
Abstract
The robotic surgical systems and computer-assisted technologies market has seen impressive growth over the last decades, but uptake by end-users is still scarce. The purpose of this article is to provide a comprehensive and informed list of the end-user requirements for the development of new generation robot- and computer-assisted surgical systems and the methodology for eliciting them. The requirements were elicited, in the frame of the EU project SMARTsurg, by conducting interviews on use cases of chosen urology, cardiovascular and orthopaedics procedures, tailored to provide clinical foundations for scientific and technical developments. The structured interviews resulted in detailed requirement specifications which are ranked according to their priorities. Paradigmatic surgical scenarios support the use cases.
Introduction
Computer-assisted surgery (CAS) or robotically assisted surgery (RAS) relies on specially devised machines and equipment to enhance a part of or an entire surgical procedure. Surgical robotic systems are a combination of robotic and imaging equipment, surgical accessories, software and services that assist surgeons in performing various types of minimally invasive surgery (MIS) (e.g. gynaecological, cardiovascular, neurological, urological and orthopaedic). Robotic systems facilitate dexterous teleoperation of surgical tools, with a view to reduce invasiveness and to improve efficacy and precision by miniaturization, improved stability, natural coordination, enhanced surgeon ergonomics and increased dexterity. Additional benefits may include reducing post-surgical complications, blood loss, post-operative pain, better tissue healing as well as faster recovery and reduced hospital costs compared to conventional surgery. 1,2 In addition, robotic manipulators help surgeons to work on less accessible parts of the body via small ports. For example, robotic surgery has been extensively used to enhance the excision of prostate, affected by cancer, given the difficulty in accessing the prostate in conventional laparoscopic surgery, which requires extensive experience. 2 Collectively, the characteristics of the robotic systems aim to reduce surgical invasiveness and enhance patient outcomes.
The global medical robots market is expected to reach US$12.80 billion by 2021 from US$4.90 billion in 2016, growing at a Compound Annual Growth Rate of 21.1% (http://www.marketsandmarkets.com/PressReleases/medical-robotic-systems.asp (accessed 20 November 2017)). Key players in the global medical robots market include Intuitive Surgical Inc. (Sunnyvale, CA, USA), Stryker Corporation (Kalamazoo, MI, USA), Mazor Robotics Ltd (Israel), Hocoma AG (Switzerland), Hansen Medical Inc. (Mountain View, CA, USA), Accuray Incorporated (Sunnyvale, CA, USA), Omnicell, Inc. (Mountain View, CA, USA), Ekso Bionics Holdings, Inc. (Richmond, CA, USA), ARxIUM (Buffalo Grove, IL, USA) and Kirby Lester LLC (Lake Forest, IL, USA) (http://www.marketsandmarkets.com/PressReleases/medical-robotic-systems.asp (accessed 20 November 2017)). To date, the race to develop, acquire and incorporate this emerging biomedical technology has been primarily driven by the market and the industry. While several robot-assisted MIS (RAMIS) systems have gone through feasibility trials for clinical validation, regulatory approvals and commercialization, their actual use is still scarce compared to conventional surgical procedures. Global adoption of these systems in clinical practice is still sporadic 3 except for the da Vinci surgical system (Intuitive Surgical Inc., USA) which has played a major role in RAMIS in the last two decades. Although the use of robotic systems has been tested in several surgical sub-specialties, that is, cardiovascular, thoracic, urological, gynaecological, paediatric, and general surgery, 3 surgeons in these specialties are still not inclined to use these technologies. This lack of market penetration may have been triggered by poor training programmes, excessive cost, need for reconfiguration of conventional surgical theatres as well as reported suboptimal results in some surgical areas. 4 The U.S. Food and Drug Administration (FDA, Maryland, USA) has reported a marked increase in adverse events associated with robotic surgery during 2006–2013, and this may have triggered more caution in the surgical field while prompting refocus for the development of more advanced and safer devices. 4 Surveys with surgeons suggest that inclination to the technologies is often associated with the gold standard for a surgical procedure at a given time, which is connected to the statistical success of a specific technique and indirectly to its cost. 5 Furthermore, it has been reported that only 3% of the RAMIS cystectomies in the United States were completed without converting to the open technique. 6 The slow adoption is perceived to be increased difficulty due to the handling of sensitive structures as well as working in a confined space.
The Society of American Gastrointestinal and Endoscopic Surgeons has initiated work on finding a consensus on robotic surgery including guidelines for training and credentials, indicating goals on instrumentation, visualization, integration and simulation. 7 Efforts have been carried out to assure that patient safety is the top priority when envisaging a new robotic solution to be used to enhance surgical performance. 8 In a previous study on decision-making and assistive robotic technologies in surgery, 9 a qualitative analysis was performed to evaluate four critical characteristics of surgical assistance systems, that is, situational awareness, lack of tactile feedback, immersion and impact of ergonomics. This study also provides surgeons’ requirements that are essential in designing more advanced robotic systems. However, the study was only focused on one surgical specialty, that is, colorectal surgery and was constrained to the context of decision-making. Bonfè et al. 10 used the requirements engineering methodology to collect surgeons’ requirements for a software-intensive and intelligent surgical robot on three chosen actions, that is, needle insertion for ablating procedure, laparotomy and suturing a wound. A group of experts was interviewed to obtain the goal model, which was used to express structural constraints and behaviours in a software system. In the study by Stollnberger et al., 11 a group of stakeholders, that is, doctors, patients and assistants, was interviewed, and the feedback was collected for the development of a robotic medical system which is able to conduct ultrasonography and physical examination remotely. The latter study was focused on simple use cases, such as suturing a wound. Facilitating factors and barriers for adopting robotic systems among health-care professionals have also been investigated. 3 After semi-structured interviews, one of the main facilitator factors for adopting a robotic system was ‘Perceived Usefulness’. ‘Perceived Usefulness’ regards functions with the robot – better visualization, increased precision, better dexterity, elimination of hand tremor, better suturing, better instrumentation, better angle of placement, easier access and better ergonomics. A new RAS system is expected to have the perceived usefulness. Relevant shortcomings of the current system functionality could be elicited by analysing end-user requirements. Titan Medical Group (Canada) has included a process focused on a clear and limited set of customer-centric requirements in the development of a single-port robotic surgical system. 12 As presented, 13 the development of first-generation robotic systems was generally focused on early stage developments. With no following through, the systems lack capturing in the final product of critical later stage developmental aspects. Also, earlier studies were limited in duration and showed little involvement from the end-users. It is consequently debatable whether they cover their actual needs. A qualitative study by Aaltonen and Wahlström 14 was focused on three aspects: enhancing surgical operation outcome, user experience and learning. The study selected technological solution concepts based on a technology review and an ethnographic study. It is acknowledged by the authors that the study does not provide a complete list of user requirements nor it facilitates meaningful discussions. Also, the ethnography study is only useful to address the contextual factors such as usability and investigating collaborative work settings, 15 for example, in the case of software requirements elicitation too.
