
Abstract
Background:
Changes in circulating adiponectin have been related to the risks of various cancers. However, the association between circulating adiponectin and the risk of renal cell carcinoma has not been fully determined. A meta-analysis was performed to evaluate the relationship between circulating adiponectin and renal cell carcinoma risk.
Methods:
Observational studies that evaluated the association between circulating adiponectin and renal cell carcinoma risk were identified via a systematic search of PubMed and Embase databases. The difference between circulating adiponectin in renal cell carcinoma cases and healthy controls, and the multivariable adjusted association between circulating adiponectin and renal cell carcinoma risk were evaluated. A random effects model was used if significant heterogeneity existed; otherwise a fixed effects model was applied.
Results:
Eight case-control studies with 2624 renal cell carcinoma cases and 2904 healthy controls were included. Pooled results showed that circulating adiponectin was significantly lower in renal cell carcinoma cases than in healthy controls (mean difference = −1.08 ug/mL; 95% confidence interval (CI) −1.62, −0.54; P < 0.001). Higher circulating adiponectin was independently associated with a significantly lowered risk of renal cell carcinoma (adjusted odds ratio for 1 SD increment of adiponectin = 0.78; 95% CI: 0.63, 0.96; P = 0.02). Subgroup analyses according to characteristics including study design, ethnics of participants, blood samples, numbers of participants, mean ages of participants, and study quality showed consistent results.
Conclusions:
Lower circulating adiponectin is associated with increased risk of renal cell carcinoma. The potential pathophysiological mechanisms underlying the role of circulating adiponectin in the pathogenesis of renal cell carcinoma deserve further investigation.
Introduction
Renal cell carcinoma (RCC) is one of the most common malignancies in the urological system, and the global incidence of the cancer has risen gradually during the last decade.1,2 Accumulating evidence suggests that the etiology of RCC is multifactorial, 3 and obesity has been generally considered as a key risk factor of RCC pathogenesis.4,5 However, the role of obesity in RCC patients may be complicated. 6 Some studies showed that although obesity is related to a higher risk of RCC incidence, obesity patients with RCC seemed to have longer overall survival.7,8 Therefore, extensive research is needed to understand the potential mechanisms underlying the association between obesity and RCC risk.
Previous studies indicated that obesity is associated with significant changes of a few circulating cytokines secreted by adipose tissue, such as adiponectin. 9 As a 30-kD protein produced by white adipose tissue, adiponectin confers various biological effects, including anti-inflammation, and the maintenance of insulin sensitivity, anti-atherosclerosis, and anti-cancer. 10 Previous meta-analyses have shown that lower circulating adiponectin is an important marker of many obesity-related cancers (e.g. breast, 11 prostate, 12 and colorectal. 13 However, the association between circulating adiponectin and the risk of RCC has not been fully determined. In a few pilot studies, lower circulating adiponectin was observed in RCC cases than in healthy controls,14-17 while no significant difference of circulating adiponectin was observed between RCC cases and controls in some other studies.18-21 The inconsistency of these findings may be explained by the differences of study population and sample sizes of the studies. A previous meta-analysis by Yap et al. 22 included seven studies14-16,18-21 and concluded that patients with RCC had lower circulating adiponectin than healthy controls. However, a recently published study was not included. 17 In addition, whether the difference between adiponectin in RCC cases and healthy controls is independent of study characteristics—such as study design, ethnics of participants, blood samples, numbers of participants, mean ages of participants, and study quality—remain to be determined. Therefore, in this study, we aimed to perform a meta-analysis to systematically evaluate the potential association between circulating adiponectin and RCC risk.
Methods
This study was performed in accordance with the MOOSE (Meta-analysis of Observational Studies in Epidemiology) 23 and Cochrane’s Handbook 24 guidelines.
Database search
We searched the databases of PubMed and Embase for relevant records, using the terms of “adiponectin”, combined with “renal” or “kidney”, and “tumor”, “cancer”, “neoplasm”, or “carcinoma”. We limited the search to human studies published in English. A manual analysis of the reference lists of original and review articles was performed as a supplement. The final search was performed on April 10, 2019. The full search strategy for PubMed is shown in Supplementary File 1.
Inclusion and exclusion criteria
Studies were included if they met the following criteria: (a) full-length article in English; (b) designed as cross-sectional or nested case-control studies, or cohort studies; (c) aimed to evaluate the association between circulating adiponectin and the risk of RCC; (d) diagnosis of RCC was evidenced by the histopathological findings; (e) circulating adiponectin was measured before any treatment for RCC was applied; and (f) reported the difference between the means of circulating adiponectin between RCC patients and healthy controls at baseline and/or adjusted odds ratio (OR) and 95% confidence intervals (CIs) for the association between circulating adiponectin and RCC risk. Subjects of either sex and any age were included. Reviews, editorials, or preclinical studies, and clinical studies that were not relevant to the aim of the current meta-analysis were excluded.
