
Abstract
This article reports our findings from a robot-assisted therapeutic study conducted over 49 days to investigate the sociopsychological and physiological effects in children with autism spectrum disorder using a parrot-inspired robot, KiliRo, that we developed to help in therapeutic settings. We investigated the frequency of participants’ interactions among each other and assessed any changes in interaction using social network analysis. Interactions were assessed through manual observation before and after exposure to the robot. Urinary and salivary tests were performed to obtain protein and α-amylase levels, respectively, to report the physiological changes in participating children with autism spectrum disorder before and after interacting with the robot. This is a pioneering human–robot interaction study to investigate changes in stress levels using salivary samples. Systolic and diastolic blood pressure, heart rate, and arterial oxygen saturation level in blood were also monitored to investigate the physiological changes in participating children before, during, and after interacting with our parrot-inspired robot, KiliRo. The results show that the robot can help increase social interaction among children with autism spectrum disorder and assist in learning tasks. Furthermore, the clinical biochemistry test report using urinary and salivary samples indicates that the stress levels of children with autism reduced notably after interacting with the robot. Nevertheless, blood pressure, heart rate, and oxygen levels in blood did not show positive change in all participants.
Keywords
Introduction
Centres for Disease Control and Prevention in the United States estimated that in 2014 about 1% of the world population has some form of autism spectrum disorder (ASD). 1 That is, approximately, 74 million people around the world may potentially be diagnosable with ASD. The lifetime cost of an individual with ASD in the United States averages from 1.4 million to 2.4 million USD. 2 A few important characteristics of ASD include behavioral and psychological challenges such as lack of social interaction and communication as well as persistence with sensory activities. Researchers in the recent decades have explored numerous ways to help improve the lifestyle of children with autism. Like various other therapy methods, robot-assisted therapy is explored in various settings to help children with autism in learning, social interaction, physiological, and psychological needs. 3 –8
Robot-assisted therapy to improve psychological and physiological functioning, learning, and social interaction abilities of children with autism has been finding new directions in recent years. Specifically, bioinspired robots were used in numerous studies and reported success in improving the learning and social interaction abilities of children with autism. Furthermore, these robots were also able to help reduce psychological stress and improve physical activities in these children. Nao is a human-like intelligent robot initially used extensively in soccer playing robot competitions. 9 In recent years, researchers have also used Nao robot in autism therapy giving various benefits such as improving learning, social interaction, and joint attention. 8,10 –12 In improving joint attention, the robot served as an object to mediate joint attention between the children and an adult. In another study AIBO, a dog-like robot proved to be successful in improving social interaction in children with autism. 13 In this study, the authors introduced a dog-like robot to 11 children identified with symptoms of autism and reported that the participants were much more interactive with the robot than with a noninteractive dog-like toy. Paro, a seal-like robot, has also been used to report success in improving social interaction abilities through various studies. 14 –16 ERIC is a dog-like robot developed to help elderly in providing therapeutic benefits. 17 Probo is an imaginary animal-like robot used in autism therapy to improve social interaction. 18 Bovolenta et al. investigated the effects of using robot-assisted therapy for upper limbs in patients after stroke. 19 The authors also evaluated the acceptance by patients for using robot-assisted therapy. This study involved 14 patients and reported positive for using robots in therapeutic settings with stroke patients. The authors argued that the therapists involved in this study were positive toward using robots from an organizational point of view and with regard to the responses received from patients in clinical-rehabilitative responses. Hamada et al. proposed a recreation program by designing games for the elderly with dementia using AIBO, a dog-like robot. 20 This study claimed that robot-assisted therapy can help improve and prevent dementia in elderly.
Animal-like robots have been developed by highlighting the benefits of their living counterparts in animal-assisted therapies (AATs). The need for developing bioinspired robots has been centered around the risk and challenges of using real animals. For instance, dogs were used extensively in AAT with numerous reported benefits. 21 –23 Nevertheless, hospitals and doctors show limited interest due to the fear of biting, allergy, safety, and ethical issues of using animals. 24 –26 From the perspective of animals being used in therapeutic settings, there is clearly no consideration given to the willingness of these animals to be engaged in such activities. Bioinspired robotics provides a solution to these problems by retaining the benefits of their natural counterparts while overcoming the shortfalls.
