
Abstract
The discovery of molecular alterations that play key functions in pathways of tumor growth and survival have changed the treatment approach of several solid tumors. A number of biomarkers are now approved in clinical practice for the selection of patients to be treated with the specific targeted drug, and others are currently under study. None of these biomarkers are perfect and they have a number of biases. Novel treatment approaches, such as immunotherapy, require the development of more complex biomarker combinations as the mechanism of action of these drugs involves multiple parameters. In this short communication the principal approved biomarkers in solid tumors are discussed, with attention to the novel promising biomarkers that will be developed in the future.
Keywords
Introduction
The identification of molecular aberrations in key components of signal transduction pathways involved in tumor growth and survival—so-called oncogene-addicted tumors—has dramatically changed the treatment approach of a number of solid tumors. However, patients with malignancies of the same organ respond very differently to a specific drug, with the response rate in unselected patients that could vary from less than 10% to more than 90%. Many of the newer biological or molecular therapies have efficacy in only a minority of unselected patients, and have high costs. These aspects highlight the need of predictive biomarkers able to select patients and to personalize treatments. Until now, a number of biomarkers have been approved in clinical practice, and a series of companion and complementary diagnostic assays are available in specific tumor types for treatment decision making. 1 These biomarkers are often represented by DNA alterations, which are easily determinable with methodologies relatively simple to be standardized among different laboratories. However, novel therapeutic strategies, such as immunotherapy or anti-angiogenic treatment, are turning out to be more difficult to personalize than expected, thus making it harder to identify predictive biomarkers for these types of treatment.
Approved biomarkers in solid tumors
The epidermal growth factor receptor (EGFR) history in non-small-cell lung cancer (NSCLC) was among the first evidence that the selection of patients based on the right marker could lead to significant increased efficacy of targeted agents. EGFR-tyrosine-kinase inhibitors have changed the natural history of NSCLC for those patients carrying the specific EGFR mutation and are now the standard of care for these patients. 2 The same story was regarding anti-ALK agents, which are now approved in clinical practice for the treatment of ALK and ROS1 rearranged NSCLC patients. 3 Other emerging targeted agents directed against other molecular alterations (i.e., BRAF, HER2, MET, RET, etc.) are under study.4,5 Similarly, in other solid tumors, a series of targeted agents usable only in patients carrying specific alterations are now available in clinical practice. BRAF mutation in melanoma—found in about 50% of patients—induces sensitivity to anti-BRAF agents such as dabrafenib and vemurafenib. More recently, the “synthetic lethality” concept, which targets two DNA repair pathways and induces serious cytotoxicity to tumor cells without damaging normal cells, is used for the use of poly (ADP-ribose) polymerase inhibitors in BRCA defective tumors, such as ovarian and, more recently, pancreatic cancer. 6 Other examples of targeted agents directed against driver alterations is that of anti-HER2 drugs, which are active in tumors with HER2 amplification, breast and gastric cancer, 7 or tumors with HER2 mutation (lung cancer). 5
One way to select patients is to exclude those with a high probability of being resistant to a treatment, with the search of resistance biomarkers. This is the case in colorectal cancer, for which patients with a RAS mutation are excluded from treatment with anti-EGFR mAb, as they represent a demonstrated primary resistance mechanism. 8
As molecular characteristics of a tumor are dynamic over the course of cancer progression and treatment, alterations responsible for acquired drug resistance also could be a target of treatment. A well-characterized example of this is the EGFR T790M mutation, which emerged in over 50% of patients undergoing progression to a first-line TKI, and that could be counteracted by the use of third-generation TKIs such as osimertinib. 9
With regard to immunotherapy, the only biomarker approved in clinical practice is programmed death-ligand 1 (PD-L1) expression. Patients with advanced NSCLC can be treated in the first-line setting with pembrolizumab monotherapy only if the tumor shows a PD-L1 positivity of over 50%. 10 In the second-line setting, the same drug is U.S. Food and Drug Administration (FDA) approved for adult patients with different solid tumors that have a positive score >1%. 11 On the other hand, nivolumab has been approved in the second-line setting regardless of PD-L1 expression. 12
Table 1 shows the approved predictive biomarkers in clinical practice.
Approved predictive biomarkers in clinical practice.
