
Abstract
Background:
Membranous nephropathy is the most common glomerular disease related to malignancy. However, it is difficult to distinguish between true malignancy-related membranous nephropathy and idiopathic membranous nephropathy coincident with cancer. It has been reported that phospholipase A2 receptor (PLA2R) is the first autoantigen involved in idiopathic membranous nephropathy and thrombospondin type-1 domain-containing 7A (THSD7A) may have a close relationship with malignancy-related membranous nephropathy. Therefore, the aim of this study was to compare the clinicopathological characteristics between membranous nephropathy patients with cancer and idiopathic membranous nephropathy patients without cancer to better detect malignancy-related membranous nephropathy, including glomerular PLA2R and THSD7A depositions and their circulating antibodies, together with glomerular IgG4 deposition.
Methods:
Twelve membranous nephropathy patients with cancer and 257 idiopathic membranous nephropathy patients without cancer were included in this study and had been followed up for more than 1 year. The glomerular expression of PLA2R, THSD7A, and IgG4 was analyzed by immunohistochemistry. Circulating anti-PLA2R and anti-THSD7A antibodies were assessed by enzyme-linked immunosorbent assay and indirect immunofluorescence testing, respectively.
Results:
Membranous nephropathy patients with cancer were significantly older and had higher serum creatinine and a lower estimated glomerular filtration rate than idiopathic membranous nephropathy patients (P<0.05). The positive rates of glomerular PLA2R and IgG4 depositions and circulating anti-PLA2R antibodies in membranous nephropathy patients with cancer were significantly lower than those in idiopathic membranous nephropathy patients without cancer (P<0.01).
Conclusion:
The absence of glomerular PLA2R deposition and negative circulating anti-PLA2R antibodies, along with negative glomerular IgG4 staining, may be useful clues to more accurately screen underlying malignancies in membranous nephropathy patients.
Keywords
Introduction
Membranous nephropathy (MN) is a characterized by thickened glomerular capillary walls due to subepithelial deposits, which may be idiopathic or secondary to various other diseases. The association of nephrotic syndrome (NS), particularly MN, with malignant tumors has been clearly recognized for several decades.1-3 An accurate diagnosis of malignancy-related MN is essential because its treatment is completely different from idiopathic membranous nephropathy (IMN). Moreover, immunosuppressive therapy recommended for IMN may cause or aggravate malignancies. To date, no specific clinicopathological features or biomarkers have been used to distinguish between true malignancy-related MN patients and IMN patients who are only co-occurring with cancer. 4
In 2009, M-type phospholipase A2 receptor (PLA2R) was first identified as the major target antigen involved in IMN. 5 Several studies have shown positive glomerular PLA2R deposition in 70~80% cases of IMN.6,7 Additionally, the IgG4 subclass was demonstrated as the dominant deposition in IMN. The combination of the IgG4 subclass and the PLA2R expression in glomeruli has made it possible to differentiate IMN from secondary MN. 8 Another podocyte antigen, thrombospondin type-1 domain-containing 7A (THSD7A), was recently detected in approximately 10% of PLA2R-negative MN patients, and a higher risk of cancer in patients with THSD7A-associated MN was noted.9,10 The aim of this study was to compare the clinical and pathological characteristics between MN patients with cancer and IMN patients without cancer to better detect malignancy-related MN, including glomerular PLA2R and THSD7A deposition and their circulating autoantibodies, together with glomerular IgG4 deposition.
Methods
Patients and samples
From January 2001 to December 2017, 303 patients with biopsy-proven MN at Xin Hua Hospital were initially selected for review. Among them, 45 were discovered presence of underlying disease including 12 patients with malignancy, 10 with lupus, 22 with hepatitis B virus, and 1 with Sjögren syndrome. We selected 257 IMN patients with excluded secondary causes as the control group. After 1 year of follow-up, all the data will be collected again.
The clinical data for the patients involved in this study were obtained from the medical records of Xin Hua Hospital at the time of renal biopsy, including gender, age, duration of disease, and the presence of hypertension. Laboratory tests were also conducted including urinalysis, proteinuria, serum albumin, serum creatinine, the estimated glomerular filtration rate (eGFR, calculated by The Chronic Kidney Disease Epidemiology Collaboration formula), 11 and serologic testing such as complement levels (C3 and C4), autoantibodies (ANA), hepatitis B/C surface antigen, syphilis serology, and tumor markers (AFP, CEA, PSA, CA 15-3, CA 19-9). Oncological screening, such as chest computed tomography, gastroscopy, colonoscopy, gynecological examination, and mammography, was performed in patients older than 50 years.