There are many species that are known to have proven therapeutic benefits to human beings. They include dogs, cats, canines, pink dolphins, guinea pigs, rabbits, reptile, and parrots. 27 –32 After dogs, cats, and fish, parrots are thought to be the most common household pet. 32 Parrots have been used in therapeutic settings and have provided remarkable benefits to human society. Parrots are good at mimicking the human voice and other sounds. These birds are naturally able to speak and engage in two-way conversations with humans. 33 Pepperberg, an animal psychologist from Harvard University, has reported the intelligence of parrots through many studies. 33 –36 Particularly, her reports on Alex, the African grey parrot, indicated that parrots are not only able to speak but can also engage in two-way conversation. Pepperberg reported that Alex could identify 50 different objects and understand the concept of smaller, bigger, same, and different. 37
Parrots have also been used in therapeutic setting to help people with mental or physical disorders. An African grey parrot named Sadie was able to help his owner who had bipolar disorder with psychotic tendencies. Sadie helped his owner by repeatedly saying “calm down” when needed. 38 In another setting, the parrot was used in therapy to assist patients with post-traumatic stress disorder among war veterans in the United States. 39 It is also reported that the parrots are helpful in therapeutic settings with psychiatric patients. 32 The distinct feature of talking ability in parrots is very relevant and helpful in improving learning and social interaction abilities of children with autism. Parrots have been used in elderly care and autism therapy earlier. For instance, an elderly care center in Japan implemented parrot-assisted therapy and reported improvement in various senses, such as sight, sound, and smell, in elderly. 40 In the United Kingdom, a study involving a child with autism reported calming behavior after interacting with a Caique parrot that was used as an emotional support animal. 41
Nonetheless, using parrots among children with autism is still a risky choice due to natural behaviors and potential allergic reactions caused by these birds. One common behavior issue reported by parrot owners is biting. 42 Having large beaks, parrots can cause severe harm to humans. Diseases spread through birds are also a threat to parrot owners. Particularly, parrot fever, spread by birds through the bacteria called Chlamydia psittaci can cause fever, nausea, diarrhea, and cough. 43
To overcome these challenges in parrot-assisted therapies, we have developed an artificial parrot robot, KiliRo, that mimics its natural counterpart in therapeutic settings retaining the merits while overcoming the shortfalls. In this article, we present the preliminary evidence that the parrot-inspired robot that we developed can help improve learning and social interaction abilities and provide psychological benefits to children with ASD through stress reduction.
Method
System architecture of KiliRo
