for Speech and Language Therapists who wish to integrate ultrasound into their clinical practice. Educational elements have been divided into three components: (1) theoretical understanding, (2) technical skill and (3) analysis and interpretation.
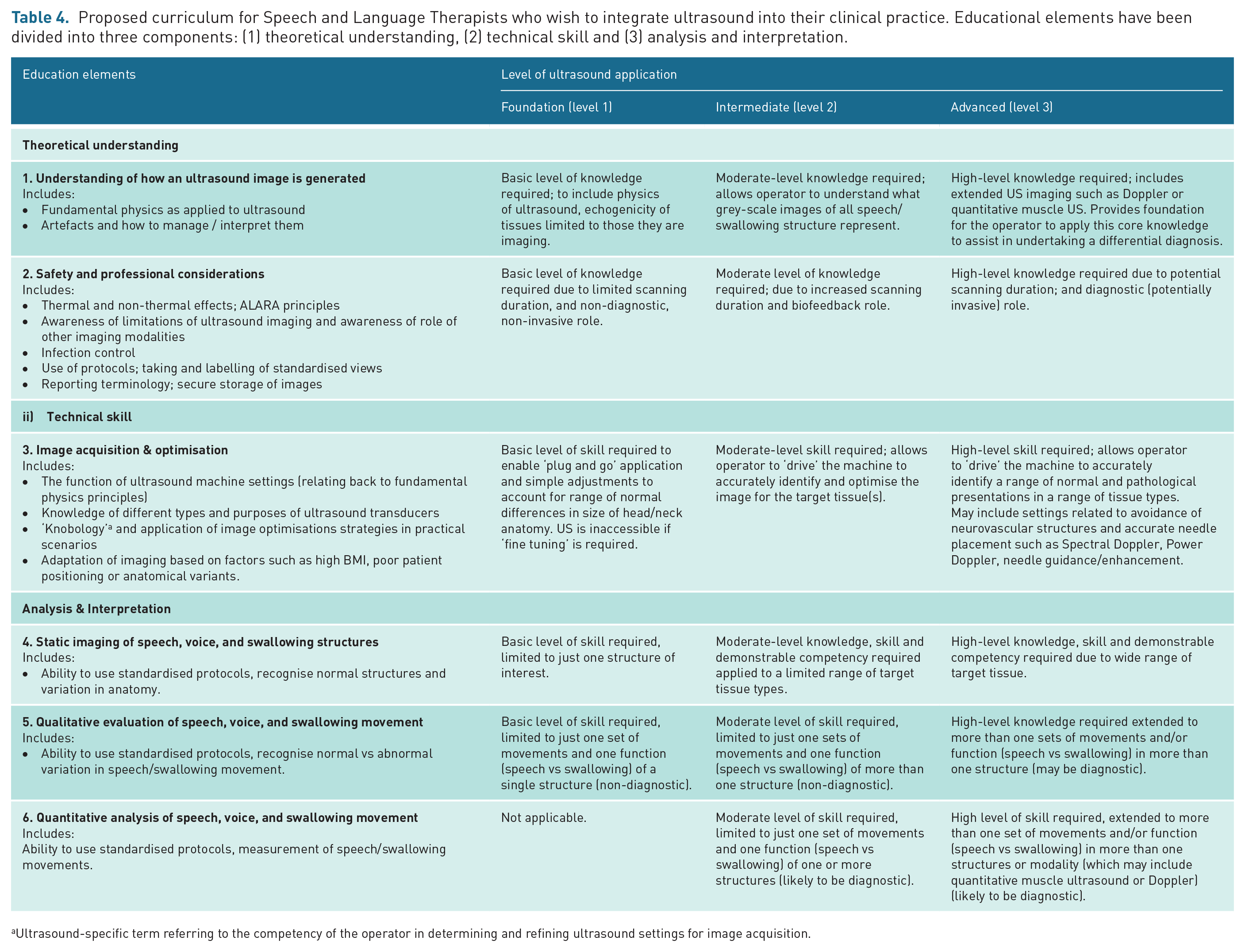
Ultrasound-specific term referring to the competency of the operator in determining and refining ultrasound settings for image acquisition.