This study was approved by the Institutional Review Board of Xin Hua Hospital Affiliated to Shanghai Jiao Tong University School of Medicine. All study-related procedures were performed according to the Declaration of Helsinki.
Routine renal pathological examinations
Paraffin-embedded tissues for light microscopy were routinely sectioned at 3 μm, followed by hematoxylin and eosin, Jones methenamine silver, Masson trichrome, and periodic acid-Schiff staining. The samples were snap frozen in liquid nitrogen and were cut at 4 μm for immunofluorescence staining, followed by staining for IgG, IgA, IgM, C3, C4, C1q, κ, and λ-light chain. The amount of tubular atrophy and interstitial fibrosis was graded as absent (T0), mild (T1) <25%, moderate (T2) = 25%–50%, or severe (T3) >50% of parenchyma 12 In electron microscopy, Ehrenreich and Churg classification criteria were used for the ultrastructural stage of membranous nephropathy. 13
Glomerular staining of PLA2R, THSD7A, and IgG4
Paraffin-embedded sections of formalin-fixed renal tissue were utilized for immunohistochemistry (IHC) using rabbit polyclonal anti-PLA2R (1:500; Sigma-Aldrich, Germany), rabbit polyclonal anti-THSD7A (1:100; Sigma-Aldrich) and mouse monoclonal anti-IgG4 (1:100; Southern Biotech, Slough, UK) primary antibodies. The glomerular expression of PLA2R, THSD7A, and IgG4 were detected according to the same protocol as reported previously, and the intensity of glomerular THSD7A, PLA2R, and IgG4 expression was assessed using a previously described method.8,14
Circulating anti-PLA2R antibody and anti-THSD7A antibody measurement
Circulating anti-PLA2R antibody was measured using enzyme-linked immunosorbent assay (ELISA) kits (EUROIMMUN Lübeck, Germany) according to the manufacturer’s protocol. 15 The ELISA results were considered negative for levels<20 RU/mL and positive for levels>20 RU/mL. Circulating anti-THSD7A antibody was detected using indirect immunofluorescence test kits (EUROIMMUN AG, Lübeck, Germany). Serum samples were diluted at 1:10 and those positive at 1:10 dilution would be further diluted, following the standard instructions. 16
Definition
MN with cancer was designated by the existence of malignancy discovered simultaneously or within 1 year after the diagnosis of MN. IMN was defined as MN without any secondary causes.
Statistical analysis
The data were analyzed using SPSS 17.0 software (SPSS Inc., Chicago, IL). Frequencies were reported for the categorical data. Normally distributed variables were described as the means with standard deviation and skewed continuous data as median and range or interquartile range. Continuous data were compared using the Student’s test for parametric variables or the Mann-Whitney U test for non-parametric variables. Categorical data were compared using χ2 test. All P values were two-tailed, with <0.05 considered statistically significant.
Results
Incidence of cancer among patients with MN at the time of diagnosis or within 1 year after the diagnosis of MN
In our study, the incidence of cancer among patients with MN was 4.0% (12/303), including 8 males and 4 females, with a median age of 66 (range, 39–73) years at the time of diagnosis. One patient with lung cancer found at 14 months after the diagnosis of MN was excluded according to the definition of our study. MN patients older than or equal to 65 years had a higher incidence of malignancies (P=0.02, Table 1).
Incidence of cancer among patients with membranous nephropathy at the time of diagnosis or with 1 year of follow-up.