The parrot-inspired robot, KiliRo, is shown in Figure 1. The body frame of our KiliRo robot was fabricated using polylactic acid and thermoplastic polyurethane materials. We used a 3-D desktop printer for printing the parts of KiliRo. The robot consists of three parts: upper, middle, and lower body. The upper part consists of one head with two eyes and a beak; the middle part consists of a body with two wings and one tail; and the lower part consists of two legs. The head has one degree of freedom enabling it to turn left and right. The beak and each wing has one degree of freedom to move up and down. The legs of the robot have two degrees of freedom allowing movement forward or backward and turning left or right. Two wireless cameras and one USB camera achieve almost 270° field of vision. In addition, to achieve real-time video transmission, the robot platform is capable of recognizing alphabets and numbers through the use of quick response (QR) codes.
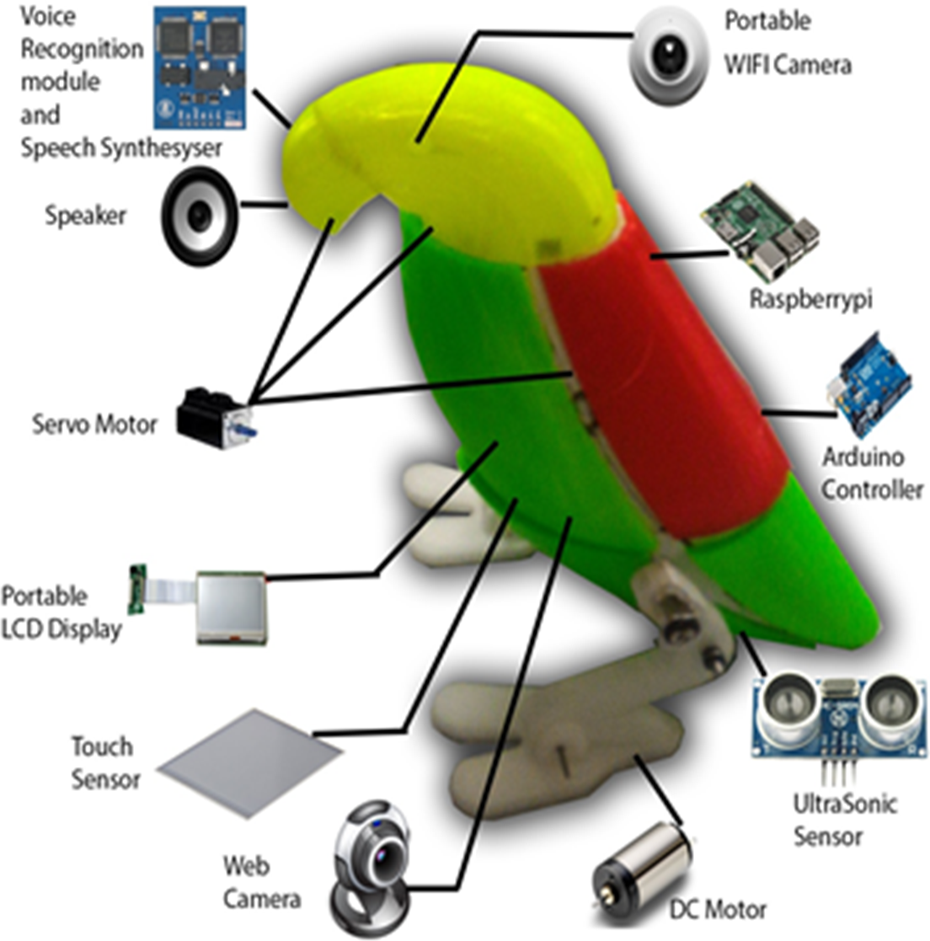
KiliRo—parrot-inspired robot.
QR code is a 2-D machine-readable barcode containing pre-stored information. The robot is capable of recognizing English letters of the alphabet from “A” through “Z” and Arabic numerals from “0” through “9” using the QR code scanning algorithm. Seven touch sensors can recognize the tactile interaction preferences of children with KiliRo robot. Sensors are attached to the robot’s wings, forehead, and body to obtain sensory information. These sensors are connected in serial to ensure touch of any sensor would enable the LED light on the robot to glow encouraging the children for more physical interaction with KiliRo.
When a number or a letter is shown to the robot, it recognizes the QR code pasted in the model and associates the corresponding text, which is then converted into speech using a text-to-speech module. Two Arduino family of microcontrollers and one Raspberry Pi 3 board were used to synthesize a range of autonomous behaviors on KiliRo including speech recognition, object recognition, real-time video transmission, text-to-speech, speaker, microphone, and locomotion gaits. Speech recognition module enabled the robot to recognize “yes” and “no” from the participants and act accordingly. This feature encouraged the participating children to have verbal communication with our robot. The speech recognition feature was used to initiate and terminate the robot’s speaking module. For instance, when “Start” was recognized, the robot started introducing itself, and when “Stop” was recognized, the robot stopped talking. A bipedal mechanism was used for synthesizing the robot locomotion. The robot’s walking motion was achieved through a pair of DC motors powered using a 2000-mAh lithium polymer battery.
For the experiments presented in this study, KiliRo’s locomotion was achieved using an android application installed on a smart phone. KiliRo’s system architecture consisting of control, actuator, sensor, module, and application is illustrated in Figure 2.
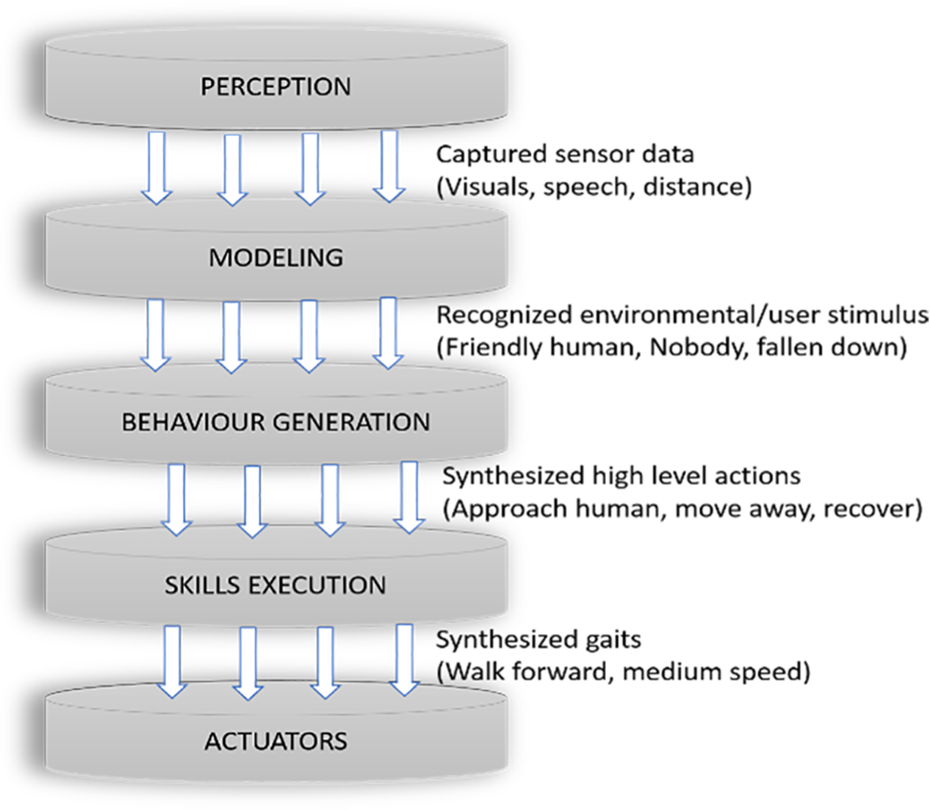
KiliRo—system architecture.
