
Abstract
Liquid biopsy is routinely used to detect epidermal growth factor receptor mutations in advanced or metastatic lung cancer, due to some limitations of tissue genotyping, especially at relapse. However, the existence of a non-marginal proportion of oncogene-addicted lung cancers that can benefit from target therapy is rapidly expanding clinical relevance of plasma genotyping. Apart from static assessment of mutations in circulating free DNA, the fact that liquid biopsy is minimally invasive and can be repeated several times makes it a suitable assay for the dynamic monitoring of cancer response to treatment. It is likely that quantitative mutation assessment by liquid biopsy will be increasingly included in the design of innovative clinical trials for patient stratification purposes.
Keywords
Lung cancer is the most common cancer worldwide and is the leading cause of cancer-related mortality. 1 The last decade has seen considerable progress in the field of systemic and molecular characterization of non-small-cell lung cancer (NSCLC), the prevalent type of lung cancer, accounting for >80% of all lung cancer cases. The discovery of oncogenic driver mutations and the concept of oncogene addiction modified the therapeutic approach for patients with advanced NSCLC. 2 Specifically, identification of activating mutations in the epidermal growth factor receptor (EGFR) gene in approximately 15% of patients introduced the era of targeted therapy in advanced NSCLC, shifting treatment paradigms from platinum-based chemotherapy to tyrosine kinase inhibitors (TKIs) to manage tumor progression and metastatic disease. 3 Other potential therapeutic targets, including rearrangements involving ALK, ROS1, or RET, and mutations of BRAF, ERBB2, and MET have been identified in lung adenocarcinoma, although their incidence is typically low (range 1%–5%). 4 In contrast, other genes including TP53 and KRAS, whose mutations are among the most prevalent alterations in NSCLC (detected in 40%–50% and 25%–35% of patients, respectively), remain currently orphan of targeted therapies. 5
As biopsy specimens can be inadequate for routine tissue genotyping, or tumor location can be inaccessible, 6 circulating free DNA (cfDNA) analysis—also referred to as liquid biopsy—has emerged as a new tool for detecting clinically relevant genetic alterations in lung cancer patients. The term “liquid biopsy” is commonly used not only to refer to molecular assays performed on cfDNA purified from plasma but also can include testing on other body fluids, such as urine and cerebrospinal fluid, and measurements of circulating tumor cells, exosomes, circulating tumor RNA as well as cfDNA. As the description of these applications exceeds the aims of this opinion article, the reader is referred to excellent comprehensive reviews recently published on this topic.7-9 In the case of advanced NSCLC, plasma genotyping is the most common application of liquid biopsy, and it is now widely used both as a diagnostic assay to investigate EGFR sensitizing mutations at baseline and to detect the acquired resistance EGFR T790M mutation at disease progression when tumor tissue is not accessible. 10 According to a recent meta-analysis, 11 the average sensitivity of EGFR liquid biopsy by using routine CE IVD-approved quantitative polymerase chain reaction (qPCR) methods is 65%–70%, although real-world studies have shown that the performance of cfDNA testing varies significantly among laboratories. 12 We recently conducted a monocentric study that investigated the ability to detect in plasma of 101 advanced NSCLC patients EGFR mutations previously identified in matched tumor tissue biopsy. We found that using targeted PCR-based methods, the detection sensitivity was 56%, a result substantially in line with literature data (manuscript in preparation). Although international guidelines recommend tissue re-biopsy for molecular characterization at relapse when liquid biopsy is non-informative, in many cases the poor physical condition of the patient does not allow this. In these cases, repeating the liquid biopsy can be considered as this can enable the detection of a previously missed p.T790M mutation, which is of potential benefit to the patient because it makes it possible to prescribe the third-generation EGFR-TKI osimertinib, which is a highly active drug against the tumors bearing this particular mutation. 13 The optimal timing to repeat liquid biopsy has not been established, although in our experience a 3- to 4-month interval between two independent tests should be considered.