Data extracting and quality evaluation
Database search, data extraction, and quality assessment were independently performed by two authors, and discrepancies were resolved by consultation with the corresponding author. The data extracted include: (a) first author, location, and design of the study; (b) types of the blood samples and methods for the measurement of adiponectin; (c) numbers of RCC cases and healthy controls, and their mean ages; and (d) variables adjusted when presenting the OR and 95% CI for the association between adiponectin and RCC risk. Study quality evaluation was performed with the Newcastle–Ottawa Scale, 25 which ranges from 1 to 9 stars and judges each study regarding three aspects: selection of the study groups; the comparability of the groups; and the measurement of exposure.
Statistical analyses
The difference between the circulating level of adiponectin was presented as mean difference (MD) and 95% CI, and estimated with the means and SDs of adiponectin in RCC cases and healthy controls in each study. The means and SDs were imputed as previously reported if the circulating adiponectin was reported as medians and ranges (or interquartile ranges). 26 The OR and 95% CI were extracted as a measure of risk associated to adiponectin (1-SD) increments. The data of ORs and their corresponding stand errors (SEs) were calculated from 95% CIs or P values, and were logarithmically transformed to stabilize variance and normalized the distribution. 24 The Cochrane’s Q test and I2 test were performed to evaluate the heterogeneity among studies. 27 An I2 > 50% indicated significant heterogeneity. A fixed-effect model was applied if no significant heterogeneity was detected; otherwise, a random effects model was applied. Sensitivity analyses—by removing individual studies one at a time—were performed to evaluate the stability of the results. 28 Influences of study characteristics, such as study design, ethnicity of participants, blood samples, numbers of participants, mean ages of participants, and study quality on the outcomes, were evaluated by predefined subgroup analyses. Potential publication bias was assessed by funnel plots with the Egger regression asymmetry test. 29 RevMan (Version 5.1; Cochrane Collaboration, Oxford, UK) and STATA software (Version 12.0; Stata Corporation, College Station, TX, USA) were used for the statistical analyses.