The purpose of this qualitative study was to gather the end-user requirements to design an improved surgical system, that is, within the SMARTsurg project (http://smartsurg-project.eu/ (accessed 20 November 2017); https://www.youtube.com/watch?v=AgPkMSqxRfs&t=15s (accessed 20 October 2018)), by determining the barriers of the methods and systems currently used and what advancements are needed specifically for the user interface (master), surgical instruments, vision and features such a haptic feedback and so on. The SMARTsurg project aims at developing an advanced system for RAMIS, focusing on reducing the surgeon’s cognitive load related to the system’s operation to enhance shorter training time, while delivering more accuracy, safety, reduced procedure time and expanded surgical applicability. To this end, the project aims to design and develop a wearable interface for a surgical system using (a) highly dexterous surgical instruments, (b) wearable hand exoskeletons with haptic feedback and (c) wearable smart glasses for augmented reality guidance of the surgeon based on the real-time three-dimensional (3D) reconstruction of the surgical field. Previous work included investigations on a wearable system of three-finger hand exoskeletons and anthropomorphic three-finger gripper. 16 High dependability will be achieved by utilizing real-time dynamic, active constraints (ACs) to the instruments’ motion in order to restrict it to the safe regions. SMARTsurg developments will employ a user-centred approach for efficient technology adoption and commercialization. This will be achieved using short prototyping and testing cycles supported by focused end-user and commercial requirements.
We followed a qualitative data analysis approach 17 for gathering the multi-user specific requirements, where urologists, cardiac and orthopaedic surgeons were involved considering the design of SMARTsurg system and targeted procedures. This article aims to illustrate the results of the requirements elicitation derived for the urology, cardiovascular and orthopaedic use cases, which would be accounted in the system design and implementation process. Once the current standardized workflow was defined using the controlled vocabulary in the graphical format, elicited requirements have been prioritized according to surgeons’ needs. Also, the conceived surgical scenarios by mapping requirements to surgical workflow are herewith presented.
Methods
Definitions and controlled vocabularies
In order to provide a standard methodology for the surgical intervention descriptions, for example, as shown in Figure 1, the consensus was reached among the SMARTsurg consortium on the following terminology:
Surgical phases indicate a collection of surgical activities, which need to be performed in a particular sequence to accomplish the surgical workflow. The aim of each phase is to reach/target the principal surgical site. For example, in the ‘Tumour excision’ phase of robot-assisted partial nephrectomy (RAPN), which involves removal of kidney tumour, the surgeon first identifies the site for tumour by cutting Gerota’s fascia, then he/she does the markings on the kidney capsule to expose the tumour area for resection.
Surgical steps are the tasks required to accomplish the phases of the procedure. Each step consists of a specific action, anatomical locations and instruments. For example, during ‘Tumour excision’ (phase), the surgeon does the ‘clamping’ (step) of the ‘renal artery’ (anatomical location) by ‘clamp’ (action) through the ‘Laparoscopic Bulldog clamp’ (instrument). Sometimes, the steps correspond to the same linguistic meaning, where the phases consist of only one step. For example, ‘Bowel mobilization’ phase has only one step, that is, ‘mobilization’.
Surgical actions are carried out by surgical instruments in surgical steps, for example, ‘cortical suturing’ (step) by the ‘large Needle Driver’ (instrument) to ‘suture’ (action) the ‘kidney’ (anatomy) during the repair of the kidney, ‘renorrhaphy’ (phase), at the end of the procedure.
Surgical instruments are used during a single step of the surgery. Surgical instruments indicate robotic instruments, for example, ‘fenestrated Bipolar’, in left and right robotic arm. Instruments, for example, ‘laparoscopic Bulldog’, used by assistant surgeons are also considered.
Anatomical locations are the anatomical landmarks, for example, ‘gerotas Fascia’, on which an instrument performs a surgical action.

Definitions are shown in italics, for example, ‘Surgical phase’. The orange arrows show the hierarchical relation between these definitions, for example, ‘Surgical step’ is a part of ‘Surgical phase’. The figure shows an example of ‘Tumour Excision’ phase of RAPN. RAPN: robot-assisted partial nephrectomy.
Use cases
The use cases were selected to contextualize the focused requirement elicitation process and to elicit application scenarios that specify targeted phases and steps, which collectively form workflows, during implementation and evaluation of system’s components. The identified use cases are as follows: Orthopaedic surgery Robot-assisted partial lateral meniscectomy (RaPLM): A meniscus tear is a common knee joint injury. RaPLM is the surgical removal of all or part of a torn meniscus. Robot-assisted repair of lateral meniscus tear (RaLMR): A meniscus tear, if not severe, RaLMR is performed to repair the part of a torn meniscus. Urological surgery Robot-assisted radical cystectomy (RARC) and intracorporeal reconstruction with ileal conduit or orthotopic neobladder: RARC is performed to remove the cancerous bladder. Here, intracorporeal reconstruction with ileal conduit or orthotopic neobladder indicates the reconstruction of urinary diversion to urethra after removal of the bladder. Robot-assisted radical prostatectomy (RARP): RARP regards prostate cancer removal, where the entire prostate gland along with some of the surrounding tissue is removed. RAPN: RAPN regards kidney tumour removal, where a tumorous portion of the kidney is removed. Cardiovascular surgery Mitral valve (MV) leaflet repair (MV mending surgery): MV mending surgery is done when the MV is too loose or severely leaking. MV replacement with an artificial valve is done when the MV is too calcified and not opening well. Coronary artery bypass grafting (CABG): CABG is advised for a selected group of patients with significant narrowing or blockage of the coronary artery.