Apart from this canonical use of liquid biopsy, new applications have been reported and it is likely that some of them will become daily practice in the next 3–5 years. One upcoming application regards genetic testing for additional actionable targets in NSCLC. These targets include mutations in BRAF, ERBB2 and MET as well as genetic alterations in ALK, ROS1, RET, and—more recently—neurotrophic receptor tyrosine kinases (NTRKs). Although is it clear that assessment of the genetic status of these genes on tissue represents the gold standard, a proportion of patients’ DNA obtained from tissue biopsy is not enough to perform these additional molecular tests, especially if a routine diagnostic is performed through a single gene rather than multiplex testing. For these patients, next-generation sequencing (NGS) of cfDNA prior to systemic therapy could be suggested. Clearly, this will require reorganization of laboratory workflows in order to make it possible to release NGS-based clinical reports within a clinically useful time frame (generally 2 weeks) compatible with therapeutic decisions. Moreover, liquid biopsy should be proposed straight away by the pathologist after histologic examination in those cases where the amount of tumor is likely inadequate for genotyping, to prevent delays in the administration of systemic therapy. Finally, there is also an economic issue, as such an NGS-based screening would add €1000–2000 cost per patient—depending on the complexity of the panel and the sequencing depth—which will represent an additional charge for the public health insurance system.
A second clinical application of liquid biopsy is the detection of resistance mutations associated with treatment with ALK inhibitors. ALK rearrangements and resistance mutations can be identified through cfDNA analysis. In a recent study, plasma genotyping identified an ALK fusion in 86% of patients, and an ALK inhibitor resistance mutation in 50% of patients, with high concordance between plasma and matched tissue genotyping. 14 Furthermore, the identification of certain resistance mutations including p.G1202R, p.F1174C, and p.L1196M plays an important role in treatment selection for ALK+ patients at progression 15 ; these alterations can be identified through liquid biopsy when re-biopsy is considered not feasible or safe.
Finally, although plasma genotyping so far has mainly been exploited to detect certain clinically relevant actionable mutations, there is a conceptually different exploitation of liquid biopsy that will, in my opinion, become increasingly important in the coming years. The fact that liquid biopsy is minimally invasive and can be repeated several times makes it a suitable assay for dynamic monitoring of cancer response to treatment. There are already examples in EGFR-mutated NSCLC patients treated with first-generation EGFR-TKI. The clearance of an EGFR mutation in cfDNA occurred at week 8 of gefitinib treatment in 88% of informative blood samples, with overall survival found to be superior in patients who exhibited EGFR mutation cfDNA clearance compared to those with persistence of the mutation in plasma. 16 In future studies, additional “sentinel mutations,” defined as driver gene mutations whose abundance can be measured in cfDNA by molecular techniques (e.g. such as TP53 and KRAS mutations) will be increasingly used to evaluate the response to systemic therapy. Along these lines, we found that monitoring the abundance of KRAS mutations in plasma by droplet digital PCR at early timepoints after administration of systemic therapy (including chemotherapy or immunotherapy) provides important predictive cues (manuscript under revision). I consider it likely that in the next 3–5 years dynamic measurements of the abundance of specific cancer-associated mutations in cfDNA will become a routine assay, and the outcome of such measurements will be used to stratify patients who need standard or intensified therapy, as shown in the hypothetical model presented in Figure 1. Several other biomarkers, such as variant allele fraction determination, variations of cfDNA during treatment, or hypermutated cfDNA, have been evaluated as potential predictive biomarkers to evaluate the response to immunotherapy in cancer patients. 17 , 18 Although the real significance of liquid biopsy in patient outcomes compared with patient management guided via canonical molecular data and imaging modalities remains to be addressed, the roadmap is well defined, and upcoming years will see exciting developments in this field.
