
Abstract
The well-being and mental health of principals is being threatened by changing working conditions such as a broader variety of roles and tasks. In this article, we argue that social capital might buffer against declining (mental) health. The purpose of this study was to investigate the potential influence of social capital, including both internal (bonding) and external (bridging and linking) social capital, on principals’ well-being. A longitudinal study was set up across three waves of data. Questionnaires were collected from 2084 Australian principals and 829 Irish principals, across six and two timepoints, respectively. The hypotheses were tested using a longitudinal path model approach using maximum likelihood estimation in lavaan for R. In line with our hypotheses, the results indicated that principals who reported higher levels of either internal or external social capital also reported higher levels of well-being. More specifically, support from colleagues outside the school and supervisor support (external social capital) and collaboration and trust in management (internal social capital) predicted well-being positively across time. The results of this study highlight the importance of having social support from colleagues and supervisors and possibilities for collaboration to maintain well-being as a school principal.
Introduction
School principals’ tasks have become increasingly complex due to decentralization (Matthews et al., 2008) and increasing accountability (Phillips and Sen, 2011). While principals’ main role is to lead learning, they are also expected to be financial and human resource managers, coaches and motivators (Engels et al., 2008). In addition, sometimes principals find that their role is to take full responsibility for implementing decisions made by central administrators that they do not agree with (Burens, 2015). A growing number of principals find it increasingly difficult to deal with the breadth and complexity of their daily tasks (Riley, 2015a, 2015b, 2019). In short, principals’ job demands are steadily increasing while their decision latitude decreases, which creates stress, as the effort required to meet demands cannot always be effectively directed (Riley, 2019; Chaplain, 2001).
Consequently, the well-being of principals is being threatened by changing working conditions (Riley and Langan-Fox, 2013; Riley, 2015a, 2015b). This threat to their well-being is also likely to have wider educational consequences with regard to effective teaching and student learning. It has long been argued that principals are one of the key elements contributing to teacher success and, in turn, to student performance (Leithwood, Louis, and Anderson, 2012; Ni, Yan, and Pounder, 2018). For this reason, the well-being of principals and teachers is getting more attention from policy makers and management (Sahlberg, 2015). However, although scholars have argued that the well-being of principals might play a pivotal role in school functioning, the topic has been little researched (Beausaert, Froehlich, Devos, and Riley, 2016).
There has been an increase in educational research investigating social capital as a way to promote mental health and well-being, and thus retention (Bauer et al., 2019; Leana, 2011). However, while the relation between social capital and well-being is well documented in other industries, and although it has been studied in teachers, it has been less researched within the field of educational leadership. Previous educational research has mostly focused on the role of human capital, the qualifications and competences of teachers and principals and their relation with students’ achievement scores (Adler and Kwon, 2002; Leana, 2011; Spillane et al., 2003). Research that has considered the role of social capital and more specifically its relation with principals’ well-being has been limited (Leana, 2011; McPherson et al., 2014). This is surprising, given principals’ pivotal role in school functioning and the influence they have on setting the conditions under which social capital emerges. Additionally, when studying social capital in the past (e.g., Fiorilli et al., 2019), the focus was mostly on either internal social capital (within the school), also known as bonding social capital, or external social capital, which has two facets: bridging (crossing the school’s boundaries) and linking (crossing hierarchy levels).
Given these gaps, the purpose of this study was to investigate the potential influence of social capital, including both internal (bonding) and external (bridging and linking) social capital, on school principals’ well-being, via a longitudinal study across three waves of data, to provide new insights into the relationship between social capital and well-being. As we undertook the research, we were aware of the literature review by Kim et al. (2008) on social capital and health research. They concluded that the majority of studies were cross-sectional and unable to measure causal relationships, because arguments might be given for the inverse relationship as well (Kim et al., 2008). Therefore, we conducted longitudinal research to address causality. We began with careful explication of both well-being and social capital, as these are often not clear in the literature. The following sections present and define the two key concepts that framed the research: well-being and social capital.
Theoretical framework
Well-being
Work-related well-being has been defined as “that part of an employee’s overall well-being that they perceive to be determined primarily by work and can be influenced by workplace interventions” (Juniper et al., 2011: 347). In addition, general well-being has been defined in several ways. Historically, the World Health Organization (1946) used the following definition: “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity” (p. 1). They expanded this in 2015 to “a state…in which every individual realises his or her own potential, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to her or his community.” Other scholars have defined well-being as “the balance point between an individual’s psychological, social and physical resource pool and the psychological, social and physical challenges faced” (Dodge et al., 2012: 230).
Well-being has often been defined by referring to between two and seven dimensions of well-being (Dodge et al., 2012), such as mental and physical well-being (Corbin and Pangrazi, 2001), or physical, mental and social well-being (World Health Organization, 1946). Physical well-being is the efficient functioning of the organs, while mental well-being is the ability to cope successfully with the normal problems and stresses of life, and social well-being relates to people’s roles within society as a whole. However, these dimensions are interrelated. For example, physical discomfort at work might lead to a decrease in mental well-being and induce feelings of depression and anxiety, and thereby impede social interaction. Although we were especially interested in mental well-being, we also included indicators of general well-being, given the interrelatedness of the various well-being dimensions.
