
Abstract
The role of biomarkers is crucial in oncology for both early diagnosis and the personalization of cancer treatments. Tissue biomarkers have gained a central role as predictors of the response to an increasing number of anticancer agents; conversely, the clinical role of circulating biomarkers (c-TMs) is limited and has remained almost unchanged over the years. The position of guidelines is summarized and discussed with reference to the potential usefulness of c-TMs in those areas of application that cannot be covered by tissue biomarkers. The pipeline of translational research on biomarkers is briefly described; the differences among analytical validation, clinical validation, and clinical utility are discussed, emphasizing that the assessment of clinical utility is the ultimate step toward clinical use. The role of monitoring of appropriateness as a proxy indicator of how the research pipeline has actually worked is discussed, and data and c-TMs overordering rates are reported. The role and limits of guidelines to influence appropriate c-TMs ordering are discussed. The design of primary studies on c-TMs is examined, underlining that they mainly focus on clinical validation rather than on clinical utility. The role of regulatory boards is also briefly presented and discussed.
Translation research in cancer biomarkers is a crucial area for both the development of novel tools for early cancer diagnosis and the personalization of cancer treatments. Cancer biomarkers can be assessed in a variety of biological materials, including tumor tissue, serum or plasma, urine, feces, serous effusions, and aspirates from, or washing fluids of, natural body cavities. Tumor tissue and serum or plasma are by far the most widely used biological materials in clinical practice. In the last decade, tissue biomarkers have gained a crucial role as prognostic indicators and, foremost, for the prediction of the response to an increasing number of biological targeted anticancer agents. Conversely, the clinical role of circulating biomarkers has remained almost unchanged over the years and appears rather limited; in fact, clinical practice guidelines recommend quite a few circulating tumor markers (c-TMs) in a restricted number of scenarios of a limited number of solid malignancies.1-3 Recommended c-TMs are tissue specific markers (i.e. PSA, thyroglobulin), onco-fetal antigens (e.g. CEA, AFP) and carbohydrate antigens (e.g. CA125, CA19-9, CA15.3). They were all discovered over 30 years ago and are associated with tumor bulk. 4 This lack of perceivable progress conflicts with the potential usefulness of c-TMs in those areas of application that cannot be covered by tissue biomarkers (summarized in Table 1).
Potential developments in clinical applications of cancer biomarkers in blood or tumor tissue.
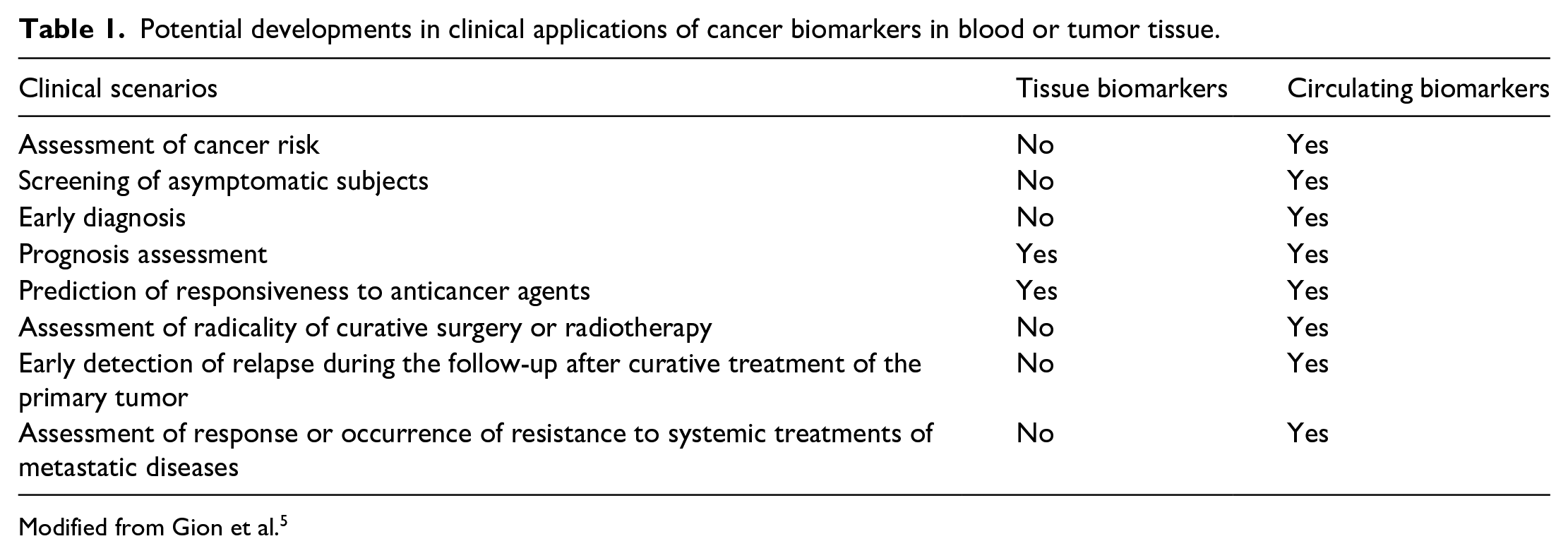
Modified from Gion et al. 5
In order to meet the needs for the clinical application of cancer biomarkers, a continuous research effort has been carried out to identify novel candidate c-TMs for both early diagnosis and prediction of response to therapies. Hundreds of molecules, including proteins (e.g. cytokines, signaling molecules, adhesion molecules, proteinases) and nucleic acids (e.g. cfDNA, miRNA, lncRNAs), are currently under investigation around the world. Several of these molecules present a solid biological rationale to be considered putative candidate markers for the clinical practice. Some of the most promising approaches in biomarker investigation seem to be the determination of batteries of markers with different biological implications 6 and the study of biomarkers in circulating extracellular vesicles. 