The detailed procedural workflows (consisting of phases, steps and instruments) of the use cases are outlined in Appendix 1. Procedural definitions and use cases workflows were confirmed after a consensus within the clinical partners of the consortium. Each surgical workflow includes workflow entities, for example, ‘Phase’, ‘Steps’ and ‘Instruments’.
User requirement collection and data analysis
We interviewed non-expert and expert surgeons in the surgical specialties. They expressed their views on potential barriers, limitations and improvements of current surgical systems for CAS and RAMIS. We conducted a total of 29 interviews. As per the breakdown of specialties, we interviewed 6 orthopaedic surgeons (1 senior, 3 mid-careers and 2 juniors), 17 urologists (7 seniors, 3 mid-careers and 7 juniors) and 6 cardiac surgeons (4 seniors, 1 mid-career and 1 junior). The mean age of orthopaedic surgeons, urologists and cardiac surgeons was 41, 43 and 39.2 years, respectively. Urologists were from Italy and the United Kingdom. Orthopaedic surgeons were from Greece, while the cardiac surgeons were from the United Kingdom and Greece. The interviewees are all male surgeons from Europe. However, in a span of 1 year, this was the maximum achievable number of surgeons within the specialties with a higher gender ratio, for example, urology, cardiovascular surgery and orthopaedic surgery. For example, the female surgeons count for only 8% in cardiac surgery, 10% in urology and 6% in orthopaedics in the United Kingdom. 18 In Italy, less than 10% of urologists are female. Worldwide statistics of urologists’ gender is difficult to find, but in most countries, majority of urologists are male, for example, in Japan 95% and in the United States about 93%. 19 As for surgeons’ skill levels, we interviewed 12 seniors, 7 mid-careers and 10 junior surgeons. A detailed information on the surgeon’s experience with open, MIS and RAMIS is shown in Table 1.
Interviewed surgeons’ experience with open surgery, MIS and RAMIS.
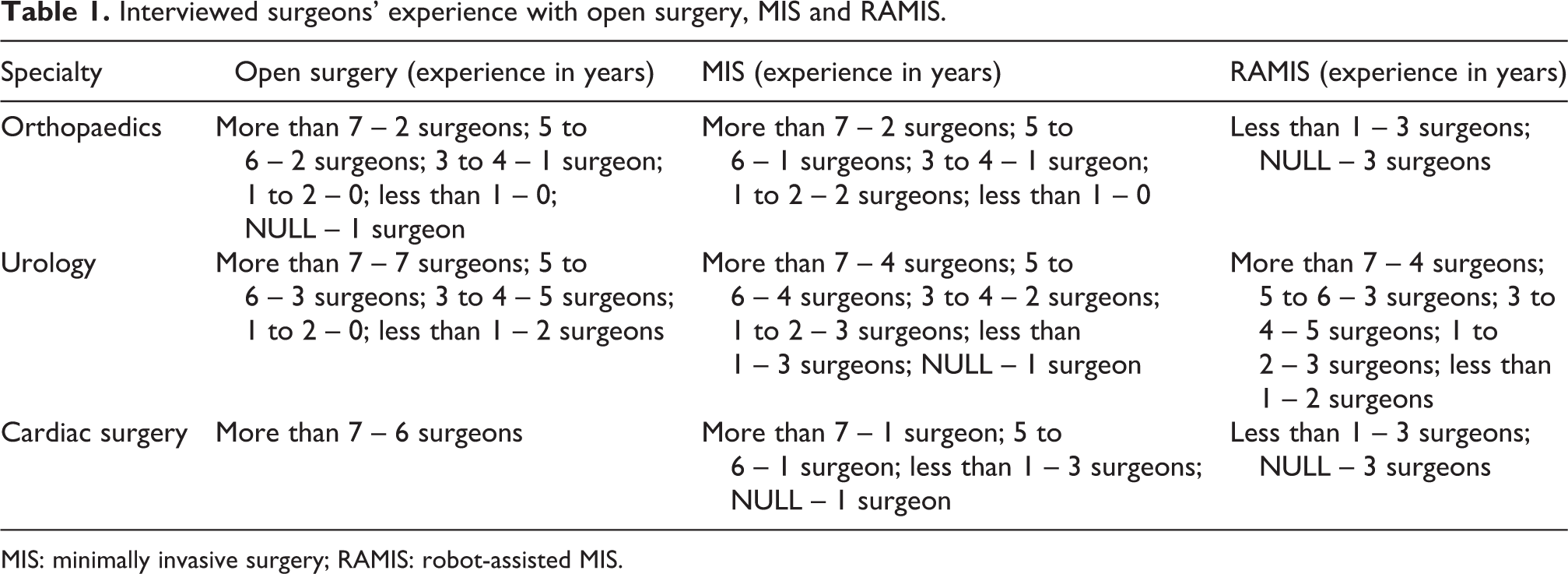
MIS: minimally invasive surgery; RAMIS: robot-assisted MIS.
Expertise level was determined by surgeons themselves. We interviewed surgeons with different levels of experience, where the questions were particularly designed consisting of understanding the limitations of open and laparoscopic surgeries as well, considering the lack of RAMIS experience of orthopaedics and cardiovascular surgeons as compared to urologists. Moreover, during the interviews, the surgeons were provided with the printed slides of surgical robotics technologies (see the Online Supplementary Material), which were explained to them to understand how certain technologies would be helpful to improve proposed use cases. The slides consist of reported examples of physical hardware blocks, for example, master–slave design, vision components and so on which explained to be not taken as the foreseen solutions, but only as suggestions that will be adaptable to the actual surgical requirements. The surgeons allowed to freely think of their own application and to imagine the complexity they need without sticking to reported images. Finally, after the interview, a slide showing the prospective SMARTsurg system was explained and specific questions related to the system were asked, for example, ‘How do you expect a system like SMARTsurg will improve in new surgeons training?’.