Social capital
There are various conceptualizations of the phenomenon of social capital, as it is a complex concept, and the different conceptualizations complement rather than compete with each other (Villalonga-Olives and Kawachi, 2015). In addition, although social capital is a sociological term, it has been applied and translated within various disciplines, such as psychology and educational sciences, which might not always have helped to clarify its meaning.
The term social capital is originally attributed to Bourdieu (1986). He defined social capital in terms of the size of the network and the economic, cultural and symbolic capital the network possesses. More concretely, he defined social capital as “the aggregate of the actual or potential resources which are linked to possession of a durable network of more or less institutionalized relationships of mutual acquaintance and recognition” (p. 248). Shortly thereafter, Coleman (1988) referred to the level of trust, information channels, and norms and sanctions when defining social capital (Dika and Singh, 2002). Social capital for Coleman (1988) “comes about through changes in relationships [networks] among people that facilitate actions…social capital exists in the relations among people” (p. 100). Social capital is multi-faceted, as it encompasses aspects of social structures, enables action within those structures and allows achievements that may not be possible without it (Coleman, 1988,). In sum, both of these sociologists focused on the sum of benefits to individuals or families because of their ties with others (Dika and Singh, 2002). For the purposes of this paper, social capital is broadly defined as “the actual and potential resources embedded in relationships among actors” (Leana and Pil, 2006: 353). The embeddedness referred to here is not just about existing relationships or belonging to networks (Dıaz-Gibson et al., 2017). It also conveys that these relationships/networks are rooted in trust and expectations, where norms are generated and imposed (Coleman, 1988). Day (2000: 585) stated: “the emphasis with social capital is on building networked relationships among individuals that enhance cooperation and resource exchange in creating organizational value.” In that sense, just like Bourdieu and Coleman, we define social capital in terms of norms and access to institutional resources (Dika and Singh, 2002).
Different forms of social capital have been distinguished. In general, a distinction can be made between internal (bonding) and external (linking and bridging) social capital. Scholars also refer to bonding, linking and bridging by making a distinction between horizontal (bonding and bridging) and vertical (linking) dimensions of relationships and networks.
Horizontal social capital is created between individuals or groups at the same hierarchical level (e.g., colleagues), where bonding social capital occurs. The bonding that occurs among and between people through their internal social relationships/networks produces this subtype of social capital. Bonding emerges in structures such as familial relationships or interactions in social clubs. It reflects allegiances and shared interests, norms and values. Within the school context, this form of capital helps to establish and maintain workplace collegiality. Next, bridging social capital, another form of horizontal social capital, promotes allegiance not only to a specific school, but also to the sector with which it is connected, such as public, religious, private or independent education. For example, bridging stakeholders are professional organizations and unions for principals. Bridging social capital includes face-to-face involvement, trust, status and credibility based on expertise (Adler and Kwon, 2002; Kawachi et al., 2008; Minckler, 2014; Szreter and Woolcock, 2004).
Vertical social capital considers the relations between individuals or groups where there are differences in formal power and/or authority, for example, between a teacher and principal (Grubb and Flessa, 2006; Szreter, and Woolcock, 2004; Woodhouse, 2006). Linking capital occurs in those relations. Examples of linking stakeholders are departments of education, and other agencies such as welfare, child protection and philanthropic organizations. This type of social capital provides access to institutional power, information, wealth and social status.
More recently, and building further on Bourdieu and Coleman, Nahapiet and Ghoshal (1998) distinguished three dimensions of (internal) social capital. The first dimension, structural, refers to the connections that exist between colleagues: how often and with whom information is shared. The second dimension, relational, signifies the personal relationships that people develop with each other over time. One of the key attributes of the relational dimension is the level of trust, enabling an environment of justice and collaboration. Third, internal social capital has a cognitive dimension, representing the extent to which colleagues are able to develop a shared vision for the school/organization.
Social capital and well-being
Many studies in various settings have investigated the relationship between social capital and well-being. First, studies based in sociology have studied the relation between the social capital of citizens and their well-being. In general, research investigations into the relation between citizens’ social capital and health make the distinction between structural and cognitive dimensions of social capital (Gilbert et al., 2013). In that case, the structural dimension refers to taking part in social networks and associations and other forms of civic engagement. The cognitive dimension encompasses the perception of trust and reciprocity, through norms, values and attitudes (Engström et al., 2008). Yip and colleagues (2007), for example, studied the relation between social capital, general and psychological health and subjective well-being in China. Structural social capital was measured by organizational membership and cognitive social capital was measured by studying trust, reciprocity and mutual help. Trust was found to be positively related to all outcome measures. Similarly, the relation between (contextual) social capital and subjective health was studied in Sweden (Engström et al., 2008). Engström et al. (2008) studied four dimensions of social capital: horizontal (civic trust and participation), vertical (political trust and participation), cognitive (civic and political trust) and structural (civic and political participation). Geographical regions in Sweden were compared, and it was found that areas scoring lower on contextual social capital also reported a poorer level of health, even when controlling for background variables such as age, gender and socio-economic status. Other scholars have studied the relationship between social capital (stronger social ties and trust) and death or suicide rates (Helliwel, 2006; Kawachi et al., 1997), finding that, in general, social capital has a positive relationship with public health.
