
Abstract
The hinotori™ surgical robotic system, by Medicaroid (Medicaroid Corporation, Kobe, Japan), is a new robotic system for minimally invasive surgery. We aimed at evaluating its usability and accessibility in a preclinical setting. This was a preclinical feasibility study. Two groups of surgeons, one with three experienced robotic surgeons (group 1) and one with three robotic-surgery naive participants (group 2), performed the following tasks using the hinotori™ system in a simulated preclinical setting: console setup, docking, instrument exchange, undocking, and suturing. Each participant repeated each task three times. The time required for performing each repetition and the count of failed repetitions were the primary outcomes of the study. The subjectively perceived workload in performing the tasks, as measured by the NASA-TLX score, was the secondary outcome. The improvement of participants within the three repetitions as well as a comparison between the performances of group 1 and 2 were evaluated. The time required to perform each task decreased with repetitions for both groups, so did the subjective workload score. The time measures required to perform the tasks and the mental effort scores were comparable between the two groups for the console setup, docking, instrument exchange, and undocking tasks. The NASA-TLX score was also comparable between the two groups for the console setup and the emergency undocking tasks and decreased significantly within all tasks after the third repetition. The incidence of failed repetitions was higher in group 2 for the suturing task, however the difference was not statistically significant. The results confirmed the usability of the hinotori™ system in a preclinical setting for both highly trained surgeons and nonexperienced operators and its accessibility for both long-time users of other systems and first-time users.
Keywords
Background
The landscape of robotic surgery is expected to witness significant advances in the near future as new platforms for robotic assisted surgery will enter the market.
Three main types of surgical robots are currently being used in everyday practice: multiport laparoscopy robots, single-port laparoscopy robots, and needle insertion systems. 1 Moreover, several procedure-specific systems have been developed for neurosurgery, 2 head and neck surgery, 3 and ophthalmology. 4
Multiport systems are the most widely adopted in general surgery, as they most closely resemble the laparoscopic setting and provide the same wide accessibility to the abdominal and thoracic cavity. Notable advantages of the robotic approach compared to “conventional” laparoscopy include the improved vision field (usually provided by 3D vision systems), the wider intracorporeal range of movement, and the suppression of the physiological hand tremors.
The daVinci™ surgical system (Intuitive, Sunnyvale, California, USA) is currently the most popular and widely used in general surgery worldwide. The latest available model, the daVinci Xi™, includes a movable bed-side cart with four robotic operating arms. The robotic arms are remotely controlled by the surgeon through an interactive control platform. The system also includes a multifunctional cart-coupled operating bed.
Several new systems have been developed in the last years, most of them featuring a slightly different modular design compared to the four-arm supporting cart of the daVinci and comprising separate bed-side units, each supporting a single robotic arm. The Dexter™ robotic system from Distalmotion (Distalmotion, Épalinges, Switzerland) features two separate arm-supporting movable bed-side units designed to be fully integrated in the laparoscopic surgical field with the possibility of a quick transition from robotic to laparoscopic surgery. 5 With the Hugo™ robotic-assisted surgery system from Medtronic (Medtronic, Minneapolis, Minnesota, USA) and the Versius™ surgical system from CMR Surgical (CMR Surgical, Cambridge, UK), the operators can use up to four arm-supporting mobile bedside unit that can be flexibly positioned in the operating room to conduct fully robotic or robotic-assisted operations. The systems also feature open consoles designed to enable quick interaction for the surgical team and in-person access to the surgical site. The usability of both systems has been recently evaluated in both the preclinical 6,7 and the clinical setting. 8 –11
The hinotori™ robotic system is a novel surgical robot developed by Medicaroid (Medicaroid Corporation, Kobe, Japan). The hinotori™ consists of a full high-vision 3D console and a patient-side cart with four eight-axis robotic arms (Figure 1), 12 designed to reduce the arm-to-arm or the arm-to-assistant interference for smoother movements. The software-derived pivotal point of the instruments is designed to clear the workspace around the trocars, eliminating the need for arm-to-trocar docking.