7 The challenge with c-TMs is to translate a constantly increasing complexity (biological, analytical, computational) into tools and decision criteria that are realistically transferable to the clinical practice in a reasonable time frame. The pipeline of translational research on biomarkers can be schematically separated into four steps: (a) basic science discoveries, (b) analytic validation, (c) clinical validation, and (d) assessment of clinical utility 8 ; the latter should eventually produce suitable evidence to be included in the recommendations of clinical practice guidelines. An effective research pipeline is ultimately expected to lead to the appropriate implementation of a given intervention in clinical practice. Thus, appropriateness monitoring may be regarded as a proxy indicator of how the research pipeline has actually worked, cautiously keeping in mind that this simplified approach does not consider the impact of external barriers (e.g. economic issues, organizational settings, emotional aspects). Since their first discovery, traditional c-TMs (e.g. CEA, AFP, CA125, PSA) have been evaluated in thousands of subjects and used for clinical decisions in hundreds of thousands of patients, using fully standardized assay methods supervised through established quality assurance programs. Therefore, they are a paradigmatic example to test how results of research have been eventually translated in clinical practice. However, the existing systematic reviews on the appropriateness of laboratory tests do not present established indicators to monitor the appropriateness of test ordering, and the appropriateness of c-TMs requests is actually unknown.9,10 Recently, we developed “ordering rate indicators” as proxy indicators of inappropriateness using an epidemiology-based model 11 ; in brief, registered c-TMs requests were weighed against expected orders of c-TMs—the latter is assumed on the basis of cancer prevalence and guidelines recommendations. We showed a very elevated ordering rate in Italy (221 c-TMs orders per 1000 inhabitants) with reference to tumor prevalence. In fact, order patterns of c-TMs recommended only in some specific malignancies (i.e. CA125, CA15.3, CA19.9) appeared totally unrelated to the epidemiological figures of the malignancies in which the markers are indeed recommended. 11 From the health care side, the demonstrated overuse of traditional c-TMs is expected to cause overdiagnosis and risk of overtreatment, to lead to unnecessary costs, and to induce an overload of health care services for confirmatory tests in false positive cases. From the research side, the evidence of such a huge overuse of c-TMs indicates that the pipeline of translational research has not been fully effective at least in the implementation phase, given that the compliance of clinicians to recommendations on c-TMs of clinical practice guidelines seems to be poor. The reason for this poor compliance is manifold, as quality, consistency, and completeness of clinical practical guidelines may limit their implementation in the clinical practice. Recently, recommendations on c-TMs offered by clinical practice guidelines have been evaluated by our research group; in brief, a systematic search of clinical practice guidelines on solid tumors was performed in literature databases and websites; pertinent guidelines were selected and assessed according to their quality; and recommendations were summarized and compared side-by-side.1-3 The quality of method and reporting of guidelines was assessed in a collateral study. 12 In brief, 590 documents were classified as being informed by a systematic search method using criteria inspired by Oxman and Guyatt, 13 Jadad and Enkin, 14 and NICE. 15 As summarized in Table 2, only 28.5% of the examined guidelines have been prepared according to a properly performed and reported systematic search of the literature. Surprisingly, 27.8% of documents claiming to be “guidelines” appear to have been produced without any type of literature analysis.