The main challenges in designing a parrot-inspired robot include the design of a parrot-like morphology, integration of sensory systems, and the nontrivial process of implementing theoretical designs generated analytically into physical mechanisms.
Study setting and participants
The study presented in this article was conducted at a single venue. More specifically, it was run at a special school for children with ASD in India.
A number of individuals assisted the research team to conduct the study. Twenty volunteers were recruited to assist with various tasks including monitoring social interactions, assessing learning, and recording physiological measures. One pediatrician and one child psychologist both with a minimum experience of 5 years were involved in the study as advisors. Two consultation sessions were organized with the pediatrician and the child psychologist for the parents of participating children on the first and last day of the study.
Study participants were recruited through invitation letters to potential participants in five pre-identified schools 3 weeks before the scheduled period for the study. Parents were given 2 weeks to respond to the invitation. A total of 52 invitations were sent to which 37 parents responded that they would be willing for their children to be involved in this experiment. A meeting was conducted with interested parents at the proposed study venue 7 days prior to the experiments, and a request was made to complete the Childhood Asperger Syndrome Test (CAST) questionnaire to identify autism behaviors in participating children. CAST involves a set of 39 “yes” or “no” questions captured in a questionnaire to evaluate autism behavior in children. 44 Children scoring 15 and above were classified to have symptoms of autism. Out of 37 children, 9 were excluded from the study due to low scores in the CAST questionnaire, and another 2 were excluded due to severe autism behavior as judged by the pediatrician and the child psychologist.
One parent informed that he was not willing to participate in the study due to logistical reasons. In addition, one parent withdrew from the experiment stating that she was traveling to her native place with her child and may not be available for the next 2 months. Finally, our experiments were conducted with 24 participants over a period of 49 days. Participating children were between 6 years and 16 years of age and had no prior exposure to robots. The mean age of participating children was 9.71 with a standard deviation (SD) of 3.24. Attendance was taken each day at the end of the study. The mean attendance rate of participants was 75.01%. Consent from parents was obtained before involving their children in the study. Parents were informed that they may withdraw from participation at any time without any compensation, and safety precautions taken were explained in detail. This study had approval by the authors’ institutions ethics committee.
Procedure
Children were exposed to the robot for a minimum duration of 60 min each day over 49 days. Participants were allowed to interact and carry the robot freely. This study was performed with no compulsory attendance requirements for the participants. Nevertheless, the researcher and volunteers were present every day throughout the study adhering to the maximum working hours as instructed by employment rights in New Zealand and India. Four sessions were conducted each day with a minimum of 15 min per session. During the first session, the robot was placed on a table with the dimension of 3 × 3 ft2. The participants were allowed to have an open interaction with the KiliRo robot. The second and third sessions involved activities around learning abilities of the robot. Letters of the alphabet and numbers were shown to the robot, and its ability to recognize them was demonstrated in front of participating children.
Our KiliRo robot uses the QR codes on each of the cards shown to identify letters of the alphabet and numbers. We expected the participating children to believe that the robot is answering the questions on the alphabet and the numbers autonomously as in the case of trained real parrots. During the fourth session, the robot was operated to move forward and backward while talking to the participants about its capabilities. The participating group was randomly divided into two. Group I consisted of 10 participants with a mean age of 10.50 (SD = 3.66) and was considered for investigating improvements in social interaction, learning, and psychological changes. Group II consisted of 14 participants with a mean age of 9.71 (SD = 3.24) and were considered for investigating the physiological changes in participating children before, during, and after interacting with our KiliRo robot.