Previous research explained the positive influence of social capital on health by referring to the fact that the presence of social capital can foster self-esteem, provides social support, enlarges access to resources and might buffer stress (Ziersch et al., 2005). For example, in a longitudinal study, the internal social capital, more specifically the perception of justice, of 1519 Dutch employees had an inverse effect on symptoms of depression (Ybema and Van den Bos, 2010). A review study including 14 studies focusing on the relation between the cognitive dimension of social capital (i.e., confidence) and mental well-being also found a significant relationship (De Silva et al., 2005). Similarly, in an investigation of external social capital, Iwase and colleagues (2012) questioned 2260 inhabitants of a Japanese city with around 700,000 inhabitants and found that bridging social capital (i.e., participation in groups involving people from a diversity of backgrounds) negatively influenced bad health; however, bonding social capital was not significantly related to health. They have concluded that there is a growing need for longitudinal research studying the relationship between social capital and well-being, while keeping in mind the various dimensions of social capital. In line with Gilbert et al. (2013), we would suggest that what is needed is a much clearer articulation of the types of social capital that findings are reporting on.
Second, previous research has studied the social capital of employees in various sectors and its relation with their well-being. Driller and colleagues (2010) from the field of health, for example, investigated the relationship between social capital and emotional exhaustion in clinicians in four German hospitals. Lower levels of perceived social capital were found to be significantly related to clinicians’ emotional exhaustion. A study by Sapp et al. (2010) of 26 manufacturing employees found that social capital was a protective factor with regard to job stress.
Third, within the field of education, scholars have studied the relation between teachers’ social capital and their well-being. Veronese and colleagues (2018), for example, studied three cohorts of Palestinian teachers in conflict-ridden areas and found positive relations between social capital, operationalized as basic and social services offered, and personal well-being. Edinger and Edinger (2018) studied the social capital of 122 elementary school teachers in the United States. They found that social capital, that is, teachers’ centrality of position in their school’s trust network and the density of a teacher’s academic advice ego-network, had a significant positive relation with their job satisfaction.
Fourth, a limited number of studies have looked into principals’ social capital and well-being. Leana and Pil’s (2006) work suggested that principals whose embedded relationships and networks within and across schools are weak might be at increased risk of ill health when facing intense job demands. If principals have a relational basis to their leadership, it is more likely that the bonding form of social capital will be present. When this form of leadership extends to the broader community of stakeholders, it is also likely that bridging (crossing the organization’s borders) and linking (crossing hierarchy levels) social capital will emerge. These forms of social capital aid leaders facing increasing job demands (Bauer et al., 2019; Grubb and Flessa, 2006; Szreter and Woolcock, 2004; Woodhouse, 2006). In addition, a large body of educational research has been looking into subcomponents of social capital and its relation with principals’ well-being, or related variables. For example, the role of social support and isolation was studied for principals’ burnout. As expected, it was found that a lack of social support led to isolation and thus more emotional and physical burnout (Stephenson and Bauer, 2010). Similarly, Price (2012) found that principals’ relationships with their teachers affect principals’ job satisfaction and commitment.
Studies such as those discussed above have indicated the significance of social capital for well-being, and therefore that this linkage is worth investigating in relation to school principals, particularly as this is a relatively new area of educational research. Consequently, it is hypothesized that if principals can rely on colleagues in the school (internal social capital) and a broader community of stakeholders (external social capital), the increased support will help them face the increasing demands that tax their well-being. More concretely:
Hypothesis: Principals who self-report higher levels of both internal and external social capital will score higher on well-being across time (even after controlling for autoregressive effects).
Method
Participants
The present study is drawn from a larger project investigating the health and well-being of Australian and Irish school principals (including deputy and assistant principals). 1 Responses were both anonymous and voluntary. Participants voluntarily provided contact details to the researchers to be used for subsequent invitations. The invitations and reminder e-mails were sent out two weeks apart while the survey was open. All principals who completed the survey in Year 1 were invited to complete an update survey in the subsequent years.
The longitudinal study included 2084 Australian principals and 829 Irish principals (complete sets only). For the Australian cohort, women represented 56% of the sample. In 2012, the participants were on average 56 years old (SD = 7 years). On average, they had been in a leadership position (deputy, assistant or principal) for 12 years (SD = 8 years). They were mainly working in government schools (72%), but were also in Catholic (14%) and independent schools (14%). Their schools were fairly evenly distributed over the 10 deciles of the national socio-economic index, that is, the Socio-Economic Indexes for Areas (SEIFA), which ranks areas in Australia according to their relative socio-economic advantage and disadvantage. Most of the schools were situated in a suburban location (39.5%), while 26% were in rural locations, 18.5% in urban locations, 10% in large towns and 4.5% in remote locations. The majority (61%) were principals in primary education, 13% were responsible for both primary and secondary education, while the remainder were principals in secondary education. These demographic measures match with the total population of school principals in Australia, indicating that the sample is representative of the whole country (Riley, 2014). In the analyses, we used the data from 2012 to 2017 (six time points, also referred to as t2 to t7).
In the Irish cohort, women represented 69% of the sample. In 2014, on average, principals were 48 years old (SD = 7.79 years) and had been in a leadership position for 12 years (SD = 7.40 years). Most of the schools were situated in villages, rural areas or small towns (54%). Unlike Australia, 46% were located in rural locations. Most principals (69%) were working in a primary school, while 28.5% were working in a school for secondary (2nd level) education. The rest were working in a “special school”. In the analyses, we used the data from 2014 to 2015 (two time points).