Results
Results of literature search
The processes of database search and study identification were presented in Figure 1. Overall, 621 studies were obtained via an initial database search, and 602 were excluded based on title and abstract mostly because they were irrelevant to the aim of the meta-analysis. The remaining 19 studies underwent full-text review. Of them, 11 were further excluded because 3 of them reported overall cancer risk rather than RCC risk; 1 reported cancer mortality rather than RCC risk; 2 did not measure circulating adiponectin; 2 were reports of the same cohorts; and the other 3 did not include control groups of healthy participants. Finally, 8 studies14-21 were included.
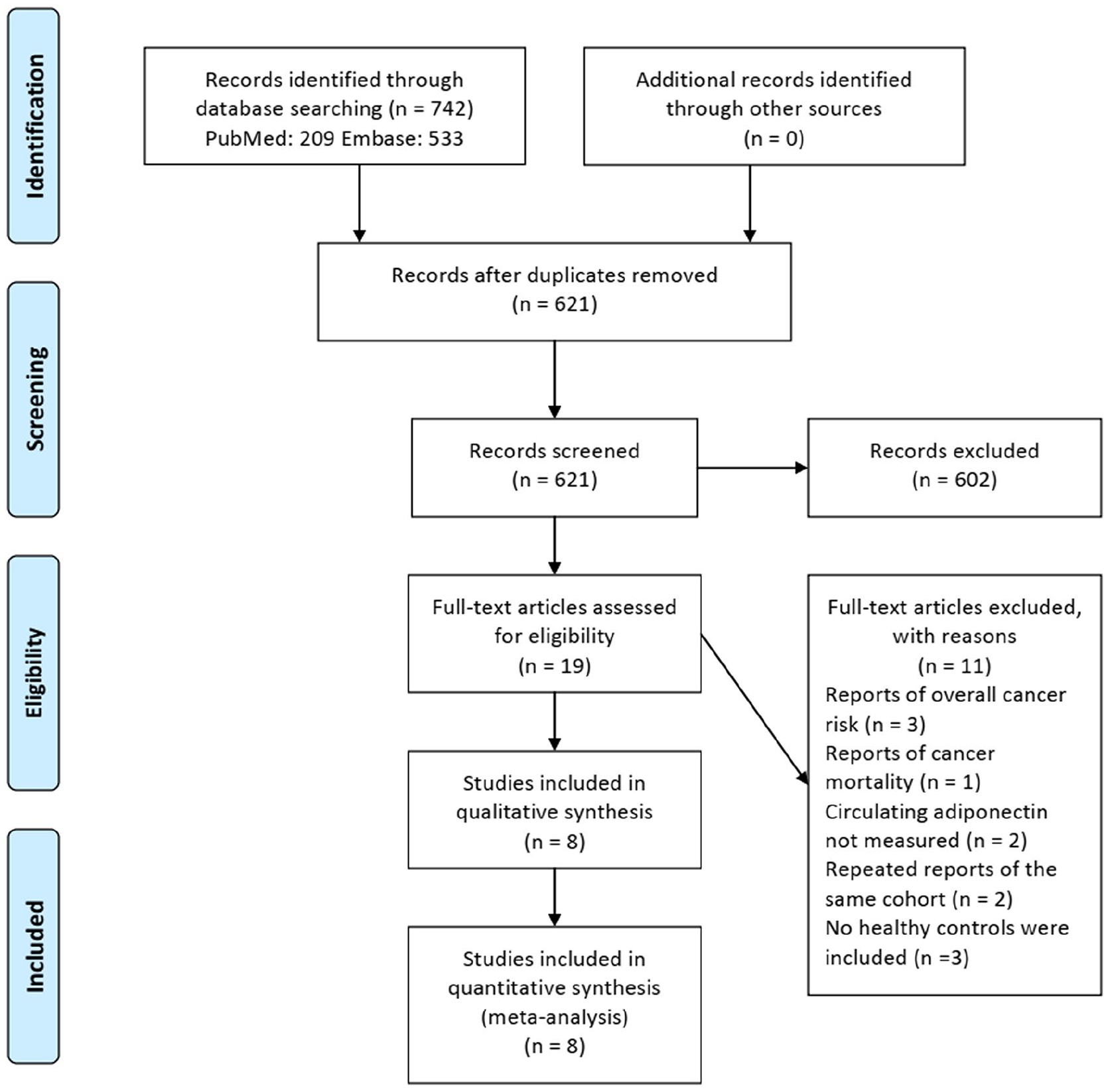
Flowchart of database search and study identification.
Study characteristics and quality evaluation
The characteristics of the included studies are presented in Table 1. Overall, our meta-analysis included 8 observational studies including 2624 RCC cases and 2904 healthy controls.14-21 One study included two independent sets of data from Caucasians and African Americans, 14 and another study included two independent sets of data from a discovery phase and a validation phase. 17 These datasets were included independently for the estimation of the difference in circulating adiponectin between RCC cases and healthy controls. These studies were performed in Greece, 18 Finland, 19 the USA,14,21 Korea, 15 and China.16,17,20 Three of them were designed as nested case-control studies,14,19,21 and the others were designed as case-control studies.15-18,20 Circulating adiponectin was measured by radioimmunoassay (RIA) in one study, 18 and by enzyme-linked immunosorbent assay (ELISA) in the others14-17,19-21; plasma was used for the measurement of adiponectin in three studies,15-17 while serum was used in the others.14,18-21 The number of participants ranged between 79 and 1169, and the mean ages varied from 55.0 to 68.4 years. Five studies14,15,18,19,21 reported ORs and 95% CIs for the association between adiponectin and RCC risk after the full adjustment of participant characteristics such as age, gender, body mass index (BMI), smoking, hypertension, and diabetes. The Newcastle–Ottawa Scale varied from 7 to 9 for the included studies (Supplementary File 2).
Characteristics of the included studies.