The hinotori™ patient’s side cart.
The hinotori™ system is currently approved for use in Japan. Only one study involving the use of the system for the evaluation of basic features for potential tele-surgery is mentioned in the literature, 13 while no usability preclinical or clinical study has currently been published. Moreover, no contemporary studies on systems with a four-fixed-arms design, other than those involving the daVinci™ systems, are currently available. Aim of the present study is to investigate the usability profile of the hinotori™ in a preclinical setting, both for extensively trained and for untrained robotic surgeons. We expect to demonstrate that the system is readily approachable by both types of users when performing basic perioperative and intraoperative tasks.
Methods
In this preclinical observational feasibility study, two groups of surgeons were assigned to complete perioperative and intraoperative tasks using the hinotori™ system. Group 1 consisted of three surgeons with previous robotic training in dry lab, wet lab and experience of more than one hundred robotic procedures in patients, performed using the DaVinci Xi™. Group 2 consisted of three surgeons without specific robotic training and only observational experience in robotic surgery. The study took place at the Medicaroid Europe headquarters in Düsseldorf in a simulated operating theater environment. Following a basic training on the main features of the hinotori™ system, the participants completed a series of exercises by running through a simulated surgical workflow. All exercises were performed using the hinotori™.
Since this was a preclinical study, not involving human subjects, the approval by the Institutional Review Board of our Department was not needed.
Workflow organization
The participants completed a 20-min briefing to be instructed on how to complete the tasks and were allowed a 20-min practice of the tasks, with the objective of achieving as many repetitions as possible. Both groups then performed the same tasks in a timed setting. The training sequence was randomized for group 1 and group 2, so that the same group was not always the first to perform a task. The order of the trainees performing each task was also randomized in each group. As one group performed each task, the other group was blinded in order to avoid “passive-training.”
Each task was repeated three times by each participant. Two observers followed the participants during each task to record the time required for the completion of the task and the eventual failures in completing the task. The study design was summarized in Figure 2.

Design of the study. Reps.: repetitions.
Operating room organization and robotic system configuration
The following equipment related to the robotic system was placed in the operatory room (Figure 3): the console, the patient-side robotic cart, and a standard operative bed. An instrument cart was also used to place the instruments during the various phases of the training.

Operating room map (view from above).
The main body of the robotic system is represented by the bedside cart. The bedside cart supports four separate robotic arms, each featuring seven adjustable joints and an instrument-docking site, overall providing up to eight degrees of movement. The system does not require an arm-to-trocar connection: the trocars’ pivotal point is calibrated by using a company designed pointer that needs to be attached to each arm and pointed at the trocars’ entry site. 12 Upon calculation of the pivotal point, each arm is automatically set at the correct position and the instruments can be inserted.
Training definition
Each group was assigned to perform the following tasks: console activation and setup, cart and arm docking, emergency undocking, instrument exchange, and suturing.
Task 1: Console activation and setup
For this task, participants were asked to switch the console and the bedside cart on, set a language and a user profile and set the bedside cart in the draping position.
Inability to proceed in this activation sequence without assistance was defined as failure of the task.
Task 2: Cart and arm docking
For this task, participants were asked to push the robotic cart from the draping position at the side of the operatory room to the side of the surgical bed, perform the pivotal point calibration on each of the four arms, introduce the camera through the optic trocar and three instruments under direct vision, setting the robotic system on its final operative position (Figure 4).

The robot-docking task.
We used a standard robotic-surgery setting, with the optical trocar at the center, a needle holder on the “right hand,” left grasper on the “left hand” and the scissor on the fourth arm (Figure 5). The tasks were performed on a commercially available laparoscopy box trainer.