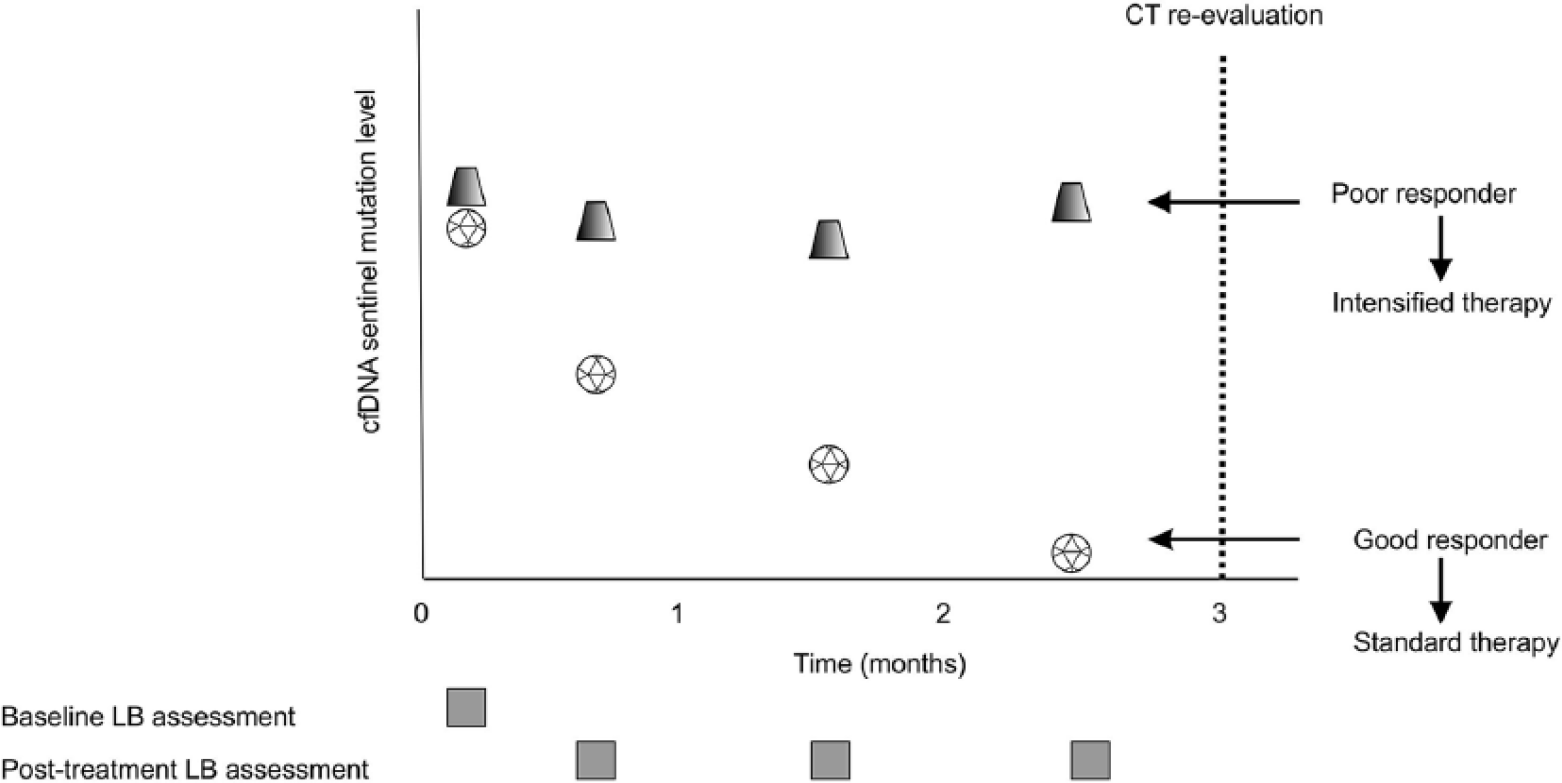
Dynamic monitoring of cancer response to systemic therapy by liquid biopsy.