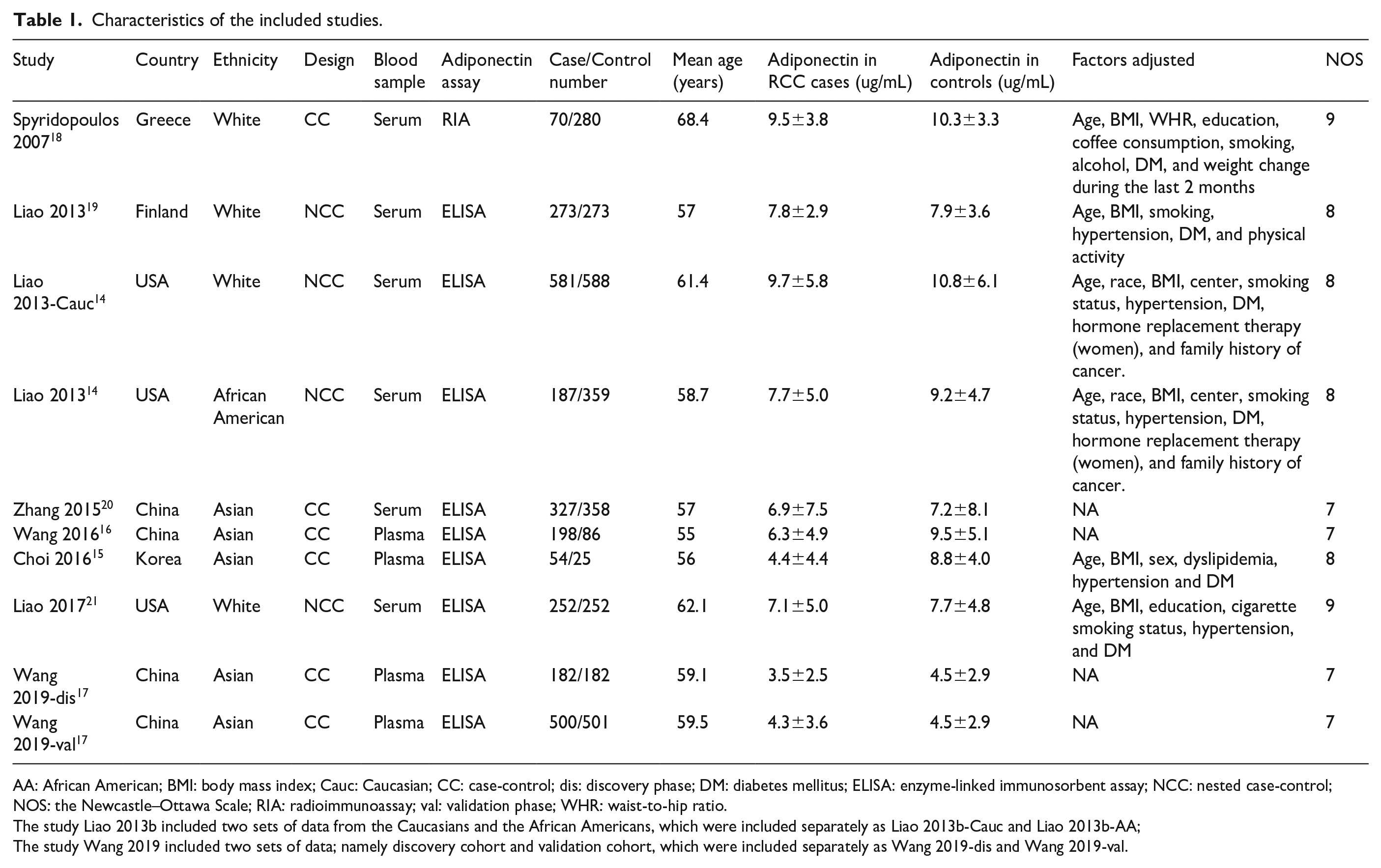
AA: African American; BMI: body mass index; Cauc: Caucasian; CC: case-control; dis: discovery phase; DM: diabetes mellitus; ELISA: enzyme-linked immunosorbent assay; NCC: nested case-control; NOS: the Newcastle–Ottawa Scale; RIA: radioimmunoassay; val: validation phase; WHR: waist-to-hip ratio.
The study Liao 2013b included two sets of data from the Caucasians and the African Americans, which were included separately as Liao 2013b-Cauc and Liao 2013b-AA;
The study Wang 2019 included two sets of data; namely discovery cohort and validation cohort, which were included separately as Wang 2019-dis and Wang 2019-val.
Difference of circulating adiponectin in RCC cases and healthy controls
Ten datasets from eight studies evaluated the difference of circulating adiponectin in RCC cases and healthy controls.14-21 Significant heterogeneity was detected (P for Cochrane’s Q test < 0.001; I2 = 80%). Pooled results with a random effects model demonstrated that circulating adiponectin was significantly lower in RCC cases than in healthy controls (MD = −1.08 ug/mL; 95% CI −1.62, −0.54; P < 0.001; Figure 2(a)). Sensitivity analyses (by excluding one study at a time) did not change the results (MD: −0.85 ~ −1.23; P all < 0.05). The results of predefined subgroup analyses are shown in Table 2. The level of circulating adiponectin was significantly lower in RCC cases than in healthy controls regardless of the study characteristics—including study design, ethnicity of participants, blood samples, numbers of participants, mean ages of participants, or study quality—indicating the robustness of the results.