Instruments
Social capital
This study measures facets of social capital by making a distinction between internal (bonding) and external (linking and bridging) social capital. To measure internal social capital (bonding), we focused on the relational dimension by making use of three subscales of the Copenhagen Psychosocial Questionnaire-II (COPSOQ-II; Pejtersen et al., 2010) – trust in management, justice and collaboration – since those three dimensions are core to most definitions of social capital. The psychometric qualities of the COPSOQ-II have been demonstrated among a large sample of participants from numerous occupations and countries (Albertsen et al., 2010; Bjorner and Pejtersen, 2010; Burr et al., 2010; Dupret et al., 2012; Nuebling and Hasselhorn 2010; Nuübling et al., 2006; Pejtersen et al., 2010; Thorsen and Bjorner, 2010) and with the current sample of principals (Dicke, Marsh, Riley, Parker, Guo, and Horwood, 2018).
The trust scale consists of four items (e.g., “Does the management trust the employees to do their work well?”), measured on a 5-point Likert scale going from 1 (to a very small extent) to 5 (to a very large extent). The justice scale contains four items (“Are employees appreciated when they have done a good job?”) and is measured on a 5-point Likert scale going from 1 (to a very small extent) to 5 (to a very large extent). Finally, the collaboration scale consists of three items (e.g., “Is there good co-operation between the colleagues at work?”) and is measured on a 5-point Likert scale going from 1 (never/hardly ever) to 5 (always).
External social capital, including both linking and bridging social capital, was measured by using the COPSOQ-II subscales for supervisor support (linking) and support from colleagues outside the school (bridging). The first subscale, supervisor support, consisted of three items (e.g., “How often do you get help and support from your nearest superior?”), which were measured on a 5-point Likert scale, going from 1 (never/hardly ever) to 5 (always). The second subscale (support from colleagues outside the school) was measured by three items (e.g., “How often do you get help and support from colleagues outside your school?”), also responded to on a 5-point Likert scale going from 1 (never/hardly ever) to 5 (always). The Cronbach’s alphas for trust, justice, collaboration, supervisor support and support from colleagues outside the school were .76, .84, .89, .88, and .85, respectively, for the Australian principals in 2012, and .72, .76, .82, .86, and .86 for the Irish principals in 2014.
Well-being
We measured well-being in two different ways. First, we looked at general health, measured with one item (“In general, would you say your health is excellent, very good, good, fair or poor?”) using a 5-point Likert scale (1 = poor to 5 = excellent). This is the person’s assessment of her or his own general health. This one global item, which has been used in numerous questionnaires, has been shown to predict many different endpoints, including mortality, cardiovascular diseases, hospitalizations, use of medicine, absence and early retirement (Idler and Benyamini, 1997). The second measure used a shortened version of the mental health subscale from the Assessment of Quality of Life 8 Dimensions questionnaire (AQoL-8D; Richardson et al., 2014). The mental health subscale normally consists of eight items (e.g., “How often do you feel depressed?”), measured on a 6-point Likert scale (1 = all the time to 6 = never), but we shortened the questionnaire to include only six items, because of the low loadings of two of the items on the mental health factor. The Cronbach’s alpha was .83 for mental well-being for the Australian principals in 2012 and .83 for the Irish principals in 2014. Each scale was recalibrated to have a value between 0 and 100.
Data analysis
We tested the hypotheses for the Australian dataset using a covariance-based panel path model approach using Maximum Likelihood estimation in lavaan for R (Rosseel, 2012). The Australian data contained six measurement points and served as the main dataset for testing the hypothesized model, using a cross-lagged panel design including autoregressive relationships (i.e., effects across time within a concept, for example, a decrease or increase in one variable). The Irish data contained only two measurement points and was used just to confirm or disconfirm the basic relationship between internal and external social capital and mental and general health in a lagged study design. The schema for both models is depicted in Figure 1.
