
Abstract
Background
As an elevated D-dimer level is directly proportional to the degrees of trauma and coagulation, it is often used to assess the severity of the trauma as well as the risk of thrombosis. This study aimed to investigate the risk factors for a high postoperative D-dimer level.
Methods
A total of 623 patients undergoing radical mastectomy were included. The association between various clinicopathological factors and D-dimer variation was examined.
Results
Age, neoadjuvant chemotherapy, diabetes, and elevated neutrophil count were significant risk factors for D-dimer variation, after adjusting for other factors.
Conclusions
This study has identified the characteristics of patients who are likely to experience considerable postoperative increases in the D-dimer level. The development of effective nursing interventions for these patients is the focus of future studies.
Background
The incidence of breast cancer in China has increased due to the popularity of early screening modalities; however, breast cancer prognosis has also improved owing to advances in treatment techniques.1–3 Concurrently, the long-term survival of patients highlights the need for improving postoperative quality of life.4–6 Surgery remains the most important modality in the comprehensive treatment for breast cancer.7,8 A smaller surgical trauma can effectively reduce the risk of surgical complications and enhance the patient’s quality of life. With the current trend of reducing the surgical extent, several hospitals have steadily increased the proportion of breast-conserving surgery, thereby leading to a continuous decrease in the scope of surgery.9–11 The reduced extent of injury is associated with several benefits, including lower surgical complications, faster recovery rate, and even long-term survival. However, with the introduction of the Enhanced Recovery After Surgery (ERAS) concept, an increasing number of breast cancer patients have chosen to prolong postoperative bed rest.12–14 Although this can substantially reduce the duration of drainage tube placement, it also increases the risk of venous thrombosis. Therefore, postoperative nursing care for patients with breast cancer is now facing several emerging challenges. A comprehensive analysis of the patient’s clinicopathological characteristics and surgical approach is required to assess the degree of trauma and the risk of thrombosis.
Breast-conserving surgery has the advantages of less trauma, less bleeding, lower postoperative pain, faster recovery, and better cosmetic outcomes compared with conventional total mastectomy/glandectomy. However, due to a long waiting time for pathology, breast-conserving surgery has no significant advantages with respect to operation time. In addition, several influencing factors of surgery have introduced multiple concerns over the assessment of patient status during nursing care. A comprehensive analysis of these influencing factors, which include surgical approach and operation time, is therefore required to provide an assessment of the patient’s degree of trauma and the risk of thrombosis.
To maintain a normal physiological state, the clotting system is activated to prevent blood loss in the case of vascular damage. Although unspecific, an increased D-dimer level is a relatively sensitive biomarker for the formation of thrombosis in the circulatory system.15–17 Therefore, it is often clinically used to aid in the diagnosis of venous thromboembolism (VTE), deep vein thrombosis (DVT), and pulmonary embolism (PE). In addition, the D-dimer level has been confirmed to be directly associated with the degree of trauma, making it an appropriate indicator for the assessment of the severity of injury.18,19 As an important component of the fibrinolytic system, D-dimer is significant for the diagnosis and treatment of thrombus, tumor, and other diseases.20–24 It is a key indicator of DVT, PE, and diffuse intravascular coagulation; it can also be used to evaluate wound severity.25,26 Therefore, in this study, we focused on D-dimer in the formation of thrombosis and injury before and after breast cancer surgery. We aimed to explore the independent risk factors of increased D-dimer levels in the postoperative period and the influencing factors for the degree of trauma and the risk of thrombosis, to provide a basis for identifying patients who will require close monitoring.
Methods
Patients
This study enrolled 623 patients who underwent any of four types of radical mastectomy at the Second Hospital of Dalian Medical University: total mastectomy (glandectomy), breast-conserving surgery, sentinel lymph node biopsy, or axillary lymph node dissection. All patients had complete medical records. Clinical, surgical, and pathological findings and all medical data were collected and recorded in the database.
This study was approved by the Ethics Committee of Second Hospital of Dalian Medical University. All methods were performed in accordance with the relevant guidelines and regulations. Informed consent was obtained from all participants.
Blood sampling
Blood samples for the determination of pre- and postoperative D-dimer levels were acquired together with the samples used for other hematological tests. Preoperative sampling was usually performed on the second day after admission, approximately 3 days before surgery. Alternatively, postoperative sampling was usually performed 1 day after surgery.