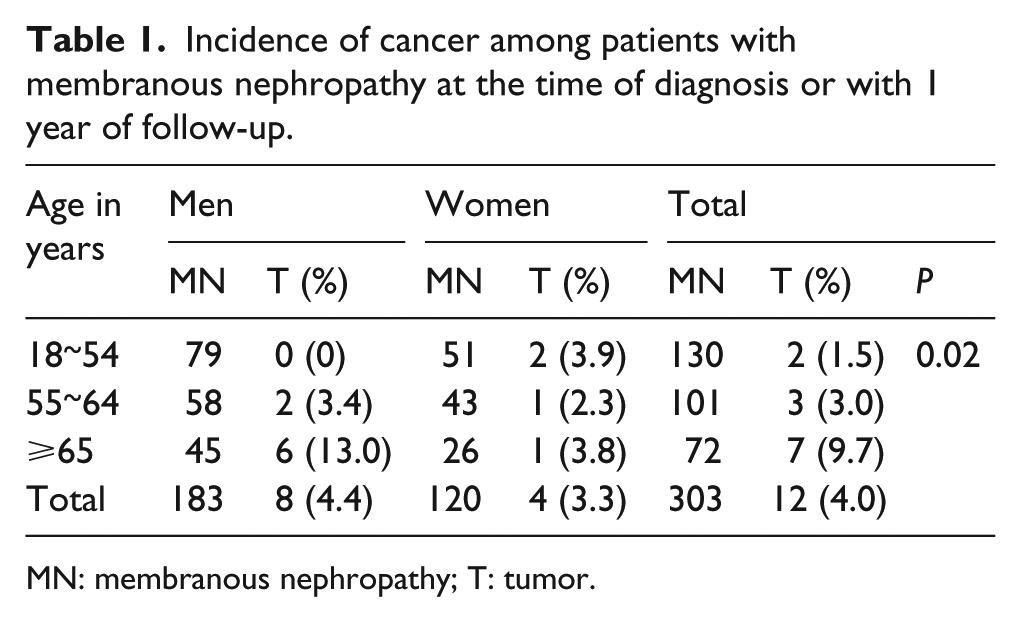
MN: membranous nephropathy; T: tumor.
Profiles of MN patients with cancer
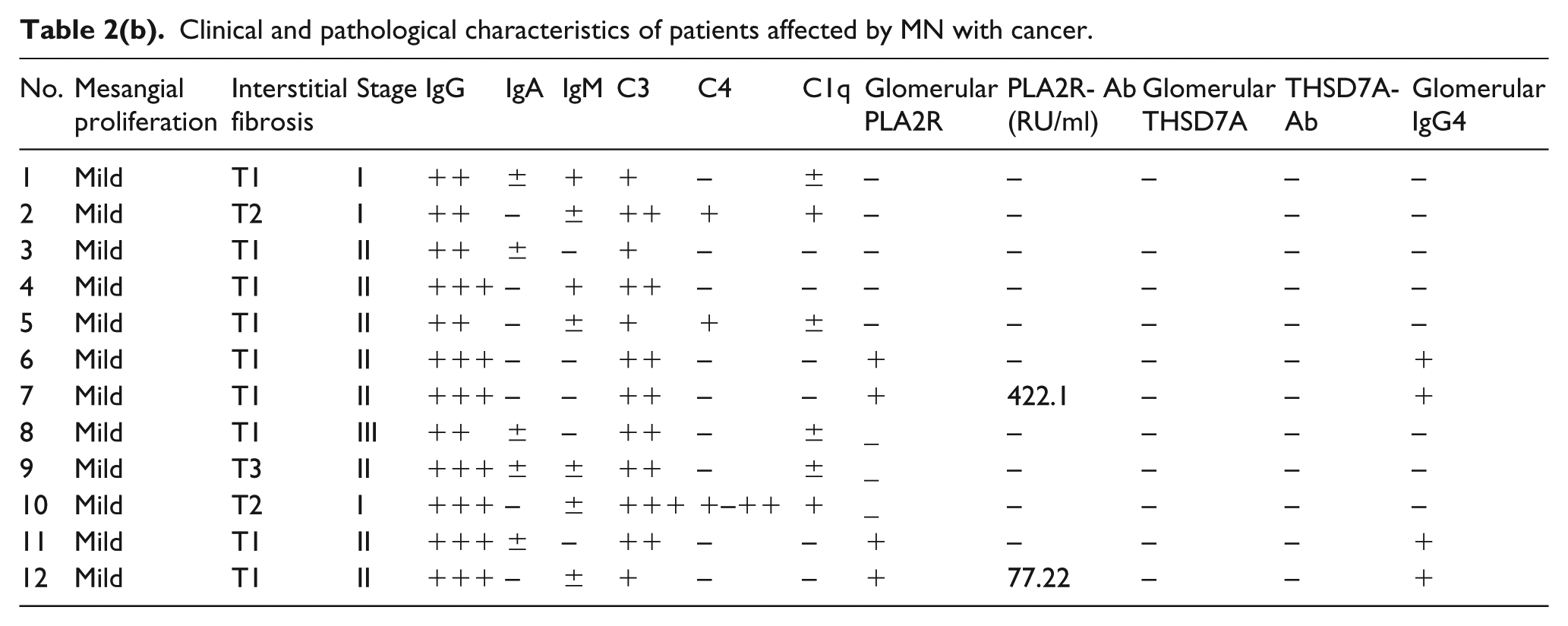
As shown in Table 2, most patients had various types of solid tumors. Lung cancer was the most common accompanying malignancy, accounting for five cases. One case with thyroid cancer and another case with stomach cancer were discovered at the time of MN relapse. Ten cases were those of tumors found at the time of MN diagnosis or within 1 year from the diagnosis. The median duration from the diagnosis of MN to cancer discovery was 3 months (range, 0–12 months).