Structured interviews were conducted either face-to-face, telephone or via computer call. In all cases, interviews were recorded in audio format as raw data. Participants gave written informed consent, and the data collection procedure was approved by Politecnico di Milano Ethical committee (opinion n. 5\2017). Similarly, the University of the West of England interviews and data collection were done in accordance with the recommendations of the University’s policy on research ethics, approved by the Faculty of Environment and Technology Research Ethics Committee (UWE REC REF No: FET.17.04.038).
Two types of questions were used during the interviews
‘Open-ended’ questions, where surgeons expressed their opinions in the descriptive form; and
‘Close-ended’ questions, where surgeons gave the answers in the form of Yes/No or surgeons expressed the answers by selecting one or more options (categories/concepts).
After the interviews, recordings were transcribed, and the data were subsequently organized. Answers were grouped for each question in the questionnaire. We assigned each surgeon an ID, that is, the first letter of each specialty followed by the user number, for example, O1, O2 and so on for orthopaedic surgeons; U1, U2 and so on for urologists; and C1, C2 and so on for cardiac surgeons.
The first analysis was conducted employing ‘within-case analysis’
17
method, where surgeons’ responses for individual surgical case study were explored in detail, as a standalone entity, to discern the patterns revealed in the individual interviews (e.g. ‘within-case analysis’ of collected interview data of orthopaedic surgeons, urologists and cardiac surgeons separately). The ‘within-case analysis’ was used to identify common categories/concepts from each surgical use case. To construct the categories, we did manual open coding.
20
A code is a word, phrase or sentence that represents aspect(s) of the data or captures essence or features of the data. The purpose of coding is to reduce the data into meaningful segments and assign names (codes) to those segments. The names of categories were defined by the domain expert in surgical robotics, or by participant’s exact words or the literature sources relevant to the study. Categories are related to (1) the phenomenon under study; (2) the contextual, intervening-structural and causal conditions; (3) the actions to handle the phenomenon; and (4) consequences of actions and interactions related to phenomenon.
20
For example, in the sentence, “Surgeons are familiar with the use of instruments. Generally, there are problems with the tissues e.g. thin meniscus. We may need smaller instruments. Current instrument diameter is approximately 2 cm.”
Further on, a disaggregation of core themes/categories, that is, ‘axial coding’ was applied to the collected information. 21 Axial coding is the process of relating codes (categories and concepts) via a combination of inductive and deductive thinking. The grouped categories are also mapped to prospective system hardware components. There are also decision blocks, for example, ‘Are all the user requirements examined?’ regards the elicited requirements that would help eliciting essential requirements of a system, where ‘NO’ decision states reanalysing the transcripts and the defined codes, and ‘YES’ decision states the essential user requirements are met and no further analysis is required. Closed questions, which inform explicit requirements to test surgeon’s opinion on them, were analysed using the analytical approach. In such cases, we found the requirements by analysing the categorical data.
‘Across-case’ analysis and elicitation of application scenarios
To do the ‘across-case analysis’, the elicited requirements obtained using the ‘within-case analysis’ were first prioritized and scored, as shown in Table 2.
Priority level and associated scores for the elicited user requirements.

The priority levels and scores for user requirements were obtained from a consensus among the clinical partners during the SMARTsurg 1st PC Meeting (Milan, Italy, 10–11 of July 2017). After deciding the priorities and scores, each of the elicited requirements with the same categories from different specialties was grouped together.
User requirements were considered mandatory requirements, that is, for the SMARTsurg system, if total priority scores of requirements from three specialties were summed up to ≥ 14. The non-mandatory requirements (total score ≤ 13), which include high and medium-high requirements (total score ≥ 10 but ≤ 13), were also analysed with the same method, but these priorities may be further extracted from the application scenarios. The threshold scores on the elicited requirements were decided as a trade-off between their complexity and the project’s resources. To extract the application scenarios, elicited requirements for each specialty were mapped to the individual phases and steps of use cases considering ‘within-case’ and ‘across-case’ analysis. Information on the use case phases and steps were obtained from the use cases’ workflows. The full user requirements analysis methodology is shown in Figure 2.

A flow chart of the user requirements analysis methodology.
Results
‘Within-case’ analysis
Appendix 2 (Tables 2A to 2C) represents, ‘within-case’ analysis of surgeons’, feedback obtained through the interviews. Multiple utterances or discussions by the same surgeon were also considered for eliciting the requirement if the meaning of the utterances was different concerning the requirements. In each table, surgeons’ feedback is reported for each feedback/requirement in the sequence of questions in user requirement questionnaire. The ‘within-case’ has identified 13, 18 and 14 different categories of elicited requirements of orthopaedics, urology and cardiac surgery use cases, respectively. For orthopaedic surgery, the category ‘anatomical problem’ was discussed seven times, more than any other category. The haptic feeling (17 times) and image quality (9 times) were predominantly discussed for urology and cardiovascular surgery use cases. In all the specialties, vision is stated as a barrier due to the small and difficult to access anatomical structures by camera. Contrary to this, the urologists, who have greater experience with the RAMIS than the other two specialist groups, discussed the need to improve the current camera systems, highlighting the limitation of camera resolutions, larger length of the camera shaft and so forth. Similarly, all surgeons also are in favour of small articulated and flexible instruments which could overcome the problem of efficiently accessing the anatomical structures, for example, MV or meniscus structure. The need for haptic feeling when suturing, dissecting and identifying the normal tissue, for example, kidney as well as the abnormal tissues, for example, tumour was also prioritized. All surgeons agreed that their postures are non-ergonomic during the surgery. Having a third tool digit is considered for tissue manipulation, for example, stabilization, repairing and suturing, as well as grasping and replicating instrument’s movements as in, for example, Castroviejo-type instruments for heart surgery. However, surgeons need graspers which could provide more force to grasp the tissue. Instrument tip swapping could be helpful in reducing infections, saving the operative time as well as replacing the task performed by assistants. For more interactive experience, urologists and cardiovascular surgeons prefer immersive stereo viewer, while orthopaedic surgeons prefer the smart glasses. Superimposing preoperative images to identify anatomical structures intraoperatively was favoured by all surgeons. Only the cardiovascular surgeons would like to see physiological data intraoperatively, for example, blood pressure. They also need communication with their team, where immersive stereo viewer could be helpful in order to provide a holistic view of the procedure. As an alternative sensory information, visual cues are most favourable except for cardiovascular surgeons. While orthopaedic surgeons do not need to have any ACs, urologists and cardiovascular surgeons think that this could be a helpful feature for preventing injuries of the critical structures, for example, blood vessels but also for the surgical training. On the topic of surgical training, some surgeons prefer the existing training methodology, while some, especially urologists, would like to use these technologies, for example, haptics to improve understanding of the procedure and dexterity. The major concerns about these technologies are their costs, teleoperation for manipulating tissues (especially to orthopaedic surgeons) and patient safety, usability and improvement with respect to the currently available robotic systems, for example, synchronized simultaneous movements of slave robot arms with the patient table. A detailed information on results of ‘within-case’ analysis is shown in Appendix 2. Functional requirements, which are elicited from the interviews, are reported in Table 3. Functional requirements could be helpful in the development of technical specifications for system components.