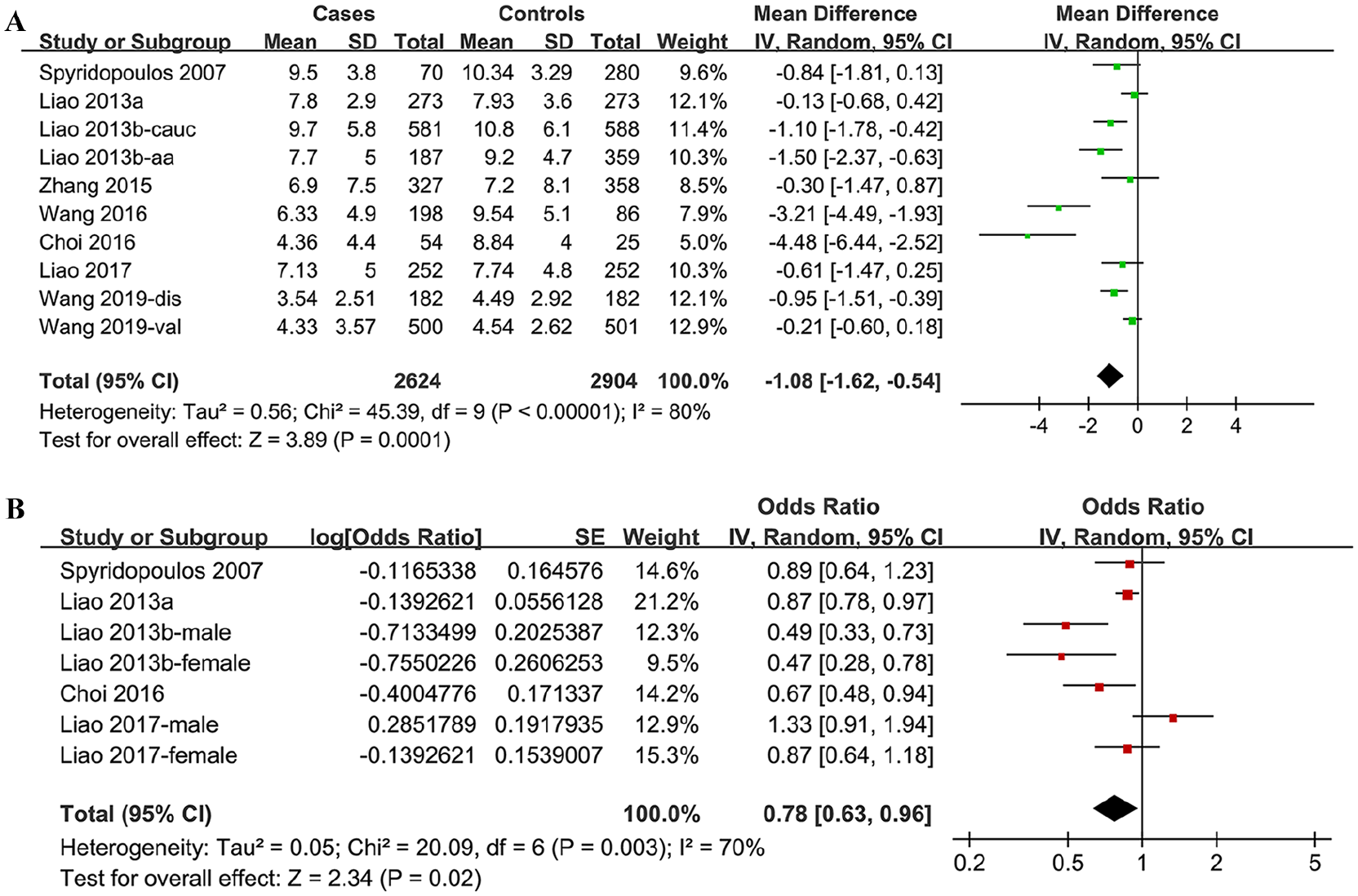
Forest plots for the meta-analyses of the association between adiponectin and RCC risk. (a) Forest plots for the overall meta-analysis of the difference between circulating adiponectin in RCC cases and healthy controls. (b) Forest plots for the overall meta-analysis of the multivariable adjusted association between circulating adiponectin and RCC risk.
Subgroup analyses for the meta-analysis of circulating adiponectin in RCC patients and healthy controls.