Social interaction and learning
Manual observation method was utilized to evaluate the improvements in social interaction and learning of participating children. For this purpose, five volunteers were allocated to monitor the improvements in social interaction and learning of participating children during the sessions with our KiliRo robot. Each volunteer was allocated to two participants to ensure the accuracy in monitoring and reporting their observations regarding participants’ social interaction. They also commented on the participants’ motivation toward learning at the end of the study by monitoring their interaction in the session, while the robot’s ability to recognize alphabets and numbers was exhibited. The volunteers were advised to maintain a structured record to manually enter the data on participants’ social interaction on a daily basis such as number of attempts to speak with the robot and peers. Figure 3 shows examples of the participants’ interactions with our KiliRo robot during the study.

Participants interacting with KiliRo.
Social network density
It is reported that identifying the network density can help determine the improvements in interaction among participants. 15 In our study, social network density (SND) analysis was chosen as a method to illustrate social interaction among participants, as it is able to provide detailed information on social interaction such as which participant interacted with whom. In this study, interaction is defined as looking, smiling or laughing, holding hands, touching, initiating verbal or nonverbal communication, hugging, petting, stroking at other participants or robot, and offering the robot to other participants.
On the first day of the study, all 10 participants from group I were gathered in a single room with the area of approximately 18.5 m2. The participants were monitored for 60 min, and their number of attempts to interact with others were recorded before interaction with the robot. An interaction was recorded if a participant exhibited more than six successful attempts to interact with another participant through any of the above defined means of interaction.
The same data were collected during the last week of the study, but with the robot. That is, this time the robot was also placed in the room at a table with other participants, and interaction of children with other participants and with the robot was monitored.
In our social network diagram, nodes S1 through S10 represent participants and node KiliRo represents the robot. The connection between the participants or robot denotes an interaction. SND before interaction with the robot is illustrated in Figure 4.
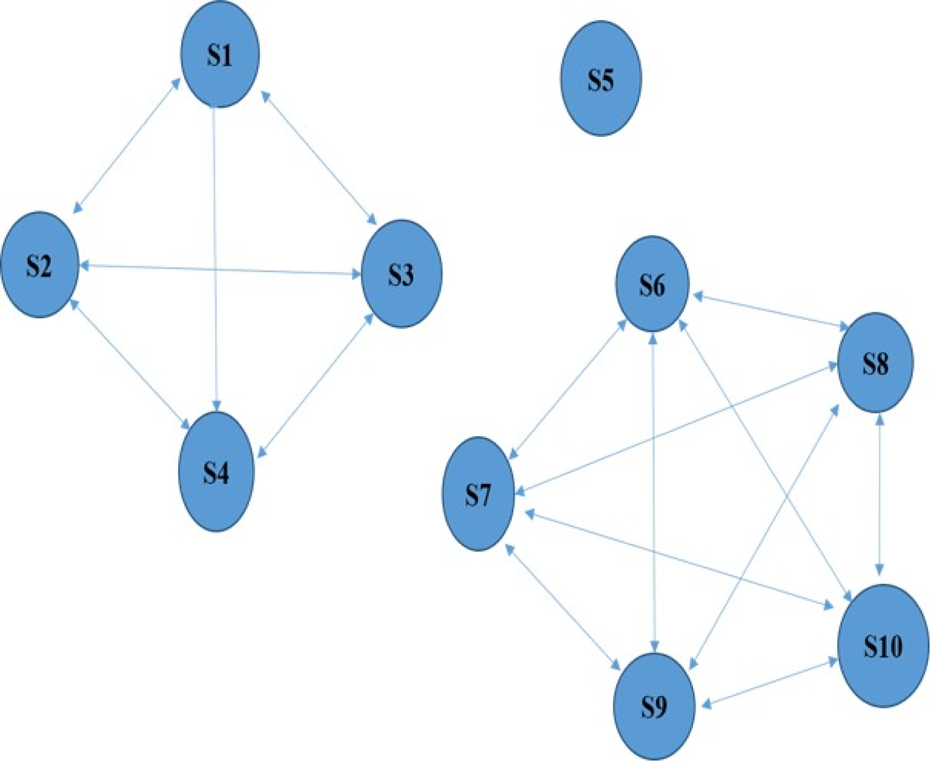
SND before interacting with the robot. As can be seen here, S5 did not interact with any other participant, and there were two groups of participants who interacted with each other. SND: social network density.