The trocar and instrument setting used in the study.
Inability to complete a passage of the sequence without assistance was defined as failure of the task.
Task 3: Emergency undocking
This task was performed starting with the robot fully docked in the final position described for the previous task (Figure 5). Participants were required to simulate an emergency conversion scenario, thus removing all instruments and the camera from the robotic arms and pulling back the robotic cart to provide enough space for two surgeons to approach the operative field from both sides (Figure 6).

The emergency undocking task.
Failure of this task was defined as the inability to complete a passage of the emergency undocking sequence without assistance.
Task 4: Instrument exchange
The instrument exchange task was also started with the robotic cart docked and the instruments in the operative position (Figure 5). Participants were required to remove an instrument and insert a new one, the action had to be repeated on each of the three operative arms (Figure 7).

The instrument exchange task.
For this task, both failed attempts and failure of the task were recorded. A failed attempt was defined as the incorrect placement of the new instrument signaled by the system, requiring the participant to remove and insert the instrument again without assistance. Failure of the task was defined as the inability to proceed in the sequence without assistance.
Task 5: Suturing
During the suturing sequence, the following subtasks were evaluated separately: needle grasping, needle driving, and knot tying. The task was performed on a commercially available silicon suture training pad simulating a 10 cm linear wound. We used a nonabsorbable monofilament polypropylene 3/0 10 cm-long suture (Ethicon, Raritan, New Jersey, USA) with a 26 mm 1/2-circle round bodied needle.
Subtask 5.1: Needle grasping
The task was performed using the setting depicted in Figure 5. The needle was placed in an easily reachable position near the suture pad and was marked at the correct grasping position. Participants were allowed to use both the grasper and the needle holder and were asked to place the needle in the needle holder grasping it at the correct marked position with the needle perpendicular to the needle holder.
The task was classified as “passed” when the 3 mm-wide correct-position mark was grasped; “passed with difficulty” when the needle was grasped within 3 mm to the left or to the right of the correct-position mark and “failed” when the needle was grasped at any other point (Figure 8).
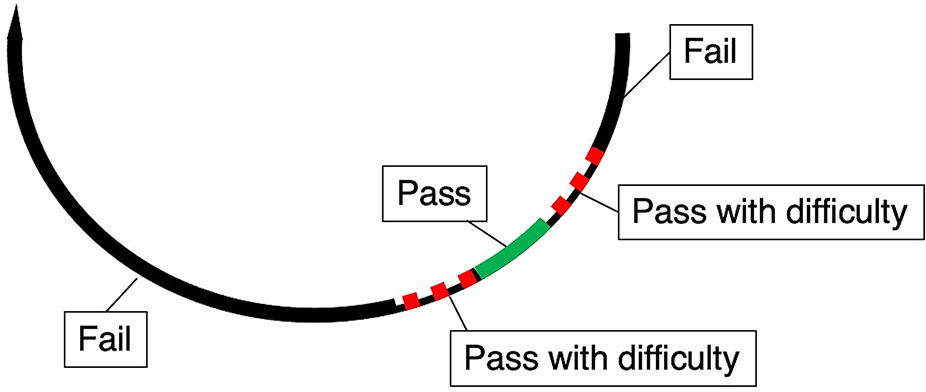
The needle grasping task.
Subtask 5.2: Needle driving
This subtask was started with the needle already in position. The action flow is summarized in Figure 9. Participants had to insert the needle through the tissue at the marked insertion point (first passage), they were then allowed to reposition the needle in the needle holder, drive it through the tissue (second passage) and extract the needle through the marked extraction point. Both points were marked on the suture pad and had a 1 mm radius.

The needle driving task.
This task was classified as “passed” when the needle was successfully driven through both the insertion and the extraction point; “passed with difficulty” when either the insertion or the extraction points were missed and “failed” when both points were missed.
Subtask 5.3: Knot tying
This subtask was started with the stitch already passed through the tissue after the previous task. Participants were asked to secure a surgical knot (Figure 10) and two simple knots. The trocar setting was depicted in Figure 5.