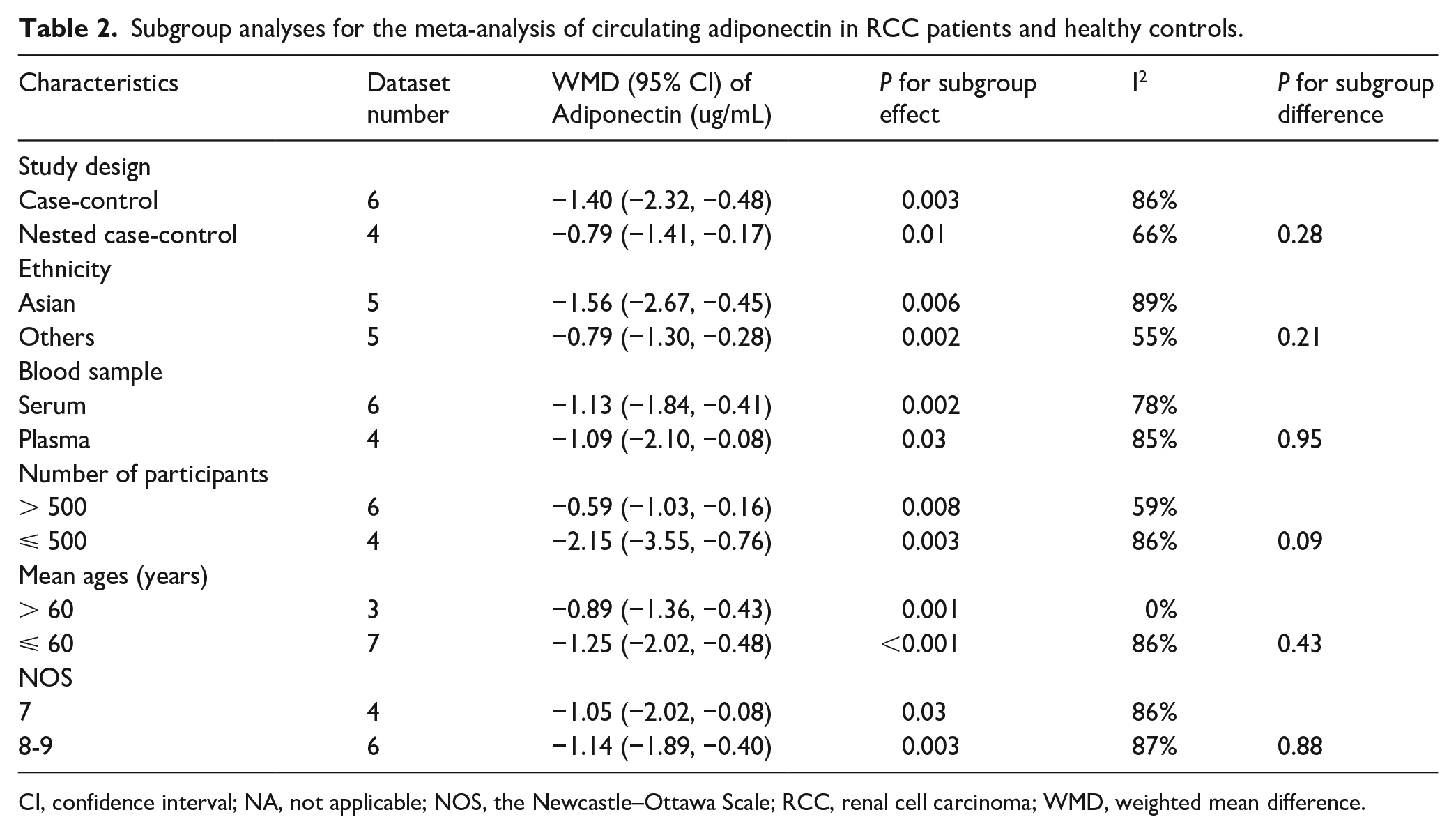
CI, confidence interval; NA, not applicable; NOS, the Newcastle–Ottawa Scale; RCC, renal cell carcinoma; WMD, weighted mean difference.
Adjusted association between circulating adiponectin and RCC risk
Seven datasets from five studies14,15,18,19,21 reported the multivariable adjusted ORs and 95% CIs for the association between adiponectin and RCC risk. Significant heterogeneity was detected (P for Cochrane’s Q test = 0.003; I2 = 70%). Pooled results with a random effects model demonstrated that higher circulating adiponectin was independently associated with significantly lowered risk of RCC (adjusted OR for 1-SD increment of adiponectin = 0.78; 95% CI 0.63, 0.96; P = 0.02; Figure 2(b)). Sensitivity analyses by excluding one study at a time did not change the results (adjusted OR: 0.76 ~ 0.84; P all < 0.05).
Publication bias
The funnel plots for the meta-analysis of the difference between circulating adiponectin in RCC cases and controls, and the adjusted ORs for the association between circulating adiponectin and RCC risk were shown in Figure 3(a) and (b). The funnel plots were symmetric on visual inspection. The results of the Egger’s regression tests also did not indicate significant publication biases (P values for Egger’s regression tests: 0.198 and 0.524).