Classification of 590 documents reported as clinical practice guidelines on the basis of literature search methods.
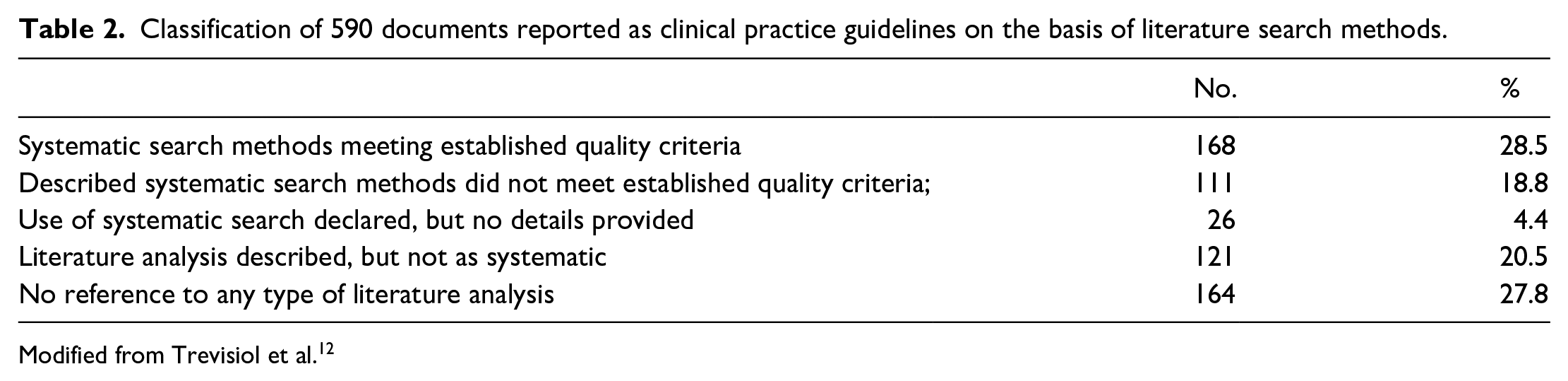
Modified from Trevisiol et al. 12
These findings indicate that the methodological quality of approximately 70% of available guidelines is still suboptimal, with one-quarter of them being formally unacceptable. It may be postulated that the poor methodological quality of available guidelines might negatively impact on their implementation. The two additional points that we explored were the completeness and the consistency of recommendations on c-TMs regarding common diagnostic or therapeutic questions arising in typical clinical scenarios (i.e. screening, diagnosis, initial work-up, short-term reassessment, and long-term monitoring after curative treatment of the primary tumor, monitoring of the treatment of advanced disease). The completeness of the guidelines was generally poor. While recommendations on c-TMs are available for the majority of clinical scenarios in a few malignancies (i.e. thyroid cancer, testicular tumors), recommendations are lacking in several clinical scenarios for the majority of cancer types.1-3 As a consequence, clinicians cannot make informed decisions on the available evidence, running the risk of taking arbitrary, and possibly inappropriate, choices.
