
Abstract
Purpose:
Numerous studies have suggested that dyslipidemia is closely related to various cancers and the high-density lipoprotein cholesterol (HDL-C) levels are associated with the outcome of cancer patients. However, the predictive value of HDL-C in patients with renal cell carcinoma remains unclear. Our study aims to explore the relationship between the levels of serum HDL-C and the prognosis of renal cell carcinoma.
Methods:
A total of 308 patients diagnosed with clear cell renal cell carcinoma (CCRCC) who received surgical treatment were retrospectively enrolled in our study. The necessary clinical data of each enrolled patient were collected and the Kaplan–Meier method and the Cox proportional hazards regression model were used to calculate the overall survival and cancer-specific survival.
Results:
Kaplan–Meier and univariate analysis showed that a lower preoperative serum HDL-C level was a risk factor of CCRCC patients. Multivariate analyses demonstrated that a higher serum HDL-C level was closely associated with better overall survival (hazard ratio = 0.32; 95% confidence interval (0.13, 0.78); P=0.013) and cancer-specific survival (hazard ratio =0.42; 95% confidence interval (0.15, 0.99); P=0.048).
Conclusion:
Our findings suggest that an increased serum level of HDL-C might predict better overall survival and cancer-specific survival in patients with CCRCC.
Introduction
Renal cell carcinoma (RCC) is the most common tumor of the kidney in adults; it accounts for about 3% of adult malignancies, 1 with the highest mortality rate at over 40%. 2 Clear cell renal cell carcinoma (CCRCC) accounts for 70%–80% of all RCC cases, which is the most common pathological subtype. Since both chemotherapy and radiotherapy are not effective methods to treat RCC, the only effective treatment is surgical resection. 3 However, after resection, 20%–40% patients will have neoplasm recurrence. 4 Currently, clinical physicians often use Fuhrman grade 5 and tumor-node-metastasis (TNM) stage 6 to predict the prognosis of patients with RCC. Additionally, other prognostic models (e.g. such as pretreatment neutrophil-to-lymphocyte ratio, 7 C-reactive protein to albumin ratio, 8 albumin to globulin ratio, 9 and positive surgical parenchymal margin 10 ) have been established to evaluate the risks. Due to the insufficiency of these prognostic variables, a novel clinical and laboratory marker is urgently needed to predict the prognosis of these patients.
A metabolic disorder is widely considered to be an important hallmark in many cancers, and the lipid metabolism disorder has been confirmed to play a crucial role in the pathogenesis of cancers.11-13 Numerous studies have found the correlation between serum lipids and various carcinoma, such as esophageal squamous cell carcinoma, 14 breast cancer, 15 renal cell carcinoma, 16 non-small cell lung cancer, 17 and gastric cancer. 18 Wolfe et al. 19 found that in breast cancer patients decreased serum high-density lipoprotein cholesterol (HDL-C) levels predicted a lower 5-year overall survival (OS) rate, and HDL-C can improve the radio sensitivity in breast cancer cells. In addition, serum HDL-C is significantly decreased in various cancer patients,20-23 which suggests a lipid disorder associated with cancers. The accumulation of studies has found that decreased serum HDL-C levels are closely related to the poor outcome of cancer patients, such as hepatocellular carcinoma, 24 gastric cancer, 25 breast cancer, 19 and colorectal cancer. 26 However, a study by Liu et al. 27 reported that pre-treatment high serum HDL-C levels were associated with the poor outcome of nasopharyngeal carcinoma patients via promoting the proliferation and migration of nasopharyngeal carcinoma cells.
However, the association between serum HDL and the outcome of CCRCC have not yet been evaluated. Our study aims to investigate the potential role of the HDL-C on OS and cancer-specific survival (CSS) in CCRCC patients after surgical resections.