Clinical and pathological characteristics of patients affected by MN with cancer.
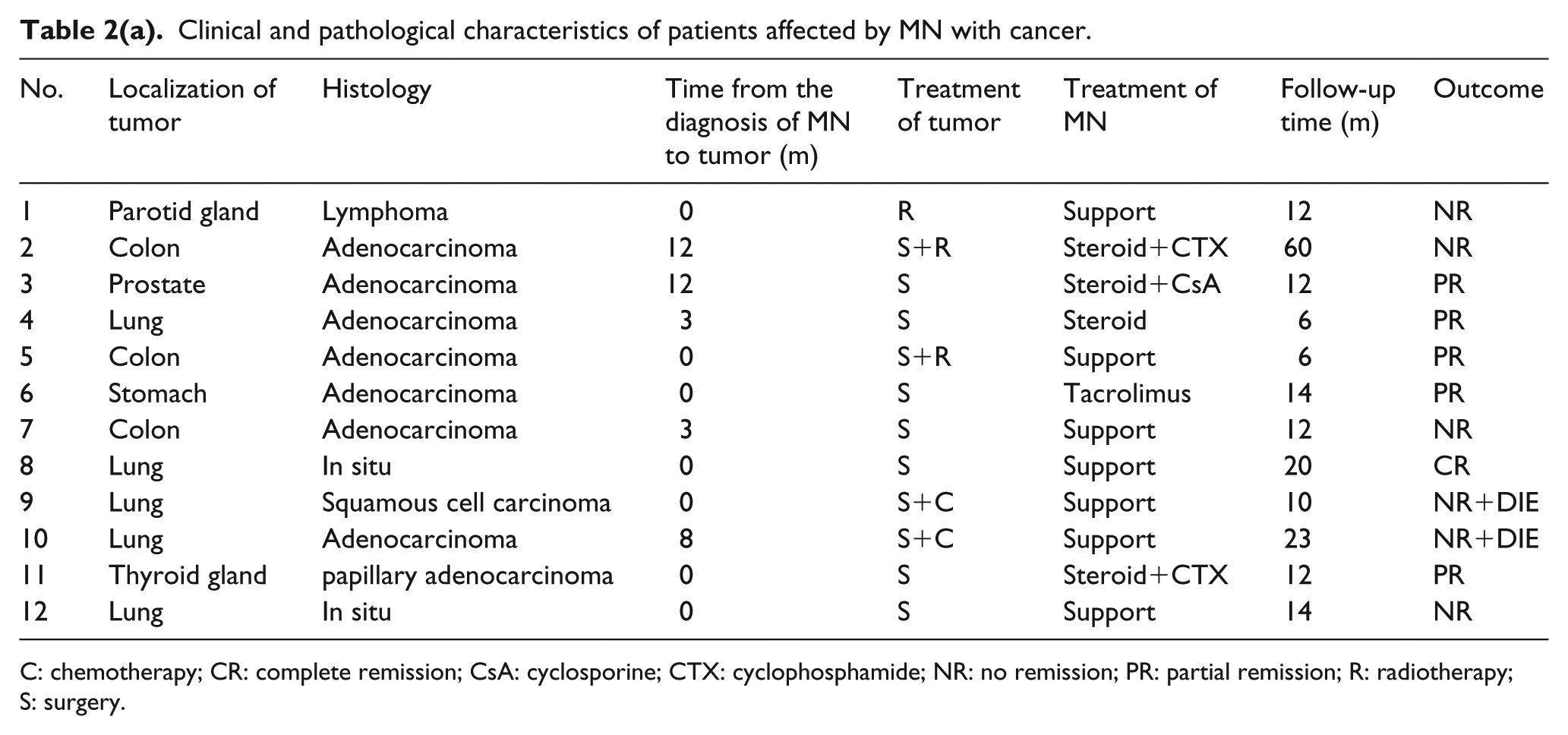
C: chemotherapy; CR: complete remission; CsA: cyclosporine; CTX: cyclophosphamide; NR: no remission; PR: partial remission; R: radiotherapy; S: surgery.