As concerns consistency, recommendations from different guidelines has resulted in contradictions in some clinical scenarios; for example, some guidelines recommend for, and some others against, the use of alpha-fetoprotein in both the screening and diagnosis of hepatocellular carcinoma 1 ; likewise, the use of CA125 in the follow-up of ovarian cancer is advocated by some guidelines, while others recommend against it. 2 This lack of consistency may lead to an odd assessment of appropriateness, since the request of a c-TM can be classified as appropriate according to one guideline, or inappropriate according to another. The reason why available guideline recommendations either fail to meet several clinical questions on c-TMs, or may provide different recommendations on the same clinical question, is possibly related to shortcomings in the translational research pipeline. As previously mentioned, the requirements to be fulfilled to adopt a biomarker in clinical practice are analytical validity, clinical validity, and clinical utility.4,8 Analytic validity concerns the accuracy with which a biomarker is measured by a given laboratory test. It includes the specific technical requirements of the chosen assay and its performances (i.e. analytical sensitivity, specificity, trueness, reproducibility). Clinical validity describes the accuracy with which a test is associated with a particular clinical condition (i.e. diagnostic sensitivity, specificity, positive and negative predictive value) or predicts a clinical outcome (i.e. prognosis, the response to a drug). Clinical utility refers to the risks and benefits associated with the use of the test in clinical practice. The measurement of clinical utility is based on the assessment of the medical and social outcomes resulting from the test results, including succeeding interventions in subjects with either positive or negative test results. Clinical utility implies that high levels of evidence exist to support the claim that the use of the test produces better outcomes for the patient than if it were not available. Clinical utility cannot be achieved without analytical and clinical validity, but analytical and clinical validity alone are insufficient to introduce the test into routine practice. 4
The reason why completeness and consistency of clinical practice guidelines on c-TMs are poor is frequently due to the fact that guidelines with high methodological quality do not endorse the results of research studies as they cannot recommend on the basis of analytical or clinical validity only, while guidelines presenting methodological flaws may occasionally base their recommendations also on clinical validity.
The regulatory boards do not contribute to drive research on c-TMs toward a clinical utility framework. In the European Union, in vitro diagnostics (IVD) may be commercialized with a CE mark after assessment and approval from a notified body. For IVD, the certification focusses on the technical features and technical quality of the products. 16 In the USA, the approval of a tumor marker by the Food and Drug Administration is also focused on analytical validity and does not necessarily imply that it should be beneficially used to direct patient care. 17
As a matter of fact, the vast majority of published studies on c-TMs have been designed to assess analytical and clinical validity, with diagnostic accuracy, prognosis, and predictive values being their explicit goals. Also some of the most recent and promising studies on c-TMs are indeed focused on clinical validity.6,7 Studies on the clinical utility of c-TMs are indeed complex and time consuming, since the effect of the marker on clinical outcomes must be distinguished from that of other variables that are necessarily present in the study design (e.g. accuracy of reference diagnostic procedures, efficacy of therapies, length of the follow-up). Studies on the role of PSA for prostate cancer screening are a paradigmatic example of studies on c-TMs focused on clinical utility 18 ; these studies have been performed in thousands of men and have lasted tens of years to reach reasonably sound evidence to be translated into recommendations of clinical practice guidelines; in addition, they have been carried out approximately after 40 years since the identification of PSA and thousands of inconclusive studies. Likewise, the value of the routine measurement of CA125 in the follow-up of patients with ovarian cancer has been disclaimed 30 years after the identification of the marker through a clinical utility study whose results were published in 2010. 19 In brief, women with ovarian cancer in complete remission after first-line platinum-based chemotherapy and a normal CA125 concentration were registered for this randomized controlled trial. Clinical examination and CA125 measurement were done every 3 months. If CA125 concentration exceeded twice the upper limit of normal, patients were randomly assigned to early or delayed chemotherapy. Median survival from randomization was 25.7 months (95% confidence interval (CI) 23.0, 27.9) for patients on early treatment and 27.1 months (95% CI 22.8, 30.9) for those on delayed treatment. 19 Results have been, in part, adopted by clinical practice guidelines, although this study has several faults, including almost certainly a selection bias (1442 registered patients from 59 institutions across 10 countries and lasted 10 years). 20 Undoubtedly, the approach used for PSA and CA125 does not fit with the continuous progress on knowledge of cell biology and the startling development of technologies, which have moved biomarkers toward the most advanced boundary of diagnosis and treatment of cancer.
In summary, the potential clinical role of novel c-TMs in oncology is rapidly growing. We have shown that the clinical use of classical c-TMs is largely inappropriate, due at least in part to the scarcity of evidence on their clinical utility. This paradigmatic example emphasizes the urgent need for a re-engineering of clinical research to facilitate the efficient translation of new biomarker assays in clinical practice. Such re-engineered research should use appropriate study designs based on clinical utility endpoints, whether in formal trials or in real-world studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.