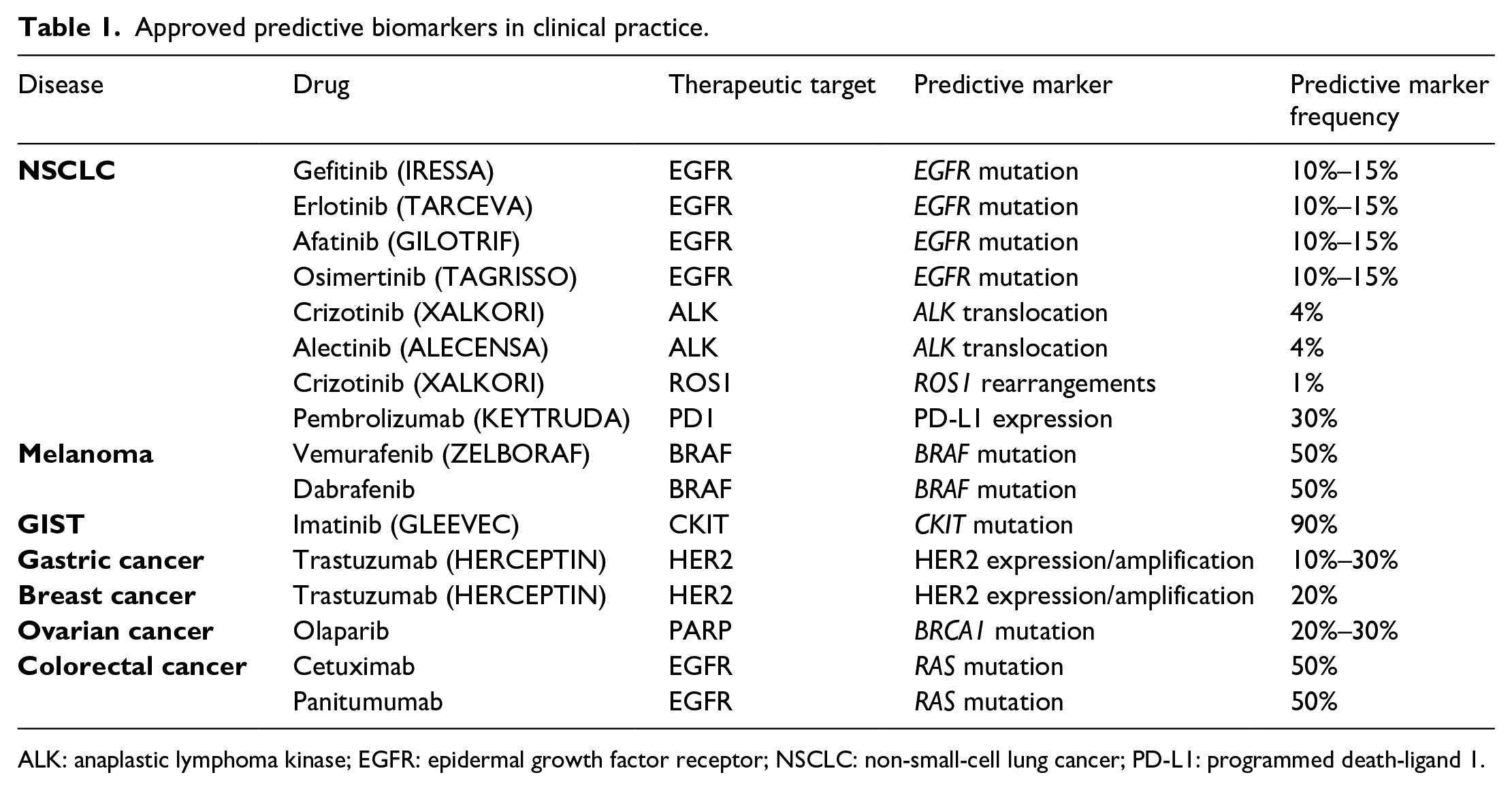
ALK: anaplastic lymphoma kinase; EGFR: epidermal growth factor receptor; NSCLC: non-small-cell lung cancer; PD-L1: programmed death-ligand 1.
Hallmarks of available biomarkers
All available molecular predictive biomarkers are not perfect. The objective response rate in patients carrying the specific alteration is about 70%–80%, meaning that a number of patients are not responsive to treatment despite the presence of the target alteration; this, in turn, means the presence of primary unknown resistance mutations. Moreover, it is known that a number of patients could respond to therapy despite the absence of the target alteration, meaning that there is still something to be discovered about the mechanism of action of these drugs.
The fact that the same alteration found in different diseases does not give the same sensitivity to the same drug is also intriguing. A well-known example of this is represented by the BRAF mutation, giving a high response to BRAF inhibitors, such as dabrafenib and vemurafenib, in melanoma, whereas in other pathologies, such as colorectal and lung cancers, very low response rates are observed. On the other hand, other biomarkers are seen to be transversally predictive of efficacy in several tumor types, such as neurotrophic receptor tyrosine kinase (NTRK) alteration.
The majority of approved predictive biomarkers in clinical practice are DNA-based alterations, such as point mutations or translocations. A number of reasons explain this fact. Most importantly, mutation analysis provides results in terms of the presence/absence of mutations and is easier to interpret than quantitative analyses in which specific cut offs and calibration curves must be established and standardized and whose results are interpreted in an objective and no operator-dependent way. These aspects reduce the variability and biases among the different laboratories, facilitating the standardization of procedures and guidelines. Moreover, the methodologies available for mutation analysis are usually easy and do not require sophisticated expertise. Finally, DNA is more stable with respect to RNA and proteins, rendering it more suitable to be analyzed starting from archived tissue material such as formalin-fixed paraffin-embedded specimens.