Parts of the curriculum (e.g. foundation level) have potential to be integrated at undergraduate/pre-registration level, whereas the intermediate and advanced curriculum might align with the aspirational scope of practice as a diagnostic tool, prognostic indicator or outcome measure for monitoring effectiveness of treatment. Training at this level is likely to be undertaken by more experienced clinicians.
The level of education and training an SLT requires will be dictated predominantly by the requirements of their job role, rather than their banding or years of expertise. For example, injection of botulinum toxin into the salivary glands is likely to require advanced training as well as governance and recognition as an extended scope of practice, compared with the skills and competency required for providing biofeedback for speech sound disorders. The SLT must have the pre-requisite competencies required for their job role prior to integration of US as an education, treatment and/or assessment tool. Training programmes should include the principles and practicalities of ergonomic US practice as well as the safe use and potential hazards of diagnostic ultrasound equipment. 23
Advanced clinical practice agenda
As a progressive area of highly skilled practice, the use of US for assessment and diagnostic purposes would seem to naturally align with the advanced clinical practice agenda. 24 We advocate though that US has the potential to become a routine part of SLT practice and that as such these clinicians do not need to be operating at ‘advanced level’ or above. Nonetheless, the four pillars of advanced practice (clinical practice, leadership and management, education and research) overlap substantially with the expanding role, that is, the use of US by SLTs. 24 As such, we encourage US adopters to explore how use of the imaging modality can further advanced clinical practice and consultant roles.
Insurance and governance
US is a non-regulated imaging modality; thus, no legal restrictions inhibit practice in this area. The use of US is recognised by RCSLT as an ‘extended scope’ of practice. As such, insurance is provided to its members provided the appropriate training and competency elements are in place; however, insurance is not an ‘exact science’ and each claim is usually assessed on its own merits. Activities that fall outside the remit of an SLT (e.g. use of US for muscle biopsy) require alternative cover and accountability agreed with the employer/provider.
Defining the scope of practice confers numerous governance and care pathway benefits. This includes awareness by other care pathway members of what the scan is and is not undertaken for, and support from clinical managers in care pathway design and staffing.
The use of terminology to explicitly clarify the nature of the scan is encouraged. An example of the professional context to the imaging process that could be communicated to colleagues is
Aligning with the scope of clinical and sonographic practice outlined for SLTs performing US (**this publication**), this scan is undertaken for the purposes of assessing/treating XXX as an adjunct to XXX as part of SLT management. The identification of other anatomical or pathological elements is explicitly beyond the scope of practice of the clinician. Therefore, the scan cannot be relied upon to either confirm or exclude any such anatomical or pathological elements.
Quality assurance considerations include data protection, storage of images/videos, testing of ultrasound devices 23 as well as continuous professional development, and access to a second opinion. As US is often undertaken in non-radiology settings, direct access to picture archiving and communication system (PACS) for secure storage and backing up of sonographic images may not be available. This may pose a risk to data security as well as continuity of care and the ability to review image quality. Mechanisms for the secure storage of sonographic images/videos will need to be addressed in line with the information governance policy of the employer. Storage may include bespoke mechanisms to upload to PACS, or the use of other secure image storage capacity as advised by a data compliance officer. There are circumstances where recording of US data is often not required, for example, when used for professional training purposes or biofeedback therapy.
Peer review of the ultrasound images and reports should form part of the quality assurance process, particularly in the emerging areas of assessment and diagnostic practice. A peer-review audit tool for such purposes is offered by The British Medical Ultrasound Society (BMUS). 25
Broader considerations
Expansion of scope of practice
Description of SLT clinical and sonographic scope of practice is not intended to stifle innovation or development of clinical practice or roles. Examples of expanded scope are provided in Table 2 and align with the advanced clinical practice agenda. 24 Such activity may include the potential for SLTs to use US to make tracheal measurements for the purpose of tracheostomy insertion26 –28 as well as confirmation of injection site of botulinum toxin in patients with sialorrhea. 29 Applying the principles outlined in this paper means that where the activity demonstrably sits within the SLT management of a patient, then professional regulation and RCSLT insurance considerations would conceivably have already been addressed. Education and demonstrable competency considerations would need to be satisfied as well as any documentation required by the employer clinical governance committees that demonstrates the change in clinical practice is safe and regularly evaluated.