Methods
Patients
We retrospectively enrolled 308 patients diagnosed with CCRCC who received surgical treatment in The Third Affiliated Hospital of Soochow University from 2003 to 2012.The inclusion criteria were: (i) CCRCC was histopathologically diagnosed; (ii) patients with radical nephrectomy; (iii) patients without preoperative neoadjuvant therapy; (iv) patients without cancer history; and (v) preoperative laboratory tests were obtained before treatment. After excluding 106 patients, the remaining 308 patients were finally included for analysis. Clinical data were obtained from the patients’ medical records. Written informed consent was obtained from each patient and the study was approved by the local Institute Research Ethics Committee.
Data collection
The necessary clinical data of each enrolled patient were collected as follows: age, sex, Fuhrman grade, tumor size, lymph node metastasis, necrosis of tumor, and lymphovascular invasion. Relevant laboratory indicators were collected before surgery.
Radical nephrectomy
Surgery was performed by several surgeons according to the standard criteria for radical nephrectomy. Open nephrectomy was performed in 147 patients, whereas the remaining 159 patients underwent laparoscopic nephrectomy. This procedure involves the removal of the whole kidney, along with a section of the tube leading to the bladder (ureter), the gland which sits at the top the kidney (adrenal gland), and the fatty tissue around the kidney.
Follow-up assessment
Follow-up was performed through telephone interviews and review of the medical records. The primary endpoint was OS, which was defined as the interval between the date of the resection and the last follow-up or death. The secondary endpoint was CSS, which was calculated from the date of the resection. The survival endpoint was CCRCC-related death or the date of last follow-up. Data for patients who died from other than metastatic disease were censored at the time of death. Patients with locally advanced CCRCC underwent laboratory tests and physical examinations every 6 months in the first 3 years, then annually thereafter. For patients with localized CCRCC, physical examinations and laboratory tests were performed twice in the first year and annually thereafter.
Statistical analysis
The survival curves were established by the Kaplan–Meier method and the log-rank test, which were used to test statistically significant differences. There is no validated cut-off value for HDL-C, and therefore receiver operating characteristic (ROC) curve analysis was performed with OS and CSS as the outcome, and the Youden index was then estimated. 28 The optimal cut-off value is that which allows the prediction of outcome with the best sensitivity and specificity. 29 Thus, the optimal cut-off value of the HDL-C was estimated by ROC curve statistical analyses. The chi-square test was used to evaluate the association between HDL-C levels and clinic pathological parameters. Univariate analysis and multivariate analysis were performed by the Cox proportional hazards model. A P < 0.05 was considered statistically significant in all statistical tests. All statistical analyses were performed using SPSS 22.0 software (IBM Corporation, Armonk, NY, USA).
Results
Patient characteristics
After the eligibility review, 308 patients with CCRCC who underwent radical nephrectomy were enrolled in the present study. The screening process and detailed information are presented in Figure 1. The clinicopathologic information of patients is presented in Table 1. Of the patients, 193 were male and 115 were female; 128 were older than 60 years, and 180 were younger; the median age was 59 (range 27–79) years; the median follow-up time was 60 (range: 1–149) months; by the last follow-up date, 40 patients had died, and 268 were alive. Upon performing ROC analysis, 1.23 mmol/L was used as the cut-off value for HDL-C. The cut-off value for alkaline phosphatase (AKP) was 125 U/L (upper limit of the normal range) and for lactate dehydrogenase (LDH) was 245 U/L (upper limit of the normal range).