Functional requirements.

MV: mitral valve; CABG: coronary artery bypass grafting; RAPN: robot-assisted partial nephrectomy; 3D: three-dimensional; HD: high-definition; UHD: ultra high-definition.
Across-case analysis
In Table 4, each cell is represented with the elicited mandatory requirement with its necessity in three specialties, that is, urology (U), orthopaedics (O) and cardiac surgery (C) (priority levels: 5 = high; 4 = medium-high; 3 = medium; 2 = medium-low; and 1 = low). After carrying out ‘within-case’ analysis, we elicited 13, 18 and 14 distinct categories of elicited requirements for orthopaedics, urology and cardiovascular surgery, respectively. A total of 33 user requirements have been elicited, on which the across-case analysis is done, out of which 4 requirements (e.g. superimposed preoperative images, ACs, articulated instruments and hand exoskeleton as a master system) are the mandatory requirements, that is, priority score ≥ 14. After the ‘across-case’ analysis, application scenarios were chosen. The main reason to conduct across-case analysis was to allow for a versatility of the systems matching the requirements in order to be used for different purposes in the hospital. Examples of application scenarios on all the use cases are reported in Table 5. The non-mandatory requirements (from no. 5 to 33) are presented in Appendix 3.
‘Across-case’ analysis – mandatory requirements.
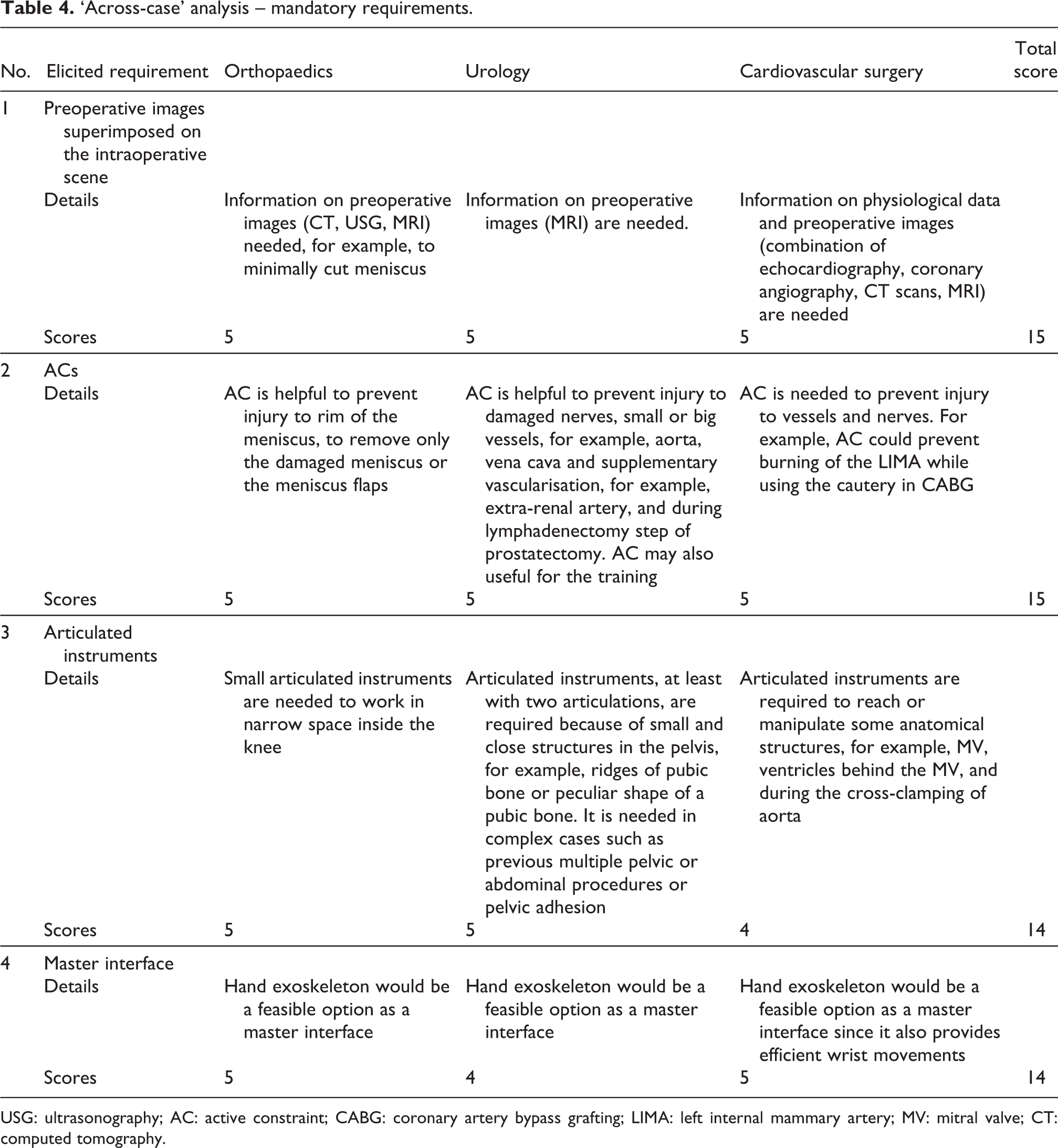
USG: ultrasonography; AC: active constraint; CABG: coronary artery bypass grafting; LIMA: left internal mammary artery; MV: mitral valve; CT: computed tomography.