Clinical and pathological characteristics of patients affected by MN with cancer.
Only three patients presented tumor-related symptoms at the time of renal biopsy. Two showed cough and hemoptysis, and one had a mass in the neck. There were no abnormal tumor biomarkers found in all patients. Five of 12 patients were smokers.
Comparison of the clinicopathological features between MN with cancer and IMN without cancer
The clinical and histological findings between MN patients with cancer and IMN patients without cancer are presented in Table 3. MN patients with cancer were significantly older than IMN patients without cancer (P=0.01), and had significantly higher serum creatinine and lower eGFR (P=0.01). Although MN patients with cancer showed higher proteinuria and lower serum albumin levels, no significant difference was found between the groups. Pathological parameters, such as the proportion of chronic interstitial fibrosis, were similar in these two groups. Also, there was no difference found in the staging of MN.
Comparison of the clinical and pathological features between MN with and IMN without cancer.
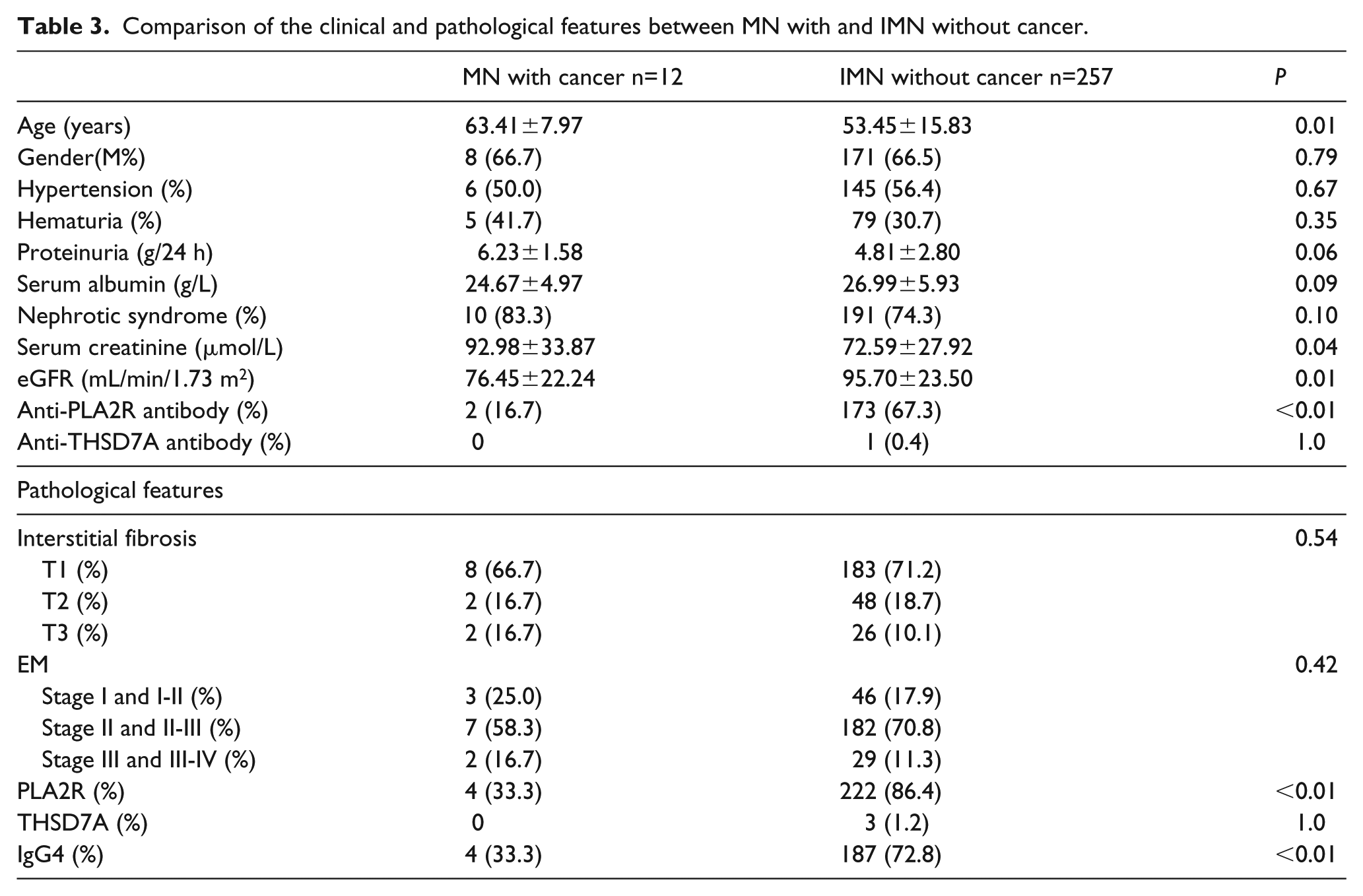
The positive rates of glomerular PLA2R and IgG4 staining (Figure 1) and circulating anti-PLA2R antibodies were significantly lower in MN patients with cancer than in IMN patients without cancer (P <0.01). However, no significant difference was found in glomerular THSD7A staining (Figure 1) and circulating anti-THSD7A antibodies due to the very low positive rate in both groups (Table 3).
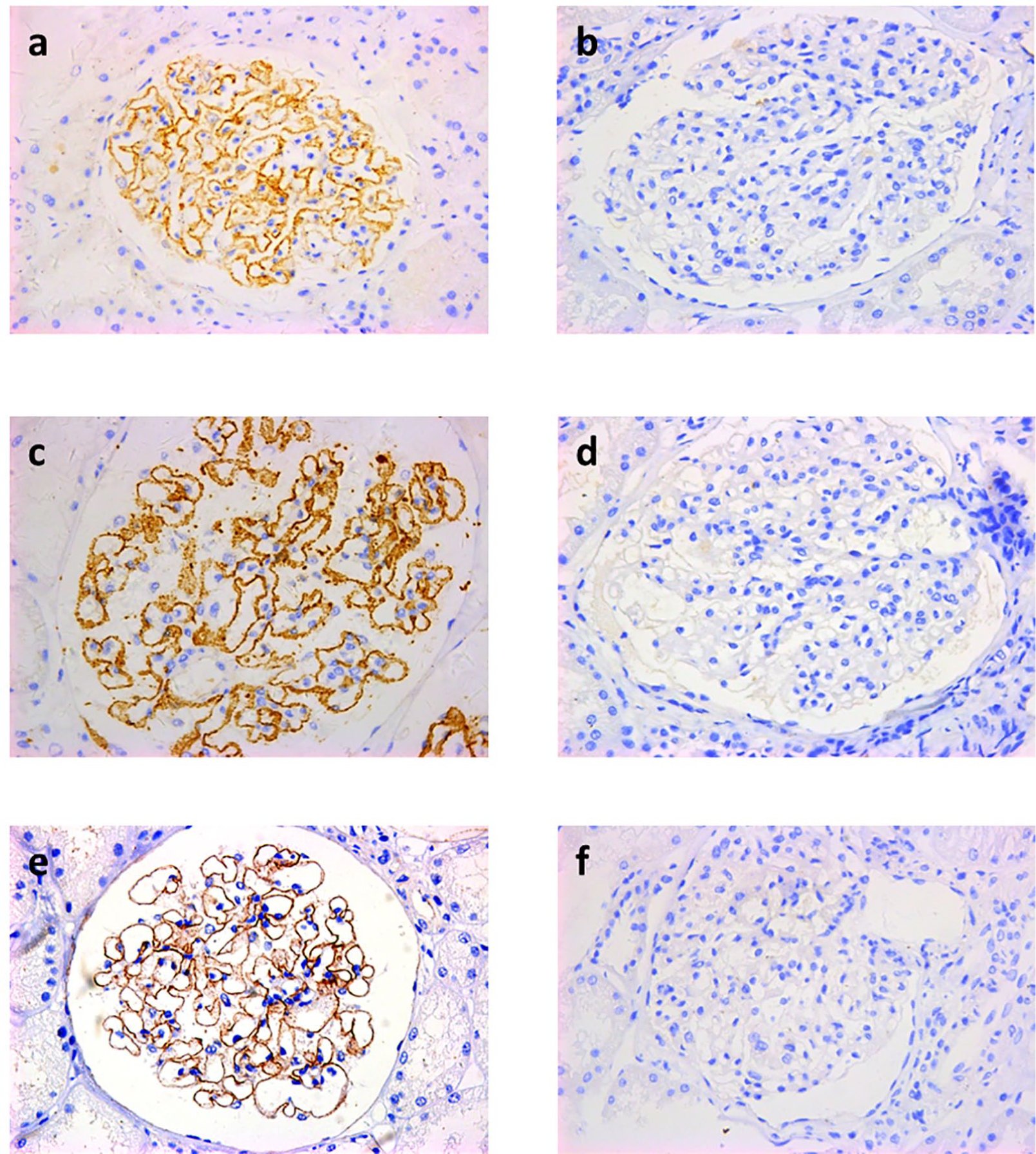