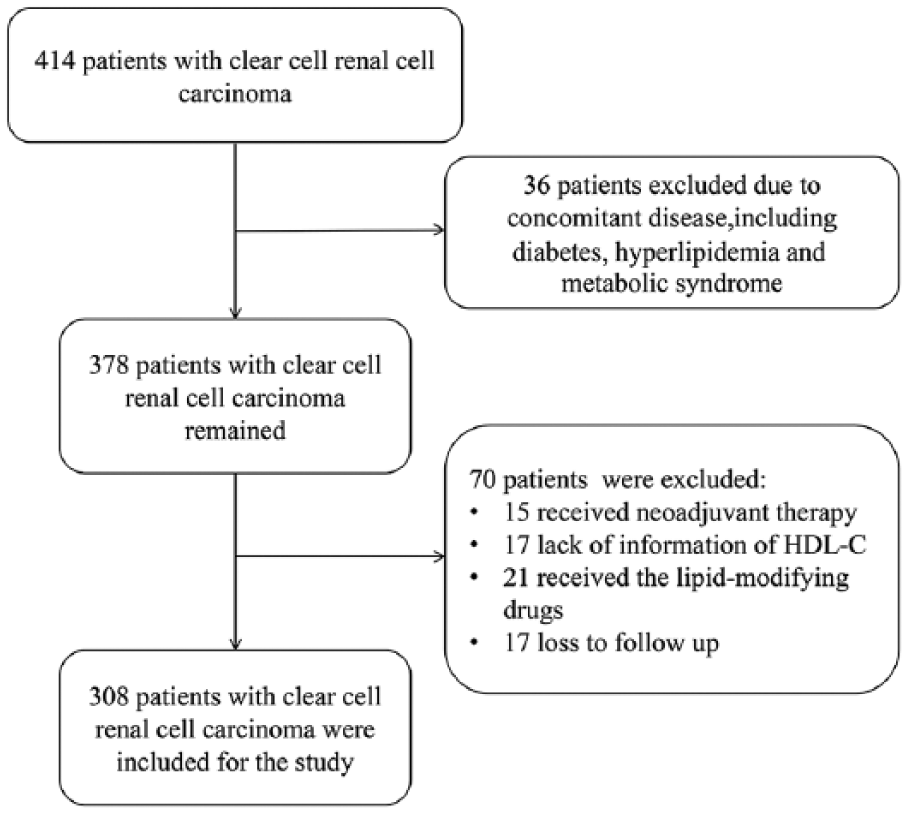
Flow diagram of the study selection process.
The clinicopathological characteristics of patients, and correlation of HDL-C with the clinicopathological characteristics.
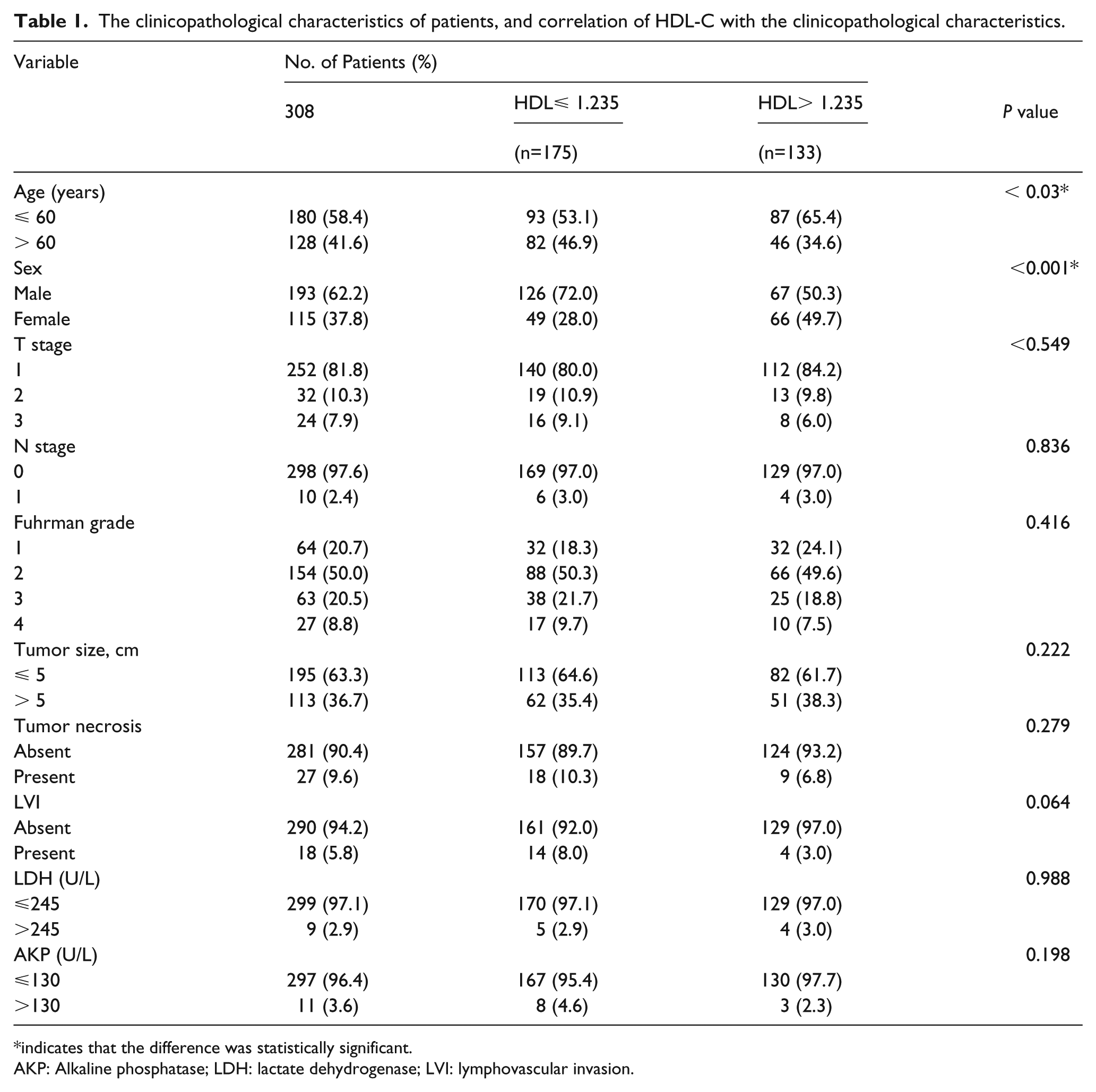
indicates that the difference was statistically significant.
AKP: Alkaline phosphatase; LDH: lactate dehydrogenase; LVI: lymphovascular invasion.
Relationship between the HDL-C levels and other clinical characteristics
Correlations between HDL-C levels and clinicopathological characteristics of the 308 enrolled patients are shown in Table 1. The lower HDL-C level was significantly associated with males (P<0.001) and order age (P=0.03). Other clinicopathological indicators were not closely related to HDL-C levels, including tumor size, tumor stage, lymph node stage, Fuhrman grade, the presence of Tumor necrosis, lymphovascular invasion, LDH, and AKP levels (Table 1).
Prognostic value of HDL-C and clinical characteristics for OS
Among the 308 patients, there were 30 of 175 (17.1%) patients with an HDL-C level ⩽1.23 mmol/L and 10 of 133 (7.5%) patients with an HDL-C level >1.23 mmol/L who had died before the last follow-up date. A higher HDL-C level was closely associated with a better OS (hazard ratio [HR] 0.39; 95% confidence interval [CI] 0.19, 0.80; P=0.01; Table 2). The Kaplan–Meier survival analysis suggested that patients with a high HDL level had a better OS (P=0.008) (Figure 2). As shown in Table 2, according to the results of univariate analysis, other clinicopathological factors—including an order age (P=0.001), an advanced lymph node stage (P<0.001), an advanced T stage (P<0.001), an advanced Fuhrman grade (P<0.001), a larger tumor size (P<0.001), the presence of tumor necrosis (P<0.001), the presence of lymphovascular invasion (P<0.001), a high AKP level (>130 U/L) (P<0.001), and a high LDH level (>245 U/L) (P=0.025)—were significantly associated with poor OS. Based on the results of multivariate analysis, a decreased HDL-C level yielded a worse outcome (HR 0.32; 95% CI 0.13, 0.78; P=0.013; Table 2), which suggested that the level of HDL-C was an independent prognostic factor in patients with CCRCC. In addition, we observed significant associations of age, T stage, and lymph node stage with OS.
Univariate and multivariate Cox proportional analysis with overall survival.