Participants S1, S2, S3, and S4 were from the same school and knew each other prior to this study. Similarly, participants S6, S7, S8, S9, and S10 were from the same school and knew each other. Participant S5 was from a different school and did not know any of the participants before the study was performed. Figure 5 illustrates the social network diagram of participants during the last week of our study after interacting with the robot.

SND after interacting with the robot. As can be seen here, participants interacted both with KiliRo and with each other. There was no participant who did not interact with anyone. SND: social network density.
Network density is calculated as

where potential connection (PC) is the maximum number of connections that could potentially exist between all nodes in the network, whereas actual connections (ACs) are the ones that were actually observed between the nodes.
PC is calculated as

where n is the total number of nodes in the network.
SND before interacting with the robot was compared with the SND after having been introduced to KiliRo as below.
SND before interacting with the robot is


Using equation (1)

SND before interacting with the robot


Using equation (1)

Learning
Inclusion and exclusion criteria were applied for considering the participants in our study that involved evaluating their learning while interacting with KiliRo. A simple task of identifying letters of the alphabet (“A” to “G”) and Arabic numerals from “1” to “7” was used as inclusion and exclusion criteria. Participants who were able to identify at least 6 of 14 items were excluded from our experimental study. Participants, S1, S4, S5, S6, S8, and S10, were thus excluded from this session of the study. Results of improvements in learning in terms of identifying the total number of alphabets and numbers after interaction with KiliRo were investigated. Before performing the study, participants, S2, S3, S7, and S9, were able to identify in total two, one, zero, and three items from the considered set of characters and numbers, respectively. During this study, our KiliRo robot exhibited its ability in recognizing the alphabets and number in front of the participating children. The study was performed for the duration of at least 30 min in two sessions.
Physiological analysis
Literature points to noninvasive methods for assessing human psychological and social behavioral processes as a highly convenient and effective approach in many clinical settings. Particularly, these methods are found to be very useful in research studies involving special-needs children. For instance, Wada and Shibata investigated the 17-KS-S and 17-OHCS hormone levels in elderly using urinary samples to evaluate the stress level in elderly while interacting with a seal-like robot. 15 However, there are other hormones in the human body whose proportional relationships to psychological changes are better quantified. It is identified that higher protein levels in urinary sample may indicate higher stress levels in subjects. 45 Previous studies have reported that a person’s α-amylase level generally increases during stressful situations. 46 Sympathoadrenal medullary activity is examined in α-amylase test and increased α-amylase levels serve as an indicator of increased stress levels. 47 For our studies presented in this article, we used urinary and salivary tests to evaluate the biological changes in children with autism before and after interacting with our parrot-inspired robot, KiliRo. This is a pioneering human robot interaction study that uses salivary test for validating the effects of robotic engagement with autistic children. Urinary sample was used to measure protein levels in participating children, and salivary sample was used to measure the α-amylase levels. Urinary and salivary samples of participating children were collected by their parents and were handed over to the laboratory technician on the first day of the study, before introducing our KiliRo robot. The first samples were collected on the first day of the study before the participants have interacted with the robot, while the second samples were collected during the last week of the study to evaluate the changes in stress levels after interacting with KiliRo robot for over 7 weeks. Both the urinary and salivary samples were taken at the study venue between 9 a.m. and 11 a.m. We involved seven participants from group I with the mean age of 10.0 and SD of 3.51 for conducting urinary and salivary tests due to various reasons including possibility in collecting urinary and salivary samples and parents’ consent. To protect the identity of participating children, the samples were labeled as subject 1 through subject 7.
Investigating the diastolic (DIA) and systolic (SYS) blood pressure, heart rate (HR), and oxygen saturation level in blood (SPO2) aids in monitoring the changes in vital signs in a human body. 48 The human body produces a surge of hormones during stressful situations, thus increasing the blood pressure through an increase in HR. By investigating these physiological measures, we propose to assess the physiological effects of using our KiliRo robot in children with autism. We also investigated the participants’ oxygen saturation levels carried by hemoglobin to monitor the effects of robot-assisted activity. In this study, we investigated the changes in vital signs among participating children before, during, and after interaction with the KiliRo robot. For this investigation, we involved 14 participants from group II (mean age of 9.71 and SD of 3.24). The tests were performed seven times during the entire study, and the mean value was calculated to report changes in children’s vital signs. Fourteen volunteers were allocated for taking DIA and SYS blood pressure, HR, and SPO2 measurements before, during, and after interacting with KiliRo. The volunteers were given training by experts for performing and recording the values of these tests. The study was overlooked by a pediatrician and a child psychologist. The readings were taken using commercially available measuring devices such as OMRON (Omron Healthcare) blood pressure monitor.