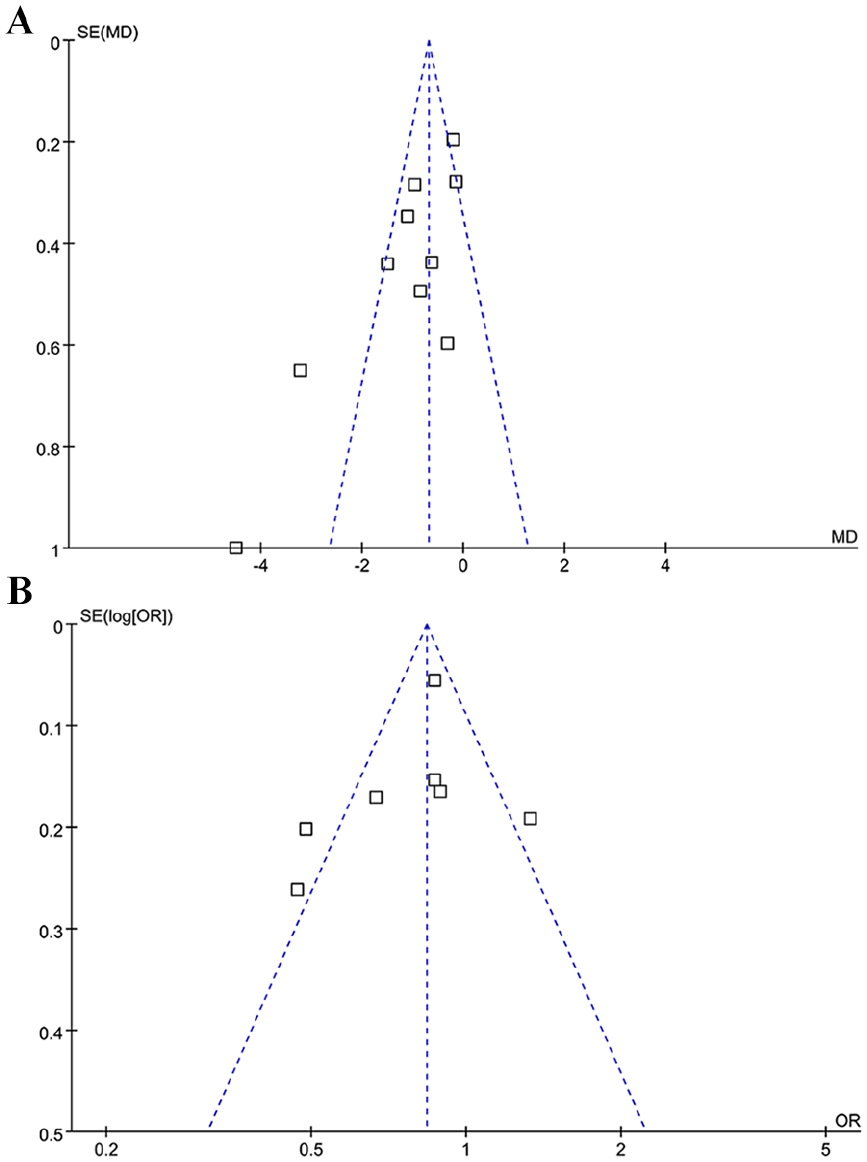
Funnel plots for the meta-analyses. (a) Funnel plots for the meta-analysis of the difference between circulating adiponectin in RCC cases and controls. (b) Funnel plots for the meta-analysis of the adjusted ORs for the association between circulating adiponectin and RCC risk.
Discussion
In this meta-analysis of eight case-control studies, we found that the circulating adiponectin was significantly lower in RCC cases than the matched healthy controls. By pooling the results of multivariable models, we found that higher circulating adiponectin was significantly associated with a lower risk of RCC, which is independent of other confounding factors such as age, gender, BMI, smoking habit, and comorbidities of hypertension and DM. These results suggested that lower circulating adiponectin may be an independent risk factor for RCC.
Our study has the following strengths compared to the previous meta-analysis by Yap et al. 22 First, we included the most recently published studies, and the overall sample size of the included studies is larger than the previous one (5528 vs. 4527). By additionally including one recent study published in 2019, 17 our study confirmed the finding of Yap et al.—that patients with RCC had lower circulating adiponectin than the healthy controls. Second, we performed the subgroup analyses and found that the difference between adiponectin in RCC cases and healthy controls is independent of study characteristics such as study design, ethnics of participants, blood samples, numbers of participants, mean ages of participants, and study quality. Third, we combined the results of studies reporting the independent association between adiponectin and RCC, and demonstrated that higher circulating adiponectin was independently associated with a significantly lowered risk of RCC (adjusted OR for 1-SD increment of adiponectin = 0.78). These results strongly suggest an independent association between higher adiponectin and lower RCC risk.