Statistical analyses
The chi-square test was used to analyze the balance between groups of various D-dimer levels, and a correlation analysis was used to identify the influencing factors of D-dimer levels. Multivariate analyses using the ENTER method were conducted to assess the risk factors of increased D-dimer levels. All analyses were performed using SPSS software, version 23.0. Two-sided P values of <0.05 were considered statistically significant.
Results
Patient characteristics
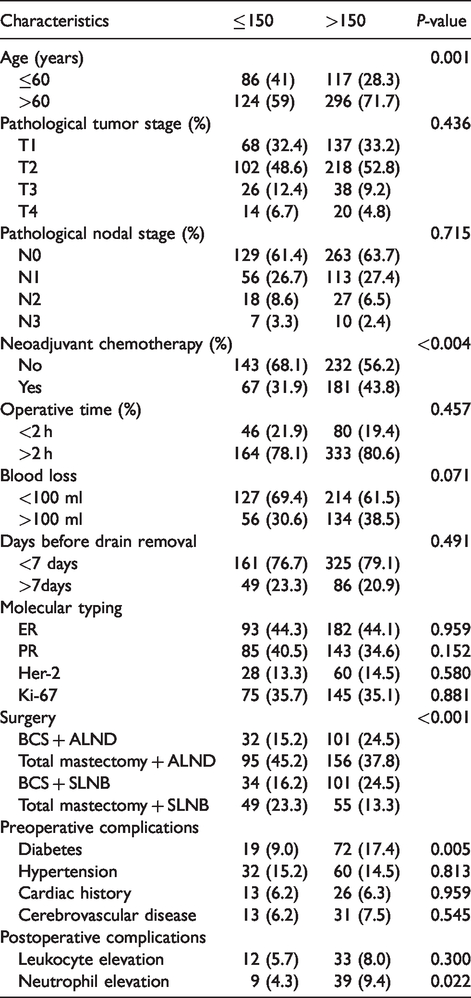
A total of 11 clinicopathological factors were identified and included in the analysis. The distributions of various clinicopathological factors were subsequently compared between the two groups. Of these, age, neoadjuvant chemotherapy, surgery, diabetes, and neutrophil elevation were significantly different between the two D-dimer groups (Table 1). Factors with significantly different distributions between the two groups were identified as possible risk factors for D-dimer variation.
Characteristics of population by D-dimer increase level (n = 623).
Correlation analysis
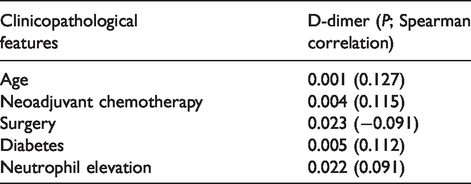
Spearman correlation analysis showed that the D-dimer difference had a linear correlation with age, neoadjuvant chemotherapy, surgery, diabetes, and neutrophil elevation (Table 2).
Spearman correlation analysis between clinicopathological features and D-dimer.
Risk factor analysis
The association between the possible risk factors and elevated D-dimer level is shown in Table 3. After adjusting for the 17 variables, age, neoadjuvant chemotherapy, diabetes, and neutrophil elevation were found to be significant risk factors.
OR for the increase of D-dimer—multivariable analysis (n = 623).
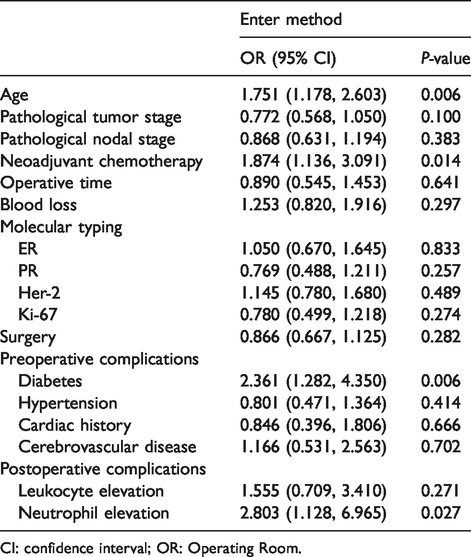
CI: confidence interval; OR: Operating Room.