Results
Improvements in social interaction
According to the SND, participants’ social interactions before and after exposure to KiliRo increased from 0.36 to 0.60. This may indicate that the interaction with KiliRo robot motivated participants to engage in interactions. As an illustration, participants S1, S2, S3, and S4 did not interact with any other participants before introducing the robot. But after introducing KiliRo, it is noted that most of them established interaction with other participants. It was also noted that participants identified seemingly like-minded people in the group and initiated interactions. For instance, participant S2 and S7 exhibited interest to hold the robot. When the researcher gave the robot to one participant, the other came nearby and was smiling at the other participant.
From observations and reporting from volunteers involved, it was found that all participants except S4 and S5 created a strong bond with our parrot-inspired robot by talking, playing, and hugging among other participants. It was noted that particularly participant S10 developed a very strong bond with our robot by talking to it very often. He also hugged the robot many times and asked the robot to talk. He was highly interested in the first session of our study in which the participants were allowed to freely interact with the robot as opposed to other sessions that involved learning. Most of the time, he was the first person to go near the robot and start talking. Moreover, he also carried the robot to other participants engaging in interactions with them that revolved around KiliRo. Reports from volunteers also indicated that participant S5 was not very keen to interact with KiliRo during the first 3 weeks of our study. Nevertheless, it was found that his interest toward the robot increased during the last 4 weeks of our study. Similarly, participants S3 and S8 showed minimal interest to interact with the robot initially, which improved during the last 3 and 2 weeks of the study, respectively.
Social interaction among participating children was evaluated using the first session of our study that lasted for 15 min each day over a period of 49 days. The time spent on interacting with our KiliRo robot by participants varied from one participant to another. The average time spent during each week, total time spent throughout the study, and average interaction time of each participant during the study are illustrated in Table 1.
Participants’ interaction time (minutes) with the robot.

Learning of letters and numbers
Our study reported notable learning improvements in children with autism using KiliRo robot. All four participants included in this study showed positive results in learning. Specifically, the participant S7 showed notable improvement in letter and number recognition from 0 to 4. She was not able to identify any alphabet or number before the study. But, at the end of the study, she identified three alphabets and one number correctly. Interestingly, she showed the alphabet “A” to the robot on the 17th day of the experiment and started saying “Aaaaaaaaaa” as an attempt in teaching the character to KiliRo. At the end of our trials with KiliRo, the participants, S2, S3, and S9, identified five, three, and five items, respectively, thus showing some evidence of substantial learning. Figure 6 illustrates the participants’ letter and number recognition scores before and after interaction with the robot.
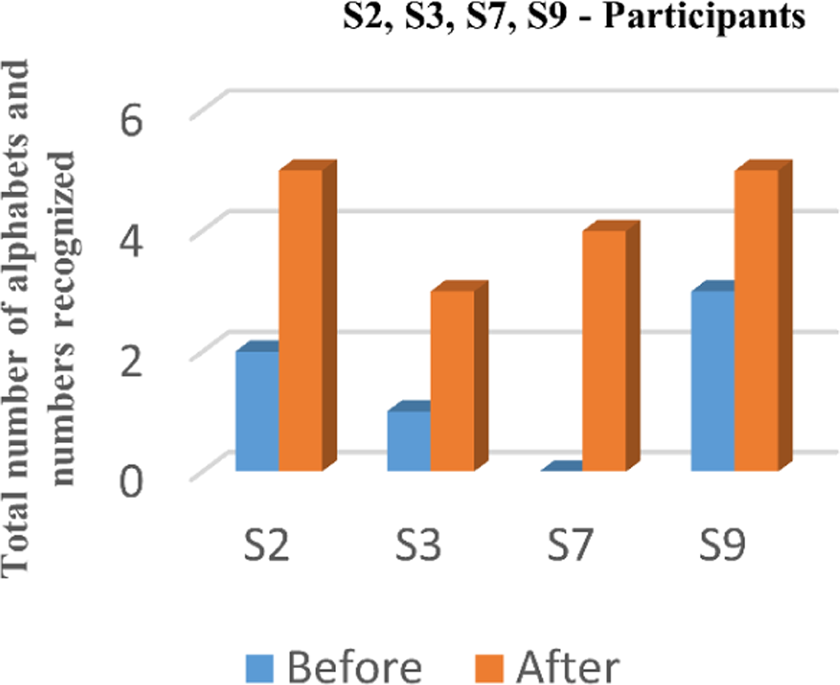
Letter and number recognition scores before and after interacting with the robot.