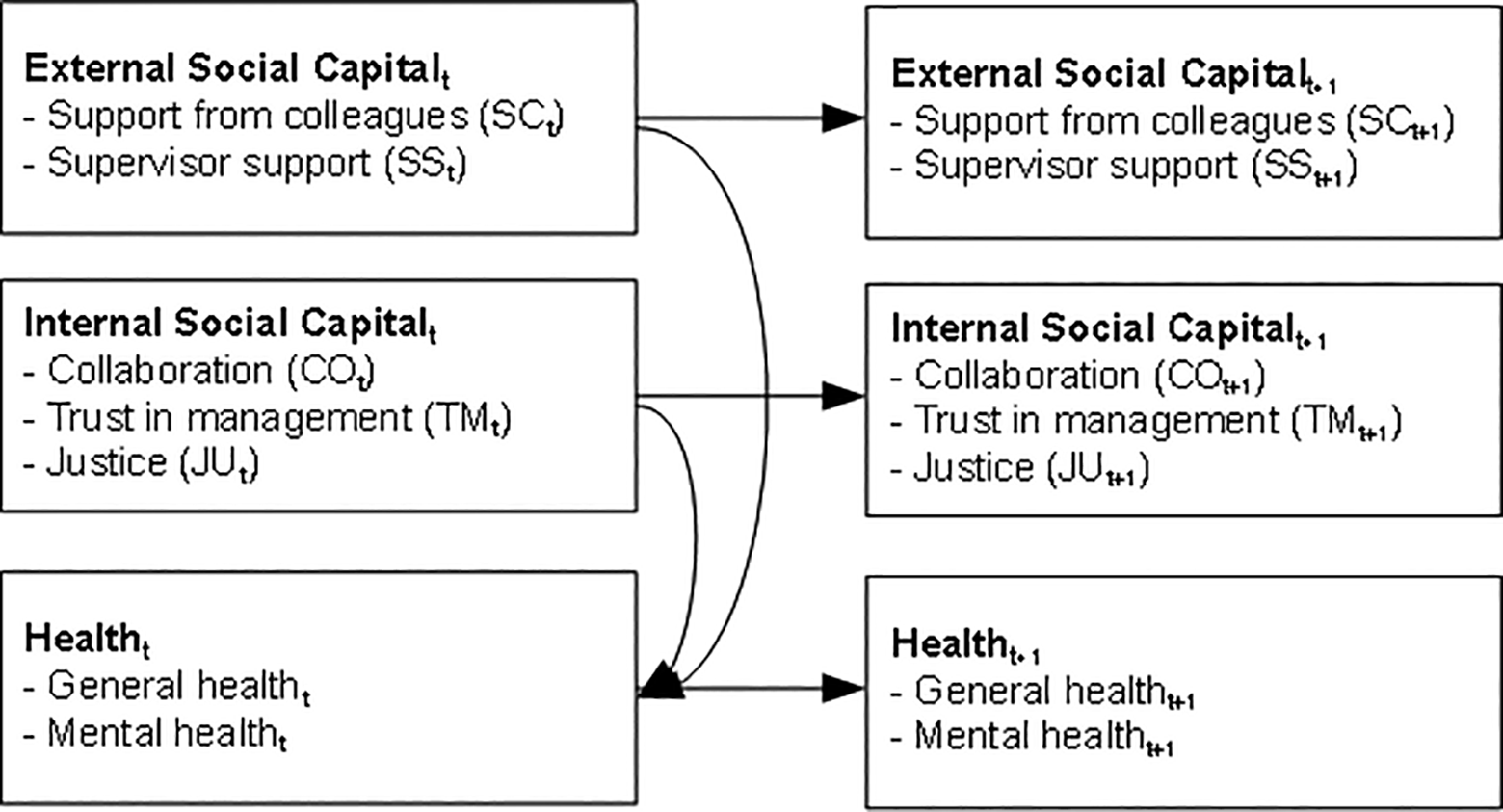
Schema of the path models.
We assessed model fit using the root mean square error of approximation (RMSEA, acceptable if ≤ .08; Browne and Cudeck, 1993) and the comparative fit index (CFI, acceptable if ≥ .90; Byrne, 2010; Hu and Bentler, 1999). Missing data were handled using full information maximum likelihood estimation (Enders, 2010), which is a common method in structural equation modelling (Dong and Peng, 2013).
Results
Preliminary analysis
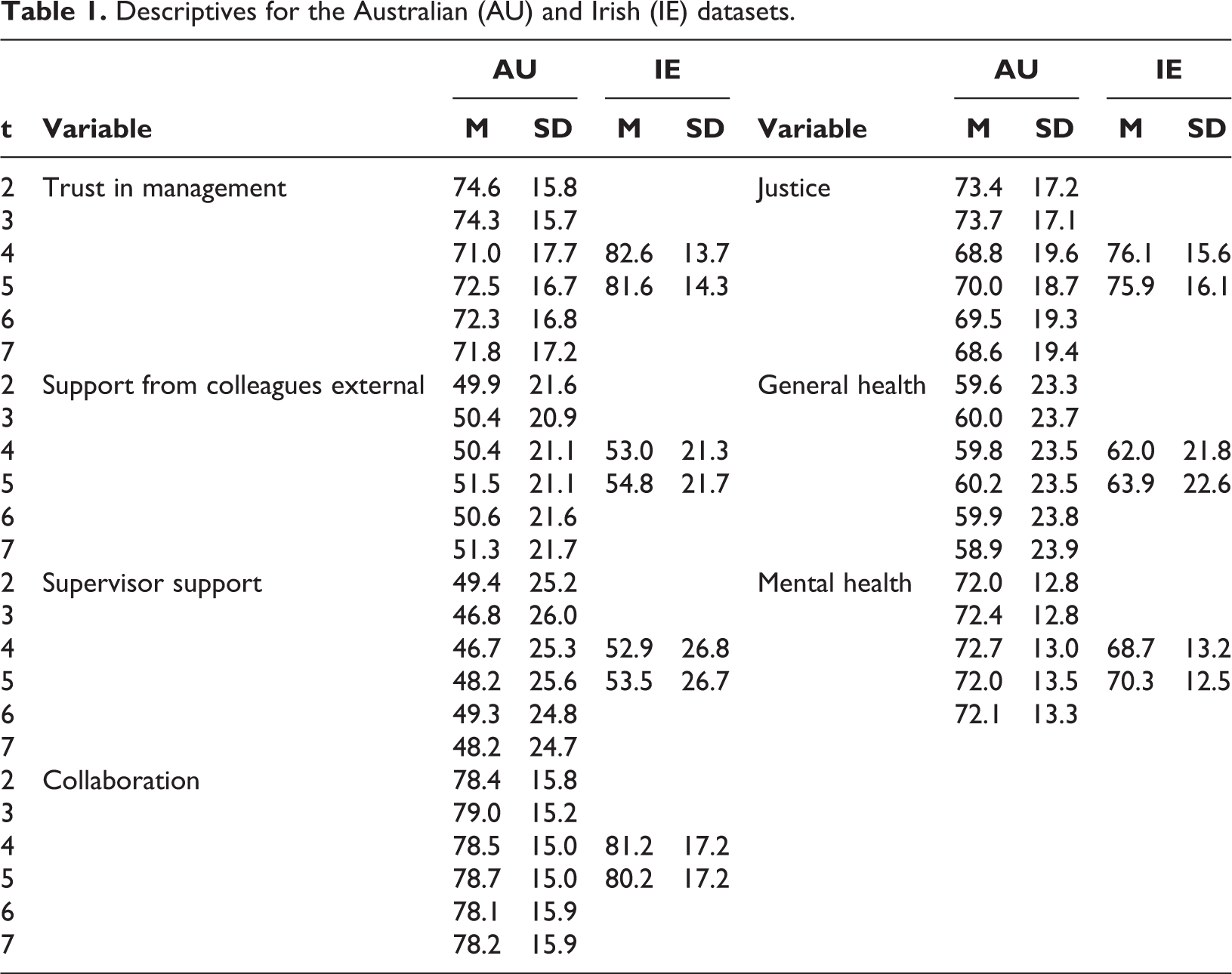
Table 1 shows the means and standard deviations of the focal variables (external social capital: support from colleagues outside the organization and supervisor support; internal social capital: collaboration with colleagues inside the organization, trust in management and justice; mental and general health). These means and standard deviations reached similar levels in both countries and also remained stable over the time periods measured. Regarding the independent variables in the model, higher values were reported for external social capital than for internal social capital. Specifically, support from colleagues outside the organization and supervisor support had higher mean scores in both countries and across measurement points (M ≈ 3.00) than collaboration, trust in management and justice (M ≈ 2.00).
Descriptives for the Australian (AU) and Irish (IE) datasets.
Hypothesis testing
We operationalized external social capital as support from colleagues outside the school (SC) and supervisor support (SS), and internal social capital, as collaboration with colleagues internal to the organization (CO), trust in management (TM), and justice (JU). We operationalized well-being as mental health (MH) and general health (GH).
The model fit of the Australian data was acceptable in terms of the RMSEA (.04) but slightly below the threshold for the CFI (CFI = .88). Table 2 shows the path coefficients of the tested relationships. Significant autoregressive relationships existed for all variables in the research model (ßs ranging from .40 to .69, p < .01). Around 50% of the variance in the dependent variables was explained by autoregressions, for both mental and general health. This figure dropped to 5% and 1%, respectively, when the autoregressive effects were not considered.