Discussion
The concept of ERAS has received increasing attention in recent years. ERAS is aimed to provide postoperative patients with multiple comprehensive treatment approaches for rapid recovery, and thus it can reduce psychological and organic/structural traumatic stress responses, ultimately lowering postoperative complications, shortening the average length of hospital stay, decreasing the risk of death, and lowering medical costs.27–29 However, ERAS is yet to reach its optimal stage, and it is still under development. Particularly, in China, specific diagnostic and therapeutic measures need to be modified to make them more specific for the Chinese population. Accordingly, continuous collecting of clinicopathological data, surgical information, postoperative complications, prognosis, and follow-up information of patients undergoing surgery—and combining them with statistical analysis—is needed to develop more reliable, effective diagnostic and treatment modalities specific to the Chinese population.
We found that age, neoadjuvant chemotherapy, diabetes, and elevated neutrophil count were significant risk factors. The older the age, the higher the risk of concurrent thrombosis and the weaker the body’s ability to recover from surgical traumas. This is why older patients should be closely monitored for the possibility of postoperative VTE. The clinical value of D-dimer has increased due to the increasing number of patients selecting neoadjuvant chemotherapy.
Diabetes is a known risk factor for thrombosis. In particular, physiologic changes after general anesthesia often lead to high blood sugar levels; combined with a prolonged time in bed, the risk of thrombosis is increased, requiring attentive monitoring of patients. Postoperative infection, particularly cell infection that leads to elevated neutrophil count, is not only a risk factor for thrombosis, but also aggravates injury. Concurrently, infection also results in an elevated D-dimer level. Although the extent in D-dimer level increase is not necessarily associated with the risk of thrombosis and the degree of body injury, preventive measures should still be implemented for postoperative infections, such as drainage-tube-related infections, wound infection, and urinary tract infection.
D-dimer can, to some extent, represent the degree of body injury. However, although breast-conserving surgery and sentinel lymph node biopsy are less invasive, there was no significant difference in postoperative D-dimer levels between these and the other two types of surgery. Consequently, the different methods of surgery cannot serve as an independent factor for the D-dimer level. This is possibly because of the confounding bias between the four surgical approaches or the extended operation time and intraoperative pathology waiting time of breast-conserving surgery and sentinel lymph node biopsy. In addition, operation time was not an independent component due to various confounding factors. Lastly, factors such as tumor node metastasis stage and molecular type of the disease are not directly associated with an increased postoperative D-dimer level.
Our study has limitations. We did not have a deep venous system Doppler USG for every patient on different postoperative days after surgery. This is a retrospective study. All the patients scheduled to undergo surgery in our hospital were examined for the risk of DVT before surgery. Surgery was performed only when that risk was low. After surgery, we continued to monitor D-dimer levels and other indicators, and observed the patients for symptoms of DVT. When the risk of DVT was considered to be high, the deep venous system Doppler USG was performed. At the same time, we also considered the shortage of medical resources and insufficient finance. Therefore, not every patient included in the study completed the test.
Infections and other postoperative complications may influence D-dimer levels. C-reactive protein (CRP), the total number of leukocytes, and other indicators not only provide information on the degree of damage but also help to determine the extent of the influence of infection and other factors on D-dimer levels. Routine preoperative examination for CRP was not performed due to high medical expenses. CRP was not monitored in patients without postoperative symptoms. Here, we analyzed the leukocytes and neutrophils in the blood routine before and after the operation to determine whether there was any possibility of infection that could influence D-dimer levels after surgery. In the future, we will strive to carry out relevant clinical trials. Additionally, Operating room time and volume of blood loss indicate a learning curve. We analyzed the operation time and volume of blood loss over different years, and both had a decreasing trend, which indirectly reflected the learning curve of surgeons for thoracoscopic surgery.
A high postoperative D-dimer level potentially corresponds to a more severe body injury and a higher risk of thrombosis after surgery. Further, our findings also indicate that despite advances in diagnosis and treatment, the collection of data—such as the patient’s basic information and previous treatment record—together with the prevention and treatment of perioperative complications, will always remain important.
Conclusions
This study has identified the characteristics of patients who are likely to experience considerable postoperative increases in the D-dimer level. The development of effective nursing interventions for these patients is the focus of future studies.
Footnotes
Acknowledgments
Not applicable.
Availability of data and material
The datasets analyzed during the present study are available from the corresponding author on reasonable request.
Authors’ contributions
LQ and YW participated in designing the study and drafting the manuscript. LQ participated in the statistical analysis and drafting of the manuscript. All authors read and approved the final manuscript.
Consent to publish
Not applicable.
Declarations of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Second Hospital of Dalian Medical University. All the patients provided written informed consent.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Dalian Medical Science Research Project (1612023).