Results of the physiological analyses
Table 2 shows the protein and α-amylase levels of participants before and after interacting with the robot.
Urinary and salivary test results.

In our trials, we observed that the mean protein level of participating children dropped from 40.31 to 17.40 after interacting with our KiliRo robot. These changes were statistically significant according to a nonparametric-related-samples Wilcoxon signed-rank test (z = −2.37, p < 0.05). The obtained results clearly demonstrate the potential of our developed KiliRo robot in lowering the stress level of children with autism through close human robot interactions.
It is also noted that the α-amylase levels have reduced in the second sample test report, from a mean of 305.71 to 151.29. Despite the fact that the level for participant 5 increased at the second time point, the overall reduction in the α-amylase levels of the group was statistically significant (related-samples Wilcoxon signed-rank test, z = −2.20, p < 0.05).
Physiological analysis
The average results of SYS, DIA, HR, and SPO2 data entered by the volunteers are shown in Table 3. The average results of the complete study were considered for evaluating the physiological effects of using KiliRo, and no readings were excluded.
Blood pressure, heart rate and oxygen level in blood.

HR: heart rate; SPO2: oxygen saturation level in blood.
Results from the notes taken by the volunteers show that there was no notable change in DIA and SYS blood pressure, HR, and SPO2 of participants before, during, and after interaction with the robot, except for a few cases. For instance, in SYS blood pressure readings, one participant recorded more than 120 before interaction, four participants during interaction, and two after interaction. For all measures (SYS, DIA, HR, and SPO2), mean values before, during, and after interactions were virtually unchanged (Table 3). Hence, we conclude that the interaction with KiliRo robot did not have notable change in blood pressure, HR and SPO2.
Conclusions
We have developed a parrot-inspired robot, KiliRo, and validated the merits of our robot in improving learning and social interaction abilities, reducing stress levels, and improving physiological conditions with a group of 24 children identified with autism over a period of 49 days. This study demonstrated that the interaction with our KiliRo robot can help improve learning and social interaction abilities of children with autism. We investigated the changes in stress levels of participating children after interacting with the robot through urinary and salivary tests. This is the first time in human–robot interaction study to use salivary samples investigating changes in stress levels. The urinary and salivary test reports from our study indicated reduction in stress levels among the participants after interacting with our KiliRo robot. The physiological changes were measured using SYS and DIA blood pressure, HR, and oxygen saturation levels and reported no notable change in readings before, during, and after interacting with the robot.
This study has several limitations. Although the results show improvements in social interaction, learning, and stress reduction, the study did not have a control group to compare the results with. Leaning was evaluated using a small sample size and may not be generalized. Even though protein and α-amylase levels indicate reduction in stress levels of participants after interacting with the robot, several other factors that may have influenced these chemical substances such as medication, body temperature, personal, or cultural activity, and time that the sample was taken. Additionally, the sample size was too low to generalize the findings of the study. Hence, the results of the study should be viewed carefully, and replication with a larger sample and control group is needed. However, the results of our pilot study indicate that the study is worth replicating with a larger sample and a control group, a larger variety of appropriate biomarkers, and tighter control of potential extraneous variables. The limited sample size of the study also did not permit more detailed analyses of the benefits of robot therapy for specific aspects of ASD 49 including gender differences, 50 and future studies may explore which children could benefit most from these types of interventions. Another possibility for future work is to conduct a study with longer duration over several months. The third area of our interest is to build on our present work and run cross-country studies at three different locations, such as India, Singapore, and New Zealand. Finally, we intend to extent the autonomous and locomotion capabilities of our KiliRo robot with increased autonomous functions.
Footnotes
Acknowledgements
The authors thankfully acknowledge the support from Dr Prem Kumar, Pediatrician, Mehta Hospitals, India, and Mrs Priya Govarthana, Chief Child psychiatrist, Govt. Women & Children’s Hospital, India. The authors are also immensely thankful to children participated in the study, their parents, volunteers from Bharath University, India, Anna Adharsh College for Women, India, Volgograd State Medical University, Russia, and Mrs Thillai Subramaniam, Head of School where the study was conducted. The funding is gratefully acknowledged.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is supported by the Institute of Biomedical Technologies, Auckland University of Technology, New Zealand, and SUTD-MIT International Design Center, Singapore University of Technology and Design, Singapore.