Emerging biomarkers in solid tumors
Targeted agents
A series of exciting biomarkers are under investigation to study the efficacy of their targeted therapies. 13 Some of these are disease-specific biomarkers, whereas other are site-agnostic biomarkers. With regard to NSCLC, together with the recommended biomarkers useful in clinical practice (EGFR, ALK, ROS1, BRAF, PD-L1), RET rearrangements and MET exon 14 mutations are also markers of interest for which clinical studies are ongoing to verify the efficacy of specific targeted agents. In prostate cancer, recent studies have demonstrated that patients with mutations at BRCA1/BRCA2 and ATM genes have a better outcome in relation to different types of treatments, and NCCN guidelines now recommend BRCA1/BRCA2 testing. In melanoma patients, biomarkers other than BRAF mutation have been identified, for which targeted therapies have demonstrated clinical activity. KIT mutations, present in about 20% of patients, is associated with a high response to imatinib. Another important gene is NRAS, which is mutated in about 20% of melanoma and gives sensitivity to MEK inhibitors.
Members of the NTRK fusion oncogene family, NTRK1/NTRK2/NTRK3, are present in a small percentage of tumors, including NSCLC, colorectal cancer, head and neck cancer, thyroid cancer, bladder cancer, glioma, melanoma. 14 Two targeted drugs, larotrectinib and entrectinib, have shown exciting results for the treatment of tumors carrying this alteration, and now testing of this biomarker is recommended.
Alterations of the fibroblast growth factor receptor (FGFR) family are also associated to response to FGFR tyrosine kinase inhibitors such as erdafitinib.
Immunotherapy
A series of biomarkers have been investigated for their potentiality to select patients to be treated with immunotherapy. Tumor mutational load is a measure of the number of mutations within a tumor genome, which is defined as the total number of mutations per coding area of a tumor genome. Mismatch repair (MMR) deficiency is an essential DNA repair mechanism that edits DNA mismatches. An MMR defect leads to an increased rate of mismatch errors and results in microsatellite instability. MMR-deficient tumors exhibit high tumor mutational burden (TMB), neoantigen load, and T-cell infiltration, and respond well to immune checkpoint blockade. Although the discovery of the association between MMR defects and response to immune checkpoint blockade is intriguing, only a few patients benefit from immunotherapy, in particular a subset of colon and endometrial cancer. Tumors with high TMB, such as melanoma, NSCLC, and urothelial cancers, have shown positive outcomes with treatment with immune checkpoint inhibitors. This is explained by the fact that high TMB increases the probability of neoantigen generation, leading to an activation of T-cell antitumor response. Standardization of TMB as a biomarker is challenging. Whole exome sequencing (WES) represents the gold standard for the estimation of TMB, 15 but the adoption of WES in routine clinical practice is difficult due to several aspects; that is, complex bioinformatics analysis requirement, the necessity of high DNA amount starting material, and the long analysis time. 15 Subsequently, several studies have demonstrated that TMB could be assessed by the analysis of targeted panels of genes. 16 However, the standardization of TMB based on gene panels among the different laboratories is also characterized by a series of difficulties, such as the selection of the gene panel to be used and the cut-off to be considered. TMB as a companion diagnostic might receive FDA approval in the near future in select tumor types, 17 and clinical trials confirming it as biomarkers will be needed in multiple tumor types.
Other potential biomarkers for immunotherapy have been suggested. A high density of tumor infiltrating lymphocytes (TILs), 18 including CD8-positive, CD3-positive, and CD4-positive TILs, is considered to reflect greater immune recognition of tumor cells in a patient, and represents a T-cell–inflamed tumor microenvironment. This inflamed tumor phenotype may be more sensitive to checkpoint blockade; therefore, in addition its prognostic role, TIL density has been studied for its predictive value as a biomarker for immunotherapy.19,20 The neutrophil-to-lymphocyte ratio (NLR) is a simple parameter that can be easily calculated from the standard complete blood count. A high NLR ratio is a negative prognostic indicator in patients with metastatic cancer treated with immunotherapy. 21 Moreover, a high pretreatment eosinophil count and a low neutrophil count have been correlated with improved response to ipilimumab and pembrolizumab in melanoma patients.22,23 Finally, gene expression profiling analysis has reported specific gene signatures that seem to be associated with the response to immunotherapy. 24
Conclusions
With regard to targeted therapy, a series of validated and trusted biomarkers are available in clinical practice to guide patient selection. However, the main issues regard primary resistance mechanisms, which lead a portion of patients to be resistant to therapy from the beginning, and the induction of acquired resistance mechanisms, which cause a limited duration of response. These resistance mechanisms are only partially understood and should be studied in more detail. On the other hand, no accurate biomarkers are available to guide the selection of patients who are more likely to respond to immunotherapy, and future studies are necessary to identify such predictive biomarkers with the aim to reduce costs and improve patient management.
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.