Path estimates for both Australian and Irish data.
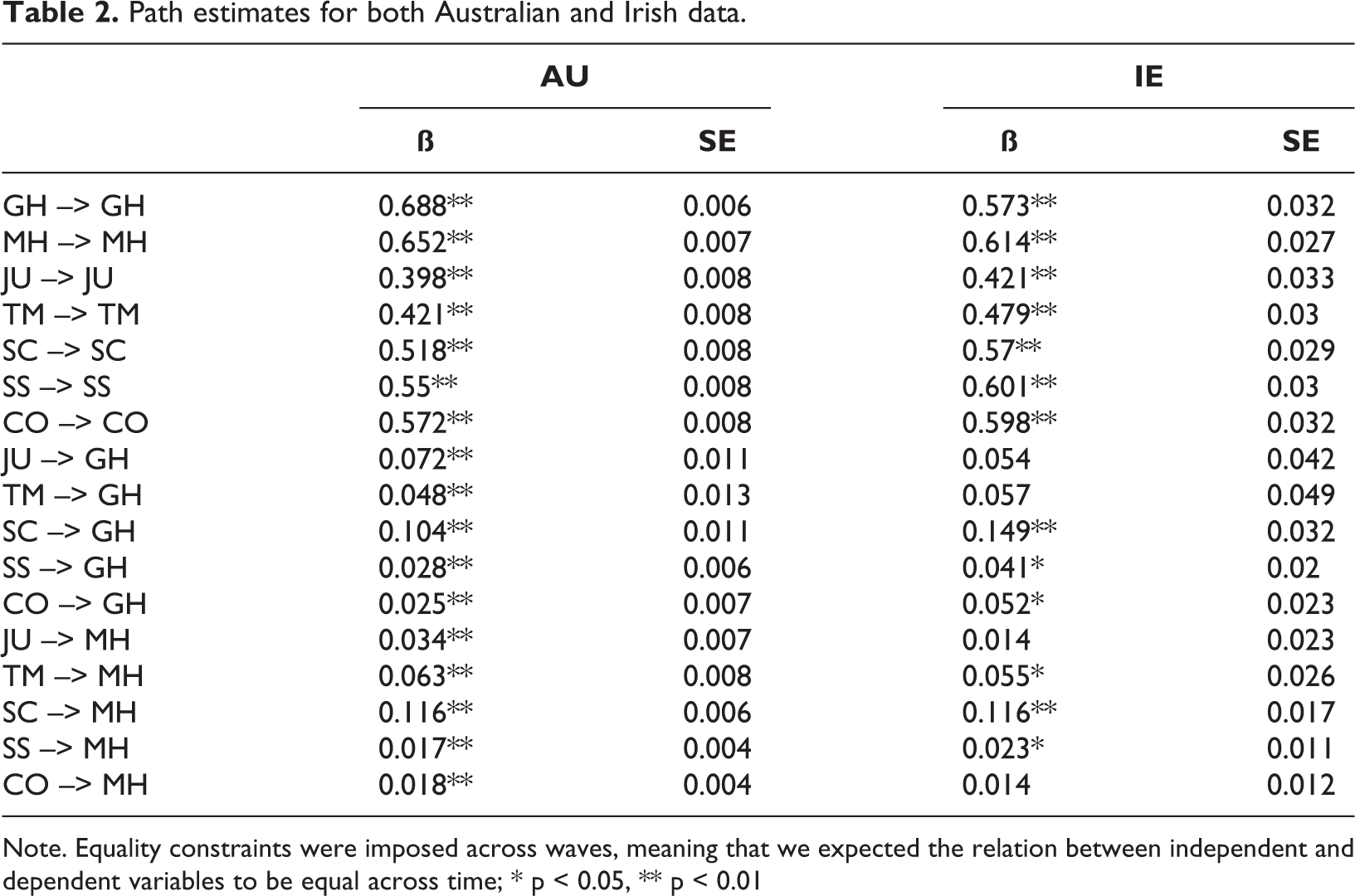
Note. Equality constraints were imposed across waves, meaning that we expected the relation between independent and dependent variables to be equal across time; * p < 0.05, ** p < 0.01
Furthermore, we found statistically significant positive relationships of both internal and external social capital with mental health (JU --> MH, ß = 0.03, p < 0.01; TM --> MH, ß = 0.06, p < 0.01; SC --> MH, ß = 0.12, p < 0.01; SS --> MH, ß = 0.02, p < 0.01; CO --> MH, ß = 0.02, p < 0.01) and general health (JU --> GH, ß = 0.07, p < 0.01; TM --> GH, ß = 0.05, p < 0.01; SC --> GH, ß = 0.10, p < 0.01; SS --> GH, ß = 0.03, p < 0.01; CO --> GH, ß = 0.03, p < 0.05). This provides strong support of the tested hypothesis.
The model fit for the Irish data was also satisfactory: RMSEA = 0.06, CFI = .94. Again, significant autoregressive relationships existed for all variables in the research model (ßs ranging from .42 to .61, p < .01). The relationships found in the Irish dataset mirrored our observations in the Australian data in that all of the relationships were positive. The explained variance was slightly smaller than in the Australian dataset when considering autoregressive effects, with 48% of the variance explained for mental and 35% for general health, but higher without the autoregressive effects (5% of the variance explained for mental health, 4% for general health). The path estimates were also more nuanced in terms of statistical significance, as the main drivers for mental (TM --> MH, ß = 0.06, p < 0.05; SC --> MH, ß = 0.12, p < 0.01; SS --> MH, ß = 0.02, p < 0.05) and general health (SC --> GH, ß = 0.15, p < 0.01; SS --> GH, ß = 0.04, p < 0.05; CO --> GH, ß = 0.05, p < 0.05) were more clearly distinguished.
Discussion