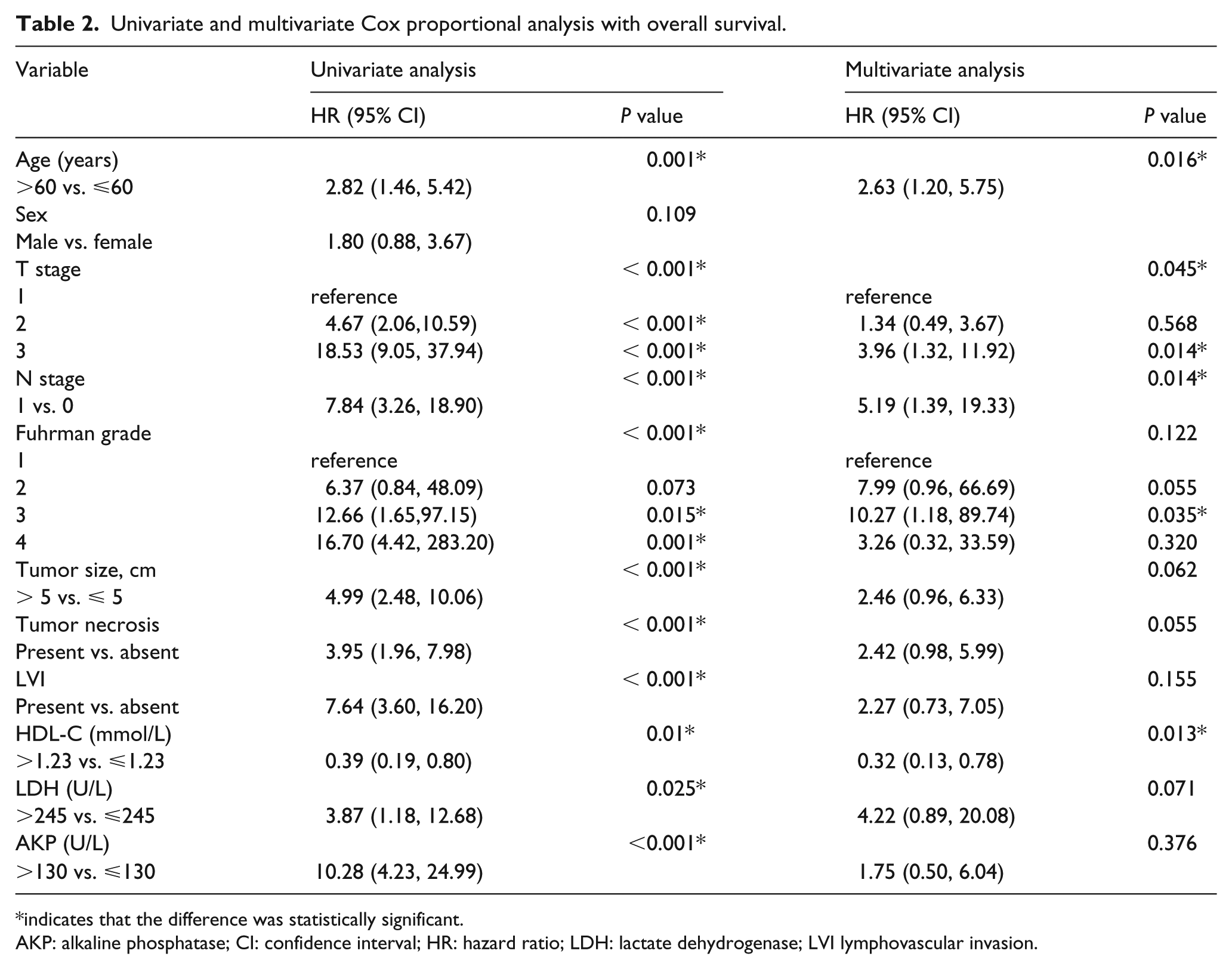
indicates that the difference was statistically significant.
AKP: alkaline phosphatase; CI: confidence interval; HR: hazard ratio; LDH: lactate dehydrogenase; LVI lymphovascular invasion.