The knot tying task. The first knot (surgical knot) is depicted in the figure.
Inability to proceed without assistance, failure to secure the knot, failure to perform a knot with the correct form, and breaking of the suture were all criteria for failure of the task.
Outcome evaluation
Primary outcomes of the study were the time required for the completion of each task and the proportion of failed and successful repetitions. The differences in the outcome measurements between group 1 and group 2 and the improvement achieved by each group by repeating the task were evaluated as metrics of the system’s usability and accessibility to untrained surgeons. For the suturing task, the three subtasks (needle grasping, needle driving, and knot tying) were evaluated separately and only the intra-group performance was evaluated as comparing group 1 and group 2 was deemed noninformative given the absence of previous robotic training for group 2.
Secondary outcome of the study was the assessment of the subjectively perceived mental workload required when using the system. This was assessed by administering all participants the NASA task load index (TLX) 14 after each task repetition. The NASA TLX is a tool to determine a subjective overall workload rating when performing a task. The workload is assessed through six dimensions: mental demand, physical demand, temporal demand, effort, performance, and frustration. Subjects can rate each dimension on an interval scale ranging from low (1) to high (100). The overall workload can score between 0 and 100. Subjects can also be offered 15 pairwise combinations of dimensions to select which from each pair has the most effect on the workload. The final NASA TLX score can therefore be used as either raw or weighted. In this study, the raw-NASA TLX score was used.
Statistical analysis
Comparison of measured times and scores of the questionnaires were performed using the Friedman test for repeated measure, the Mann–Whitney U test, the nested t-test, and the nested one-way ANOVA as appropriate. Categorical variables were compared using the chi-square or the Fisher’s exact test as appropriate. Time was expressed in seconds (s). NASA-TLX scores as numbers ranging from 1 to 100. Continuous variables are presented as means. A two-sided p value of <0.05 was considered statistically significant.
Results
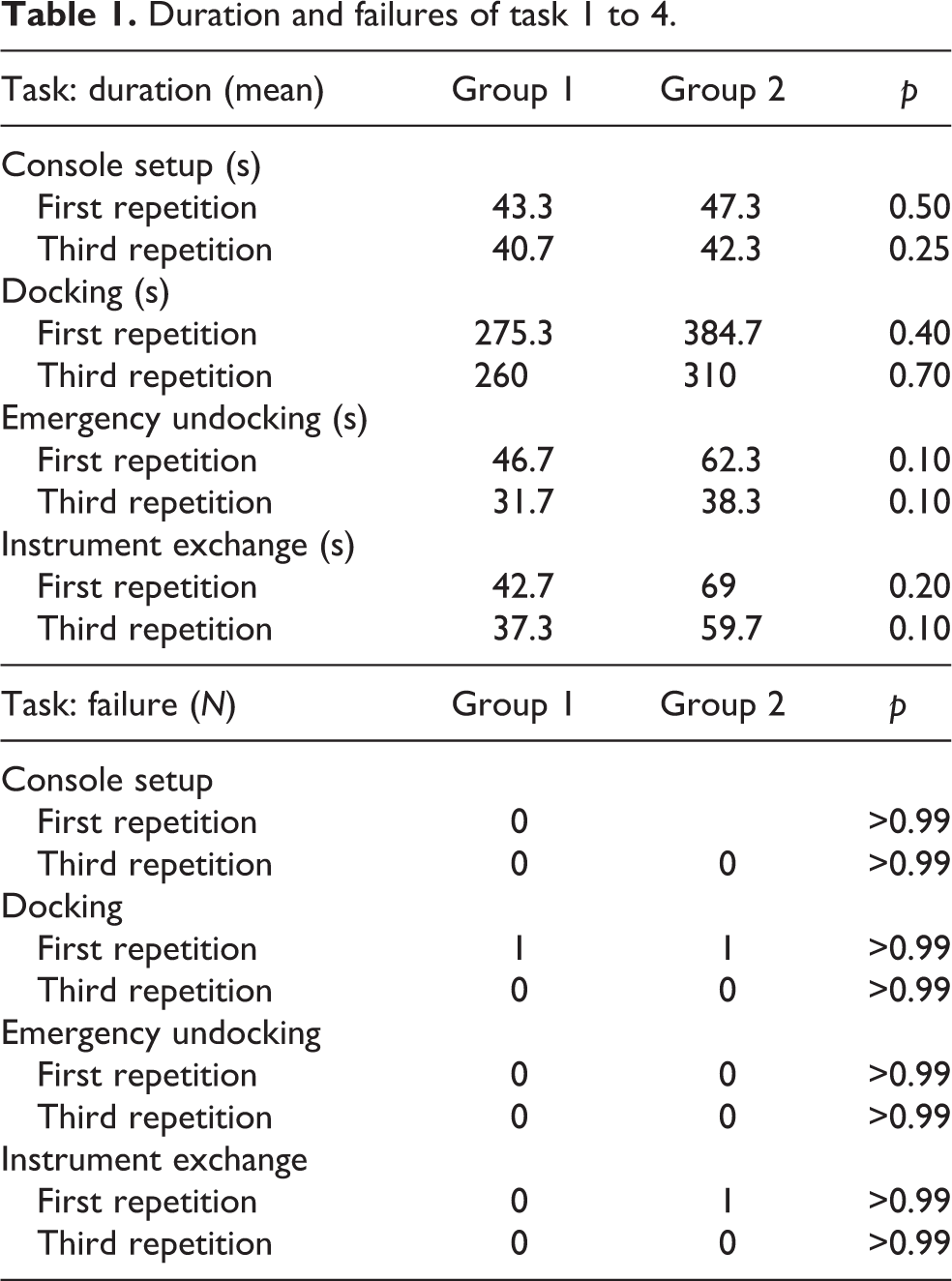
The performance of the two groups on the four tasks are shown on Table 1. Docking was the most time-consuming task for both groups with a mean of 272.8s for group 1 and 341s for group 2. All the participants showed an improvement of their times comparing the first to the last attempts. The improvement of group 1 was statistically significant for the docking task (p = 0.0278, Figure 11).
Duration and failures of task 1 to 4.