Obesity has been established as a risk factor for RCC. In an early meta-analysis of 24 cohort studies, it was demonstrated that obesity was associated with a 76% higher risk of RCC compared with normal-weight participants. 30 Subsequent analyses showed that the association between obesity and RCC risk was consistent in both males and females. 30 However, the pathophysiological mechanisms underlying the association between obesity and RCC remain undetermined. Since obesity has been related to lower circulating adiponectin, 31 and lowered circulating adiponectin has been related to risks of various obesity-related cancer, 32 we hypothesized that lower circulating adiponectin may be associated with increased RCC risk. The results of our meta-analysis confirmed these assumptions by showing that the circulating adiponectin was significantly lower in RCC cases than in healthy controls. Our findings further showed that lower circulating adiponectin remains an independent risk factor for RCC even after adjustment of other confounding factors, including age, smoking, BMI, and DM status. To date, we have been unable to determine whether lower adiponectin was simply a marker of RCC risk or it was involved in the carcinogenesis processes. To the best of our knowledge, experimental evidence is generally lacking regarding the role of adiponectin in the pathogenesis and progression of RCC. However, the potential inhibitory role of adiponectin on other cancers has been elucidated in some previous experimental studies.9,10 In vitro studies have shown that adiponectin inhibited carcinogenesis and proliferation of colorectal cancer cells by downregulating COX-2 expression. 33 In prostate cancer cells, adiponectin suppressed the growth of the cancer through inhibition of vascular endothelia growth factor (VEGF)-A-mediated cancer neovascularization. 34 Since VEGF signal pathways have been demonstrated to be involved in the carcinogenesis and metastasis of RCC, 35 it could be hypothesized that adiponectin may also influence RCC risk via the interaction of molecular pathways including VEGF. Future studies are warranted to elucidate the potential pathophysiological mechanisms underlying the role of circulating adiponectin in the pathogenesis of RCC.
Our study has limitations that should be considered in interpreting the results. First, considerable heterogeneity was detected among the included studies, and the number of studies included in the meta-analysis was relatively small, which prevented us from thoroughly investigating the source of heterogeneity. The results of subgroup analyses showed that factors including study design, ethnics of participants, blood samples, numbers of participants, mean ages of participants, and study quality were not significant modifiers for the outcome (P all > 0.05). However, the results of the subgroup analyses should also be treated cautiously as the results of the subgroup difference tests are conditioned by the small sample size and limited studies included in each stratum. Second, only the association between total adiponectin and RCC was investigated. The association between subtypes of adiponectin (e.g. the high molecular weight adiponectin) and RCC risk was unable to be determined since relevant reports are rare. Third, as a meta-analysis of case-controls studies—although some of the potential confounding factors including age, gender, smoking, BMI, and DM were adjusted when presenting the association between circulating adiponectin and RCC risk—we could not exclude other factors that may confound the association. Moreover, a causative relationship between reduced adiponectin and RCC could not be retrieved based on our findings since the nature of the study is a meta-analysis of observational studies. Finally, whether treatment strategies that increase adiponectin levels could prevent RCC remains to be evaluated in future studies.
In conclusion, results of this meta-analysis indicated that lower circulating adiponectin is associated with an increased risk of RCC. The potential pathophysiological mechanisms underlying the role of circulating adiponectin in the pathogenesis of RCC deserve further investigation.
Supplemental Material
Supplementary_file_1 – Supplemental material for Lower circulating adiponectin is associated with higher risk of renal cell carcinoma: A meta-analysis
Supplemental material, Supplementary_file_1 for Lower circulating adiponectin is associated with higher risk of renal cell carcinoma: A meta-analysis by Jiajie Fang, Xuanli Xu, Qiqi Mao, Yufan Ying, Xu Zhang and Liping Xie in The International Journal of Biological Markers
Supplemental Material
Supplementary_file_2 – Supplemental material for Lower circulating adiponectin is associated with higher risk of renal cell carcinoma: A meta-analysis
Supplemental material, Supplementary_file_2 for Lower circulating adiponectin is associated with higher risk of renal cell carcinoma: A meta-analysis by Jiajie Fang, Xuanli Xu, Qiqi Mao, Yufan Ying, Xu Zhang and Liping Xie in The International Journal of Biological Markers
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Zhejiang Excellent Young Talents Fund of Traditional Chinese Medicine (Grant number: 2018ZQ030).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.