Application scenarios for RAPN, RARC, RARP, RaPLM, RaLMR, MV surgery and CABG.a

AC: active constraint; RAPN: robot-assisted partial nephrectomy; RARC: robot-assisted radical cystectomy; RARP: robot-assisted radical prostatectomy; RaPLM: robot-assisted partial lateral meniscectomy; RaLMR: robot-assisted repair of lateral meniscus tear; MV: mitral valve; CABG: coronary artery bypass grafting; LIMA: left internal mammary artery; LAD: left anterior descending artery; 3D: three-dimensional.
a The table demonstrates the use of technology (‘elicited requirement’) with respect to the use cases of the study. Phases and steps correspond to the use cases workflow, as shown in Appendix 1. As an example, application scenarios on RAPN such as hand exoskeleton, better image quality, smart glasses (for assistants) and 3D images for visualization are needed in all the phases of RAPN. During preparation of the kidney, ACs could be used to prevent the injuries to vasculature such as the aorta or vena cava as well as organs such as the liver and the spleen. After that, during the excision of the tumour, preoperative images are superimposed to see the renal artery, while incising the renal capsule before clamping the artery. After the preoperative images are superimposed, ACs could be used to prevent the injury to renal arteries. Afterwards, haptics could be used for the closure of renal breach during suturing and pulling of the thread while doing the suturing of the kidney.
Discussion
We discuss four mandatory requirements, that is, total score ≥ 14, namely ‘superimposed pre-operative images’, ‘Active constraints’, ‘Articulated instruments’ and ‘Master system – hand exoskeleton’. The discussion is split specialty-wise, following orthopaedics, urology and cardiovascular surgery, except for the ‘Master system – hand exoskeleton’, where the requirement was discussed considering all specialties.
Superimposed preoperative images
Orthopaedic surgeons use X-ray and magnetic resonance imaging (MRI) as preoperative images. They were not sure if it is possible to superimpose preoperative images because preoperative and intraoperative images often have different orientations. The preoperative images are being taken in the supine position when the knee joint is flexed during the surgery. However, there are a few landmarks that could be useful for image registration, for example, medial and lateral femur condyle, anterior cruciate ligament, trochlea and medial compartment of the tibia. Urologists use computed tomography (CT), ultrasonography and MRI as preoperative images. The preoperative and intraoperative images are always a little different for urology use cases. There is a little difference in the parenchymal organs, for example, kidneys, but images could change for other organs, for example, the peritoneum so that the image registration could be difficult. However, superimposed images could be helpful to understand the relative positions of the organs, for example, where a tumour or ureter is. Urologists suggested landmarks that could be useful for registration, for example, vessels like the aorta, organs like spleen, lower and upper poles of the kidney during RAPN, nerves, seminal vesicles, pubic bone and the apex of the prostate during RARP, and the middle lobe of the prostate and pubic symphysis during RARC. Urologists suggested that superimposed images are useful in specific surgical steps of these use cases as, for example, during the nerve-sparing in RARP or to identify a tumour during RAPN because these anatomical regions are visible on MRI. They suggested that superimposing preoperative images could also be useful to identify the enlarged lymph nodes in unusual locations. However, surgeons need ‘on and off’ functionality for this feature. In RARP, base of the prostate is clearly visible which provides the precise coordinates as well as the apex. These coordinates can be used to determine the site of lesions for the image fusion. Cardiac surgeons use a combination of echocardiography, coronary angiography, CT or MRI as preoperative images. They suggested that it is possible to superimpose preoperative images because there is not much difference between preoperative and intraoperative images for these two use cases. However, it is hard to define the landmarks in beating heart surgery. Otherwise, there are enough landmarks available, for example, appendages or great vessels such as the aorta and the apex of the heart. Cardiac surgeons also suggested superimposing the CT information on the smart glasses or conventional loupes, which they referred to as ‘smart loupes’.
Active constraints
Despite orthopaedic surgeons initially stated that they do not need ACs, further discussions with the panel of expert orthopaedic surgeons, who also have some experience with robotics and MIS, at SMARTsurg 1st PC meeting in Milan, concluded that ACs are needed and could be useful to prevent injuries to the rim of the meniscus. Moreover, AC could be used to minimize cutting of the meniscus during surgery. ‘Parrot beak tear’ and ‘Flap tear’ are exceptional cases, where the ACs could help just to remove the flaps. Moreover, in the case of ‘Bucket Handle Tear’, ACs could be helpful to restrict the movement of the instrument in the red zone of meniscus where the success of the repair is very high. So, in this case, ACs could be helpful to prevent injury in the red-white and whitezone. It could also be helpful to prevent injury to the peroneal nerve during the cauterization for meniscectomy. For urologist, the AC is useful during the lymphadenectomy step of radical prostatectomy to prevent injuries to arteries, veins and nerves or to prevent injury to accessory vessels coming from the pelvic wall side. It could also be useful for the nerve-sparing in RARP. In RAPN, it could be helpful to prevent injury to vena cava and aorta. However, many urologists believe that ACs should only be implemented for surgical training and for junior surgeons. They also need the overriding functionality as they think that it could be a distraction, confusing and may increase the surgery time. For cardiac surgery use cases, ACs would help avoiding many vital structures, for example, vessels, nerves and so on, involved in the surgery. During CABG, in harvesting the left internal mammary artery (LIMA), surgeons have to be cautious not to get too close to the LIMA while cauterizing, where the ACs would be useful.