Glomerular staining of PLA2R, THSD7A and IgG4 in membranous nephropathy. PLA2R, THSD7A, and IgG4 were detected as granular deposits in the sub-epithelial space ((a), (c), and (e); magnification ×400). Staining in renal biopsy tissues of patients with minimal change disease were used as controls ((b), (d), and (f); magnification ×400).
Follow-up of the MN patients with malignancy
As shown in Table 2, in two patients with both glomerular PLA2R and IgG4 depositions and elevated circulating anti-PLA2R antibodies (Nos. 7 and 12), proteinuria was not reduced within 1 year after tumor resection. However, another two patients (Nos. 6 and 11) with only glomerular PLA2R and IgG4 depositions but no elevated antibodies showed malignancy at the time of MN relapse. They both achieved partial remission after tumor resection and immunosuppressive therapy for MN.
Of the eight cases without glomerular PLA2R staining, four (Nos. 3, 4, 5, and 8) resulted in remission after tumor excision, including one with prostate cancer, one with colon cancer, and two with lung cancer. One case with colon cancer and one case with lymphoma of the parotid gland (Nos. 1 and 2) showed transient improvement of NS but did not achieve complete remission. In the remaining two patients with lung cancer (Nos. 9 and 10), proteinuria persisted or worsened due to multiple metastasis during follow-up, and the patients later died of malignancy.
Discussion