Docking times of group 1.
The emergency conversion task was completed with a mean of 37s for group 1 and a mean of 48s for group 2. Group 2 showed a statistically significant reduction of the time needed to complete the task (p = 0.0278, Figure 12).

Emergency conversion times of group 2.
Instrument exchange could be carried out in 41s for group 1. The second group needed more time with a mean of 62.8s.
The performance of group 1 with the needle grasping task is summarized in Figure 13(a). The mean time for the first repetition was 9.3s and 5.4s for the third repetition (p = 0.19).

Time measurements of the needle grasping task for group 1 (a) and group 2 (b). Each dot represents one participant. Rep: repetition.
Group 2 needed 12.4s for the first and 8.2s for the third repetition (p = 0.19) (Figure 13(b)).
The mean time required for group 1 to perform the needle driving task was 17.7s for the first repetition and 11.4s for the third repetition (p = 0.18) (Figure 14(a)). Group 2 needed 25.2s at the first repetition and 17.1s at the last one, the improvement within the three repetitions was significant (p = 0.03) (Figure 14(b)).

Time measurements of the needle driving task for group 1 (a) and group 2 (b). Each dot represents one participant. Rep: repetition.
Both groups improved significantly during the knot tying task (p = 0.03). Group 1 required 126 and 92.9s for the first and third repetition, respectively (Figure 15(a)), while group 2 went from 245.8s at the first repetition to 128.7s at the last repetition (Figure 15(b)).