Articulated instruments
Due to the small area of the complex knee anatomy, orthopaedic surgeons need articulated instruments for suturing of the meniscus tear as well as for visualizing the damaged structures in 3D. For urological use cases, articulated instruments may be especially helpful for RARP. There are structures in the pelvis, very small and in close proximity, for example, ridges of the pubic bone. In complex cases where there are adhesions in pelvis or abdomen, movement of the instruments in the pelvis is difficult due to the peculiar shape of the pubic bone, and the surgery is performed in the narrow area between the prostate and the rectum. Surgeons need articulated instruments to obviate frequent change of ports and gain better access to anatomic sites. The current cardiovascular surgery instruments do not provide 360° rotational movements. During cardiovascular surgery, it is difficult to access some anatomical structures, for example, the access to the heart is provided from the anterior side, while the MV is on the posterior side. Articulated instruments could be helpful to access the ventricles behind the MV and for cross-clamping of the aorta during retrograde cardioplegia.
Master system: Hand exoskeleton
Concerning the hand exoskeleton, surgeons need them for both hands, and they welcome the possibility of using all fingers instead of the index–thumb grip of the current system. The hand exoskeleton should be lightweight and adjustable for different hand sizes with an accompanying armrest. The design of the exoskeleton needs to take into account the limitations of wrist movements and how this can be transferred to the surgical instrument. Specifically, in cardiac surgery use cases, the ability of the exoskeleton tracking a three-finger pencil grip is highly essential. Surgeons also need haptic feedback on the hand exoskeleton for assessing forces which they apply in various surgical tasks.
Limitations of this study and conclusions
Although the elicited requirements were comprehensive, the limitation of this study is the underlying inequality in the number of surgeons interviewed in different surgical specialties and their gender imbalance. However, during the ‘across-case’ analysis, prioritization and analysis have been made on a common set of requirements between the specialties, so the elicited requirements have wide applicability. Moreover, applicability could come from the already wide application base, for example, seven different use cases from orthopaedics, urology and cardiovascular surgery, thus the elicited requirements could be generalized to a broader range of surgical systems. The proposed framework from eliciting requirements could be an interesting approach to obtain a common set of user requirements in a development of the cross-disciplined robotic systems considering technologies and interfaces. Although the interviews were conducted within multi-specialty and at different centres, other health-care professionals, for example, nurses or anaesthetists from different countries were not included, which may further elicit new requirements, for example, requirements of new technologies in the preoperative phase.
Supplemental material
Supplemental_material_Questionnaire_presentation - Requirements elicitation for robotic and computer-assisted minimally invasive surgery
Supplemental_material_Questionnaire_presentation for Requirements elicitation for robotic and computer-assisted minimally invasive surgery by Hirenkumar Nakawala, Elena De Momi, Antonia Tzemanaki, Sanja Dogramadzi, Andrea Russo, Michele Catellani, Roberto Bianchi, Ottavio De Cobelli, Aristotelis Sideridis, Emmanuel Papacostas, Anthony Koupparis, Edward Rowe, Raj Persad, Raimondo Ascione and Giancarlo Ferrigno in International Journal of Advanced Robotic Systems
Footnotes
Author’s note
Elena De Momi and Giancarlo Ferrigno are now affiliated with Department of Electronics, Information and Bioenginnering (DEIB), Politecnico di Milano, Milan, Italy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project has received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement No. H2020-ICT-2016-732515.
Supplemental material
Supplemental material for this article is available online.
Appendix 1
Appendix 2
Appendix 3
‘Across-case’ analysis: Non-mandatory requirements.

| No. | Elicited requirement | Orthopaedics | Urology | Cardiovascular surgery | Total score |
|---|---|---|---|---|---|
| 5 | Image resolution | ||||
| Details | Better image quality is helpful. | Better image resolution, for example, 4K (3840 × 2160 px) – Ultra HD image quality | Good image resolution, at least at the level of conventional loupes, is needed. Surgeons also require magnification (2.5× to 3.5×) and a larger field of view (from 1.5 mm2 to 5 cm2) | ||
| Scores | 5 | 3 | 5 | 13 | |
| 6 | Three-fingered instrument | ||||
| Details | The three-fingered instrument could be helpful to stabilise the meniscus in meniscus repair. It could also be useful to view knee compartments, to cut free cartilage pieces, and to repair tendons and nerves. | Urologists do not need the three-fingered instrument. However, they would like to try first if implemented. The wrist articulation is missing in three-fingered instrument and it may not provide same articulation as the da Vinci single port. | The three-fingered instrument is helpful for cutting the sutures. The cardiac surgeons also showed a willingness to try on a prototype. | ||
| Scores | 4 | 4 | 5 | 13 | |
| 7 | Smart glasses | ||||
| Details | Smart glasses are required for assistants and for surgical training. | Smart glasses are required for assistants and for surgical training. | Smart glasses are required for assistants and surgical training. | ||
| Scores | 5 | 3 | 4 | 12 | |
| 8 | Haptics | ||||
| Details | Haptics could be required during the tissue manipulation. | Haptics could be required to feel the planes between prostate and rectum, to feel pushing and pulling tissues, thread tension during suturing. It is also helpful for surgical training. | Haptics could be useful to feel the calcium deposit in the coronary artery. | ||
| Scores | 3 | 3 | 4 | 10 | |
| 9 | 3D images | ||||
| Details | 3D images are helpful for better visualisation. | 3D images are helpful for better visualisation. | |||
| Scores | – | 5 | 5 | 10 | |
| 10 | Alternative haptic sensation | ||||
| Details | As an alternative haptic feedback, visual cues could be helpful. | As an alternative haptic feedback, visual cues could be helpful. | Cardiac surgeons do not prefer to have an alternative haptic sensation, but they only prefer the naturalistic feedback. | ||