In this study, we found that the positive rates of glomerular PLA2R and IgG4 depositions and circulating anti-PLA2R antibodies in MN patients with cancer were significantly lower than those in IMN patients without cancer. We also found that MN patients with cancer exhibited clinical characteristics including higher serum creatinine and lower eGFR.
MN is the most common glomerular disease associated with cancer and the most frequent form of nephrotic syndrome in elderly patients.2,3 A series of previous studies was inconsistent in the percentage of cancers in MN patients, as summarized in Supplementary Table 1.17-30 The incidence of cancer shown in this study was similar to that of another Chinese cohort, 28 but was lower than that reported in other countries. This discrepancy may be explained by the differences in genetic background or environmental conditions. Other factors, such as the age of subjects and cancer-screening ability of different medical institutions also may have some influences. Additionally, because some cancers occur after the diagnosis of MN, regular and careful follow-up is also necessary. It was reported that approximately 40% of malignant tumors were found simultaneously at the diagnosis of MN, while more than 40% of tumors presented after the MN diagnosis. 3 In the present study, malignancies were discovered either at the MN diagnosis or during the follow-up after the diagnosis, a finding that was consistent with other results. Latent tumors accompanied by MN usually become apparent within 1 year. However, one study showed that the risk of cancer in patients with MN continued even many years after the MN diagnosis, 27 suggesting that a long-term follow-up may be necessary if cancers cannot be detected initially.