Time measurements of the knot tying task for group 1 (a) and group 2 (b). Each dot represents one participant. Rep: repetition.
Failed attempts were recorded in two cases for the docking task (one for each group) and in one case for the instrument exchange task, no significant difference was detected between the two groups (Table 1).
The error tracking for the suturing subtasks is evaluated descriptively in Table 2. Overall, no failures occurred in group 1 during the suturing task, while three failures were detected in group 2 (11%, p = 0.07). “Pass with difficulty” occurred in only one repetition for group 1 (3.7%) and in five repetitions (18.5%) for group 2 (p = 0.08). All subjects passed the task at the last repetition.
Error tracking of the suturing subtasks.

PWD: pass with difficulty.
Participants’ subjective evaluation of the workload required for each task is reported in Table 3. The scores reported in every column represent the mean of all three subjects for each repetition. Overall, the perceived difficulty in performing the tasks decreased significantly with each repetition for both group 1 and group 2. Paired comparisons between group 1 and group 2 for each repetition of each task are reported separately in the right column. No significant difference between the two groups was detected after the console setup and the undocking tasks. Conversely, a significant difference on the perceived workload was reported after all repetitions during the suturing and the docking tasks. During the instrument exchange task, no difference in the perceived workload was detected between the two groups after the last repetition. The docking and the suturing tasks were the more subjectively demanding, with a mean Raw NASA TLX score of 20.1 and 22, respectively.
Subjective workload evaluation.