Another permutation might be where an SLT commences a parallel or advanced clinical activity which involves US imaging in a role that sits outside of what would otherwise be considered part of the SLT management of patients with speech or swallowing disorder. An example might include US-guided muscle biopsy of the muscles involved in speech and/or swallowing to support neurological diagnosis. RCSLT insurance considerations may not apply in such cases; therefore, a potential alternative route would be to arrange indemnity insurance via an employer. Again, education and demonstrable competency considerations would need to be satisfied along with agreement with clinical managers.
Research
Given the sparsity of research evidence to support the application of US in the SLT profession, it is imperative to develop the evidence base relating to if, where and how US can enhance clinical effectiveness and efficiency of SLT assessment and treatment pathways. This includes consideration of optimal education and service delivery models as well as whether the use of imaging may have a negative impact on clinical outcomes or efficiency of resource use. The research priorities in this area are described in a recently published consensus paper. 5
In relation to SLTs performing diagnostic US, some evidence, including a diagnostic test accuracy analysis in relation to the use of US to detect vocal fold palsy, can be drawn from other professional groups such as intensivists, anaesthetists and ear, nose and throat (ENT) medical practitioners.30,31 Nonetheless, the evidence base for the use of diagnostic US by SLTs needs development. The overlap with ENT practitioners, intensivists and head and neck sonographers provides potential opportunity for pooled research and inter-professional collaboration.
In addition to research which seeks to demonstrate the effectiveness of US biofeedback and evaluate assessment protocols, ongoing work seeks to improve the US technology. For speech assessment, systems are now available which synchronise the audio and US signals for play back and analysis. 32 To analyse tongue shape and movement, the surface of the tongue must be tracked accurately. Ongoing work seeks to refine automatic tracking for both speech and swallowing assessment,33 –35 allowing the analyst to extract numerical values to measure movement. Another approach involves machine learning to classify images. An example of this includes recent work to determine the correctness of articulatory gestures in children with speech disorders automatically, 36 an approach which can also be used for outcome measurement. Further work using machine learning to classify various speech, swallow and laryngeal functions is likely in the future.
A direction of travel for other specialities and geographical regions
This paper specifically reflects the situation for SLTs in the United Kingdom, and in this regard, it is noted that the level of autonomy is perhaps greater than that of some professionals in other countries. It is hoped therefore that the generic mechanisms outlined in this paper will provide a potential direction of travel for such professions and regions to advance their use of US imaging in a robust and sustainable manner.
Conclusion
This paper presents a framework approach to support use of US in the SLT profession. As the uses of US in SLT are at different stages of development, scope of practice will depend on the specific area in which the SLT wishes to practice and the multidisciplinary support available to them. The combined (1) clinical usability and (2) clinical utility of US imaging according to the literature are key determinants of the scope of practice in this area. This encompasses a broad range of imaging elements relating to the assessment and therapeutic management of patients with speech, voice and/or swallowing disorders.
Education and competency assessment considerations are explicitly aligned with the clinical and sonographic scope of practice and provide the foundation for robustly satisfying a range of governance requirements. These are further addressed with elements such as data security and continuing professional development.
The framework provides an adaptable model for supporting expansion of US across a range of SLT specialities, including those outside of the current scope of SLT practice.
Footnotes
Acknowledgements
With thanks to the following people who provided a pre-submission review of this manuscript: Gemma Clunie, Helen Newman, Claire Slinger, Lisa Crampin, and Lindsay Campbell; plus representatives of The Royal College of Speech and Language Therapists (RCSLT) Amit Kulkarni (Research & Development Manager) and Tom Griffin (Enquiries Coordinator).
Confirm that you are aware that permission from a previous publisher for reproducing any previously published material will be required should your article be accepted for publication and that you will be responsible for obtaining that permission
Not applicable.
Contributors
All authors made a substantial contribution to the development of this manuscript. The framework concept was provided by MS and is based on his previous work with other allied health professional groups in this area. JA led on the manuscript draft, revision and pre-submission peer review. JC provided all information relating to use of US in speech disorders as well as critical review of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Not applicable.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Dr Joanne Cleland receives funding from the Chief Scientist Office of Scotland (TCS/20/02) and Economic and Social Research Council (ES/V012401/1).
Guarantor
Mike Smith is the guarantor of this article.
Permission from patient(s) or subject(s) obtained in writing for publishing their case report
Not applicable.
Permission obtained in writing from patient or any person whose photo is included for publishing their photographs and images
Not applicable.