Lung cancer is considered as the most common accompanying malignancy in MN patients followed by gastrointestinal tract cancer and prostate cancer. In this study, the most frequent solid tumor in MN patients was also lung cancer, as shown in Table 2. Lefaucheur et al. 26 found that all MN patients with cancer had nephrotic-range proteinuria, while other studies showed that one-third of MN patients with cancer had non-nephrotic proteinuria at the time of the MN diagnosis. 27 Similarly, our study showed that 2 of 12 MN patients with cancer had mild proteinuria, indicating that even MN patients with non-nephrotic proteinuria also should be screened for cancer at the time of diagnosis or during the follow-up.
A previous study suggested that two clinical characteristics were associated with a higher risk of malignancy in MN patients: age older than 65 years and heavy smoking. 26 Additionally, some pathological features could be clues to screen malignancy, including a higher number of inflammatory cells infiltrating glomeruli (more than eight cells per glomerulus) and the presence of mesangial electron-dense deposits. 26 Our study demonstrated that the mean age of MN patients with cancer was significantly older than that of IMN without cancer, and the incidence of malignancy was much higher in MN patients older than or equal to 65 years. These findings confirmed previous studies that age was closely related to the occurrence of cancer in MN patients. However, we found no discrepancy in terms of renal morphology between the groups. Further studies with larger samples are needed. It is worth noting that the relationship between malignancy and MN may be overstated because of the increased incidence of cancer among the elderly in the general population. Moreover, MN patients may be monitored more closely than the general population, increasing the possibility of detecting asymptomatic cancer. 31
In 2009, Beck et al. 5 first confirmed PLA2R as a major antigen in IMN, while PLA2R was seldom detected in secondary MN. Next, many subsequent studies found that glomerular PLA2R deposition or circulating anti-PLA2R antibodies were also presented in a few cases of malignancy-related MN as shown in Supplementary Table 2.8,16,32-42 Glomerular IgG4 staining could also be observed in some of these patients. 32 However, other studies have suggested that glomerular IgG4 deposition was not associated with malignancy-related MN.14,43 In our study, glomerular PLA2R staining was positive in four MN patients with cancer, along with glomerular IgG4 depositions simultaneously, while glomerular PLA2R and IgG4 staining was negative in other MN patients with cancer. Furthermore, we noticed that among the four MN patients with cancer having glomerular PLA2R depositions, two showed no remission of NS after tumor excision, and another two showed malignancy at the time of MN relapse, suggesting that the coincidence between MN and cancer could not be ruled out in these cases.
Since the discovery of a new autoantigen, THSD7A, in MN, 9 some studies have found a higher incidence of cancer (approximately 20%) in patients with THSD7A-associated MN, whereas other studies have found a relatively lower incidence (6~7%) as shown in Supplementary Table 3.10,16,42,44 In this study, neither glomerular THSD7A deposition nor circulating anti-THSD7A antibodies were observed in all 12 MN patients with cancer, suggesting that the relationship of THSD7A-associated MN with malignancy remains controversial. 4
There were some limitations in our study. First, the sample size was relatively small and only from one hospital. Second, because frozen tissues were not available, we investigated glomerular IgG4 staining by IHC using formalin-fixed paraffin-embedded samples.
In conclusion, the absence of glomerular PLA2R deposition and the negative circulating anti-PLA2R antibodies, along with negative glomerular IgG4 staining, may be useful clues to more accurately screen underlying malignancies in MN patients.
Supplemental Material
MN_revised_manuscript_supplementary_08052019 – Supplemental material for Clinicopathological features in membranous nephropathy with cancer: A retrospective single-center study and literature review
Supplemental material, MN_revised_manuscript_supplementary_08052019 for Clinicopathological features in membranous nephropathy with cancer: A retrospective single-center study and literature review by Dan Zhang, Chong Zhang, Fan Bian, Wenzhu Zhang, Gengru Jiang and Jun Zou in The International Journal of Biological Markers
Footnotes
Acknowledgements
We are deeply grateful to all participants in this study. This work was supported by grants from the National Natural Science Foundation of China (grant No.81570634 and No. 81770706).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.