| Scores | 3 | 5 | 1 | 9 | |
| 11 | Extended visual feedback | ||||
| Details | Extended visual feedback is helpful to put the suture through the meniscus and to feel the correct length; to see popliteal artery, where more narrow or flexible camera is also needed. | Extended visual feedback is helpful in radical prostatectomy or trans-corporeal reconstruction to see big vessels, renal arteries behind fat and lymph nodes near vena cava or aorta. | Extended visual feedback is helpful to see the critical structures in heart, for example, aorta. | ||
| Scores | 1 | 5 | 3 | 9 | |
| 12 | Flexible camera | ||||
| Details | Flexible camera is required to look around corners. For example, it could be used similar way as automatic flexible cystectomy, flexible sigmoidoscopy or colonoscopy. | Flexible camera is required to reach or visualise some anatomical structures, for example, mitral valve, ventricles behind the mitral valve, and during the cross-clamping of aorta. It should be designed like a bronchoscope. | |||
| Scores | – | 5 | 3 | 8 | |
| 13 | Needle holder (slave side) | ||||
| Details | A new needle holder for suturing is required in meniscus repair. | New instruments or modification to existing instruments is needed, for example, small needle drivers | |||
| Scores | 5 | 3 | – | 8 | |
| 14 | Instrumentation | ||||
| Details | A new needle holder for suturing is required in meniscus repair. | New instruments or modification to existing instruments is needed. For example, thin instruments and small needle drivers are useful aiding minimally invasiveness. Bigger instruments to handle bowel (larger jaws and more force on tissue), to take specimen out and retractors for tissue retraction would be helpful. An easier system to put clips, for example, Hem-o-lok clips and disposable instruments are required. | |||
| Scores | 5 | 3 | – | 8 | |
| 15 | Immersive stereo viewer | ||||
| Details | An immersion stereo viewer is required for better immersive experience. It should be used by surgeons. | An immersion stereo viewer is required for better immersive experience. It should be used by surgeons. | |||
| Scores | – | 3 | 4 | 7 | |
| 16 | Camera control | ||||
| Details | Orthopaedic surgeons prefer using joystick or exoskeleton or hand control. | Head movements are required to control the camera. | Cardiovascular surgeons require voice control, specifically in the big field, and another finer control in the focused field. | ||
| Scores | 3 | 1 | 3 | 7 | |
| 17 | Physiological data | ||||
| Details | Orthopaedic surgeons do not need to see the physiological data. | Urologists do not need to see the physiological data. | The physiological data, for example, vital signs which needs to be verify repeatedly, is essential in cardiac surgery. | ||
| Scores | 1 | 1 | 4 | 6 | |
| 18 | Small instruments | ||||
| Details | During RaPLM and RaLMR, knee positions and camera ports are generally required to change repeatedly for better visualisation and manipulation. There are also tissue problems, for example, thin meniscus, where the smaller instruments, at least size of current instrument, for example, 4 mm, are would help for doing surgery through medial meniscus posterior horn for stitching of meniscus tear. | ||||
| Scores | 5 | – | – | 5 | |
| 19 | Teleoperation | ||||
| Details | Teleoperation is required for minimal meniscus resection because surgeons’ posture is not good during RaPLM and RaLMR. | ||||
| Scores | 5 | – | – | 5 | |
| 20 | Instrument jaw grip | ||||
| Details | Instruments which could provide pencil grip-like mechanism are required. | ||||
| Scores | – | – | 5 | 5 | |
| 21 | Magnified vision | ||||
| Details | Magnified vision is helpful for better visualisation | ||||
| Scores | – | 5 | – | 5 | |
| 22 | Magnified haptic/force feeling | ||||
| Details | The exaggerated haptic feeling is required to reduce iatrogenic complications. | Realistic haptic feedback is required. | For clinical purposes, it should not be magnified, but kept within the physiological ranges. | ||
| Scores | 1 | 3 | 1 | 5 | |
| 23 | Surgeon’s position | ||||
| Details | Ergonomic surgeon’s position is required. | Ergonomics and surgeon’s position should be considered when constructing the actual master interface. | For cardiovascular applications, resting the forearms while operating with fingertips is important to minimise tremor. | ||
| Scores | 1 | 1 | 3 | 5 | |
| 24 | Camera size | ||||
| Details | Due to smaller access to the operating area, the size of camera should be less. | ||||
| Scores | – | – | 4 | 4 | |
| 25 | Teleoperated vision system | ||||
| Details | Teleoperated vision system is helpful to remove camera handling by assistants. | ||||
| Scores | – | – | 3 | 3 | |
| 26 | Master interface size | ||||
| Details | The small interface is desired (35–40 cm2). | ||||
| Scores | – | – | 3 | 3 | |
| 27 | Instrument tip swapping | ||||
| Details | Instrument tip swapping is helpful. | Instrument tip swapping is helpful because it remove the need of changing the instruments. | Instrument tip swapping is helpful. | ||
| Scores | 1 | 1 | 1 | 3 | |
| 28 | Manipulation with left-handed surgeon | ||||
| Details | Modification to current instruments is needed for left-handed surgeons. | ||||
| Scores | 1 | – | – | 1 | |
| 29 | Field of view | ||||
| Details | Wider field of view may be helpful to see the assistants’ instruments and remove the need of changing the ports. Field of vision should be as larger as possible or needs to be able to ‘look around corners’. | ||||
| Scores | – | 1 | – | 1 | |
| 30 | Clutching mechanism | ||||
| Details | New clutching mechanism is needed because frequent clutching is required to handle the workspace limitation. | ||||
| Scores | – | 1 | – | 1 | |
| 31 | Easier understanding of surgical workflow steps | ||||
| Details | It is difficult to handle complex surgical cases and follow the open surgery approaches by the junior surgeons, where explicit procedural guidance may be helpful. | ||||
| Scores | – | 1 | – | 1 | |
| 32 | Tissue grasping mechanism | ||||
| Details | Urologists require newer grasper which could provide more force to grasp tissues. | ||||
| Scores | – | 1 | – | 1 | |
| 33 | Length of camera shaft | ||||
| Details | Short camera length may be helpful to stop clashing of instruments with assistants. | ||||
| Scores | – | 1 | – | 1 |
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.