Both theory and practice suggest that principals’ social capital is important for developing and maintaining their well-being (Hargreaves and Fullan, 2013; Leana, 2011). If principals can rely on colleagues in the school (internal social capital) and a broader community of stakeholders (external social capital), it will be easier to find support and face the increasing demands that negatively impact their well-being (Grubb and Flessa, 2006). However, there is a gap in the research concerning the relation between principals’ social capital, including both internal and external social capital, and their well-being. Although the relation between internal and external social capital and well-being has been studied before, it has not yet been studied among school principals. In that sense, this study took an exploratory approach along with a more conservative, confirmatory approach when it comes to studying the effect of social capital on the well-being of school principals specifically, which was made possible by the use of two parallel datasets. The hypothesis driving this study was that principals who have greater (internal and external) social capital should score higher on well-being across time. The hypothesis was studied via a longitudinal study across six (Australia) and two (Ireland) data collection timepoints.
A panel path model approach using maximum likelihood estimation was applied. The results indicated that principals who reported higher levels of either internal or external social capital also reported higher levels of mental well-being. Similarly, and again in line with what was expected, a positive relation was found between social capital and general health across time. In other words, the higher the level of social capital, the higher the perceived general health of principals. More specifically, support from colleagues outside the school and supervisor support (external social capital) and collaboration and trust in management (internal social capital) were significant positive predictors of general health across time.