TLX: task load index; rep: repetition; instr: instrument; emerg: emergency.
Discussion
The main aim of the present study was to evaluate the feasibility of the tested robotic system throughout a series of key tasks in the everyday routine of robotic surgery, that is, console setup, docking, instrument exchange, and suturing.
The console setup task was designed to evaluate the “first-impact” accessibility of the system for a first-time user, as switching up the system and setting up the software to begin the operation is commonly one of the first action performed by a surgeon facing a robotic procedure. We were not allowed to publish details of the software interface in this study, however the relatively low time required for the task and the low perceived workload demonstrates the accessibility of the system. The fact the no significant difference in both procedural time and NASA-TLX score was detected among the two groups, confirms the usability of the software also for unexperienced users.
Although docking was the most time-consuming task, it is a standard procedure and could be mastered effectively also by the unexperienced surgeons, as shown by the comparable task duration. The subjective workload index remained significantly higher in group 2, although it decreased remarkably after the third repetition. It must be kept in mind that the docking is probably one of the most delicate tasks to perform in robotic surgery and also an action that surgeons without previous robotic experience are completely naive with.
The adoption of a “pointer-based” pivotal point identification system represents one of the innovations introduced by this robotic system, with the main advantage of simplifying the robot-to-trocars connection thus reducing the obstacles at the operating table. The risk of collision between the robotic arms is also reduced, as no direct connection between the arms and the trocars is required, other than the inserted surgical instruments. The procedure of pivot pointing the robotic arms to virtually connect them to the range of the trocars, however, must be trained and represents an essential step of preparation for the surgery with this robotic system. The operator has to be careful in this phase to avoid inadvertent injuries at the abdominal wall by excessive approximation of the pointer. The use of a soft pointer or of a laser pointer system instead of a rigid instrument could be considered as a further development of the system.
The instrument exchange task is not a complicated procedure. Interestingly, the subjectively perceived workload decreased remarkably in group 2 as subjects got familiar with the sequence, so that at the last repetition no significant difference was detected in the workload score between the two groups. Moreover, less than a minute was required from both groups to achieve a complete instrument exchange. The fact that this step is one of the most common steps in any robotic operation makes the task really important, especially if we take into consideration the cumulative effect that such a step holds for major operations with a large number of instruments and thus a high number of instrument exchange throughout the operation. 15 –18 To further highlight the reason for conducting such a task, we provide the following scenarios: an elective change of instrument in order for example to clip a vessel with clip applier is a controlled situation, whereas trying to achieve hemostasis from an oozing vessel with the use of the same aforementioned clip applier is an emergency situation that both require an instrument exchange. In both cases, the same instrument must be connected with a robotic arm, must be identified as such from the system, must be placed via the trocar at the activating position, and then the clip can be applied. Whether urgent or elective, the task must be feasible simple and quick to carry out. All these mentioned features were met for the hinotori™ system in our study.
Ruurda at al. showed in their study from 2004 that an experienced surgeon needed significantly less time to perform a single stich (81.4 vs. 95.9s; p = 0.005) with the use of the robotic assistance in comparison to laparoscopic surgery without the use of the robot. 19 Since the hinotori™ is a completely new system, with no previous preclinical or clinical evaluation, comparison with the commercially available systems regarding the suturing time exceeded the scope of this study. Moreover, since it was previously demonstrated 19 and it is also quite reasonable that skilled robotic surgeons will perform better than surgeons with no previous robotic experience in suturing tasks, we decided not to include a group 1 versus group 2 comparison of the suturing tasks in this study. However, we believe it is remarkable how the group 2 participants significantly improved in needle driving and knot tying in the timed task and that this result was paralleled by a marked reduction in the workload score for this group. The fact that also group 1 participants improved significantly in the timing during the knot tying task probably confirms how the system proved to be easy to get accustomed with, both for new users and for subjects who are likely to be long-time users of other systems.
The emergency conversion, although less needed in the daily routine with an incidence of less than 1% in major operations, is a crucial situation that requires agility from the operating team. Two neuralgic points should be considered in this scenario. First, the position of the robotic console with respect to the patient’s bed site, as it may influence the time required for the first surgeon to scrub in and be active on the operating table. Second, the time of undocking of the robotic arms, so that the patient can be reached from both sides, is of paramount importance. 20 –22 Several study have now demonstrated the crucial role of this task, and the importance of implementing the acquisition of this skill in a robotic surgery curriculum. 23 –25 In our study, we concentrated on finding out whether the assistant could fully free the patient from the robot and the results were remarkable. In almost 30s (mean of both groups 30.5 s), the robot was fully removed from the patient and the surgical field was readily accessible from both sides. Remarkably, times of execution and workload score were both comparable between group 1 and 2 since the first repetition, and this confirms the safety of the system as this crucial task could be immediately mastered also by first-time users. This result could probably be explained by the fact that the trocars are not in direct contact to the robotic arms (the robot uses the pivot point mentioned in the “Introduction” section in order to triangulate and calculate the trocar position and movement), thus making the task of removing the instrument easy and feasible even for robotic-surgery naive participants.
We must here critically comment the fact that the setting is not clinical and such an emergency situation cannot be directly comparable to our task where no stress is applied.
This study has limitations inherent to the number of participating trainees and tasks’ repetitions that limit the power and feasibility of the statistical analysis. Indeed, each group consisted of only three participants, making the study sample size relatively small. It has however to be kept in mind that this is the first ever preclinical usability study performed using the hinotori™ robotic system. We believe the reported data support the feasibility of the system and its accessibility also for nontrained physicians, thus paving the way for further studies in both the preclinical and clinical setting. Also, we believe our results provide a relatively wide set of reference values that should be the benchmark for any future study evaluating the performance of the hinotori™ and, potentially, of other robotic systems.
Conclusion
The results after our first assessment of the hinotori™ system in a preclinical setting showed a feasible system that required substantially low subjective workload for both novice and advanced surgeons. The system is much appealing for further evaluation in clinical studies.
Footnotes
Acknowledgments
We acknowledge the contribution of Stefano Varotto, from the multimedia service of the Department of Surgical, Oncological and Gastroenterological Sciences of the University of Padova, in the creation of the tasks’ images.
Authors’ note
The two authors Giovanni Capovilla and Evangelos Tagkalos contributed equally to the realization of this manuscript and therefore share the first authorship.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.