The findings suggest that collegiality and collaboration do lessen the symptoms of decline in well-being. This is a positive, if unsurprising, finding and suggests that it is very important for principals to have internal and external collegial networks that promote social capital. This finding is interesting because of the long work hours that principals report. The mean working hours for the Australian participants were 58.8 hours per week, with the Irish reporting ∼50 hours per week. The very long hours at work would predict a decline in (mental) health (Dinh et al., 2017), but this appears to be counteracted by high levels of social capital for school principals. What is even more impressive with this finding is that Dinh et al. found that “Women’s mental health scores began to track lower than men’s once they worked more than 35 hours, a slight drop in men’s scores occurred after they worked more than 50 hours, yielding preliminary evidence for gendered and non-linear workhour-health relationships” (p. 45). With a high percentage of female school leaders (69% of the Irish principals, and 56% of the Australian principals), the higher mental health scores in spite of long average working hours suggests that social capital is a very valuable resource for them. Our findings are in line with similar previous research that studied the relation between people’s social capital and health or (mental) well-being (e.g., Edinger and Edinger, 2018; Engström et al., 2008; Veronese et al., 2018). However, in our study, we see similar patterns of results across outcome variables, time and regional contexts, which gives us confidence in the results found.
Limitations and suggestions for future research
This study’s limitations suggest different approaches for future research. First, future research could further sort out the concept of social capital. This study made a distinction between external and internal social capital. Concerning the latter, we focused especially on the relational dimension, by looking at trust, collaboration and justice. The two other dimensions of internal social capital, namely structural (i.e., connections between colleagues) and cognitive (i.e., shared vision among colleagues), could be studied in future research. This could be done through social network analysis, which could provide more detailed insights into how and when connections are formed and used. External social capital could also be further explored, for example, by including neighbourhood attachment as a way of identifying and measuring this form of social capital. The fact that the concept of social capital originated from sociology, but has been applied in various disciplines, such as psychology and the educational sciences, might have led to confusion about the meaning and dimensions of social capital. Future research could take a multi-disciplinary perspective and clarify how the concept of social capital has been defined and measured in various disciplines.
Second and related to the previous point, future studies could further investigate the dynamics of social capital by applying qualitative research methods. What interplay is taking place between social support, trust and collaboration? What determines how principals feel socially supported and, in turn, show higher levels of well-being and health? Are there additional variables that need to be taken into account? That said, we did use the richness of our dataset to explore potential avenues for future research in post-hoc analyses. Specifically, we tested for regional differences (rural areas vs. urban areas) and the perception of social community (Sample item: “Is there a good atmosphere between you and your colleagues?”), based on previous research (Beausaert et al., 2016). However, the inclusion of these variables did not change the overall pattern of effects.
Third, the study took into account data collected in Australia and Ireland. However, while six waves were collected in Australia, only two waves were collected in Ireland. The literature has argued that (mental) well-being is something that evolves over time (e.g., stress leading to burnout; Beausaert et al., 2016). Therefore, longitudinal research that includes more than two waves is of crucial importance. This would also allow for an in-depth investigation regarding the specific trajectory of ill-being: how and when do mental health and physical health affect general health? While other research has suggested that, for instance, mental health issues will affect general health at some later point in time, we still do not know much about the time lag that we should take into account in longitudinal research. Future research could also collect data in more diverse countries in order to study national differences. When studying national differences, person-related background characteristics could be taken into account, such as gender, age, socio-economic status, kind of employment or level of education. Such effects were tested in preliminary analyses in this study. We did not identify statistically significant effects of these background variables. These variables were not included in the final model due to a substantial amount of missing data for these variables and differing measurement approaches between the countries.
Fourth, the way we measured general health, by asking people to assess their own general health on a 5-point Likert scale going from poor to excellent, is often criticized. Although this way of measuring general health is in line with how previous research was set up and although we measured mental health alongside general health, showing similar patterns, other ways of measuring general health could be considered. For example, economists prefer more objective data or observed behaviour, if possible, for measuring health. Other scholars have argued that a more objective measure is needed because of the confounding role that personality might play. Optimists might tend to indicate that they are more satisfied with their general health than pessimists. Additionally, the subjective scores for well-being might differ according to regions or national culture. However, it has been found that cross-country differences in subjective health predict suicide behaviour (e.g., Helliwel, 2006; Kawachi et al., 1997). In other words, nations reporting poorer average health using a subjective measure also have higher suicide rates. In that sense, subjective health measures are informative (Helliwel, 2006).
Practical implications
The multiple and various demands on principals, in combination with the dominating image that they have to carry all the burdens of managing a school, make theirs an impossible, often isolated, job (Grubb and Flessa, 2006). Therefore, having some social support within and outside the school and the possibility to collaborate might be welcome. The results of this study highlight the importance of having social support from colleagues and supervisors and possibilities for collaboration to maintain well-being as a school principal. This could be done by investing in communities or networks of principals, either face-to-face or online, in which support can more easily be found. Another way of addressing the increased demands could be by restructuring principals’ tasks. Pounder and Merrill (2001) argued that unbundling or repackaging the job responsibilities with an administrative team that shares the leadership of the school could be a solution. In light of these suggestions, they talked about co-principalship in which leadership is shared between two people, a possibility that could both reduce work hours and increase social capital. While this might appear to be an expensive solution, it may turn out to be the only real way to provide principals with the support and collaboration needed for maintaining their well-being.
Conclusion
Recent changes in working conditions, such as a broader variety of tasks, have put the well-being of school principals under pressure. This study highlighted the importance of having social support from colleagues and supervisors and possibilities for collaboration to maintain school principals’ well-being. To our knowledge, this was the first study that investigated the potential influence of social capital, including both internal (bonding) and external (bridging and linking) social capital, on principals’ well-being, following a longitudinal approach. We suggest for governments to invest in communities or networks of principals and to restructure principals’ tasks, for example, by introducing co-principalships.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.