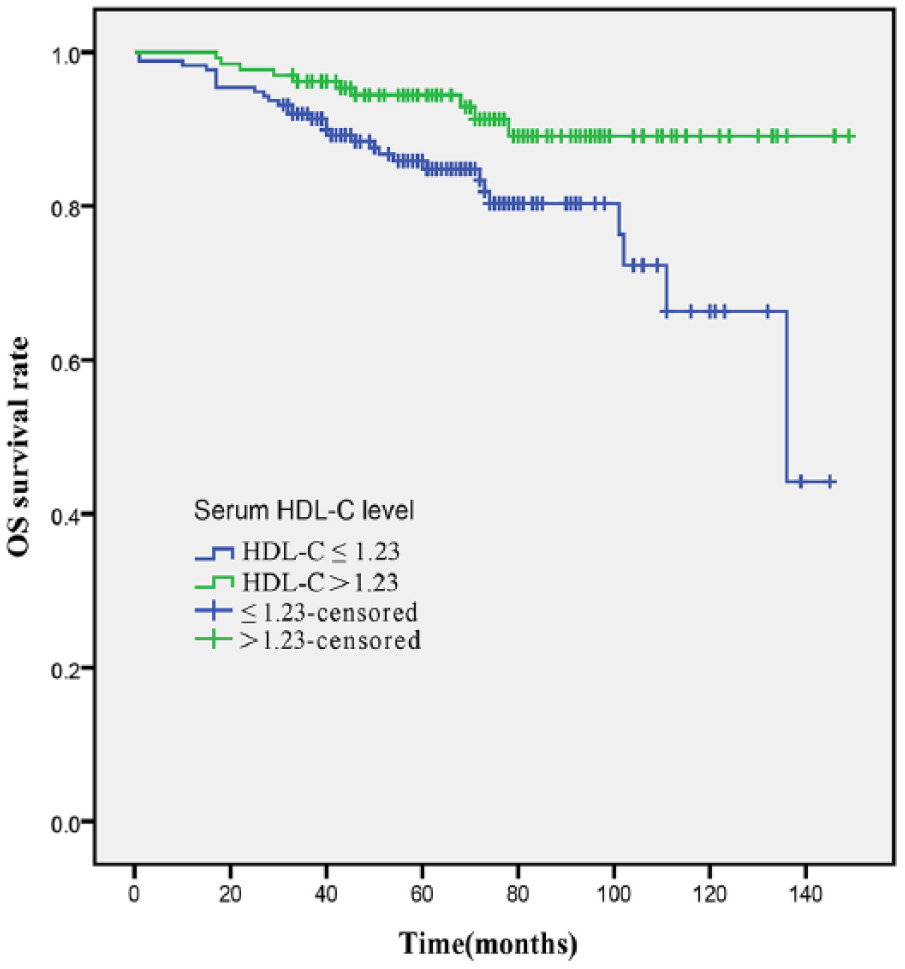
Kaplan–Meier curve for overall survival regarding high versus low HDL-C levels.
Prognostic value of HDL-C and clinical characteristics for CSS
Among the 308 patients, death due to CCRCC occurred in 26 of 175 (14.9%) patients with an HDL-C level ⩽1.23 mmol/L, and 10 of 133 (7.5%) patients with an HDL-C level >1.23 mmol/L at last follow-up date. Regarding CSS, univariate analyses showed that a low HDL-C level was closely associated with a worse CSS (HR 0.37; 95% CI 0.22, 0.95; P=0.017; Table 3). The Kaplan–Meier survival analysis suggested that a decreased HDL level had a better CSS in patients with CCRCC (P=0.03) (Figure 3). In univariate analysis, clinicopathological factors—such as order age (P=0.004), an advanced T stage (P<0.001), an advanced lymph node stage (P<0.001), a larger tumor size (P<0.001), the presence of tumor necrosis (P<0.001), the presence of lymphovascular invasion (P<0.001), a high AKP level (>130 U/L) (P<0.001), and a high LDH level (>245 U/L) (P=0.025)—were related to worse CSS. Multivariate analyses showed that a decreased HDL-C level was statistically linked with decreased CSS (HR 0.42; 95% CI 0.15, 0.99; P=0.048; Table 3). Moreover, age, T stage, N stage, tumor size, and tumor necrosis were independent risk factors for CSS (Table 3).
Univariate and multivariate Cox proportional analysis with cancer-specific survival.
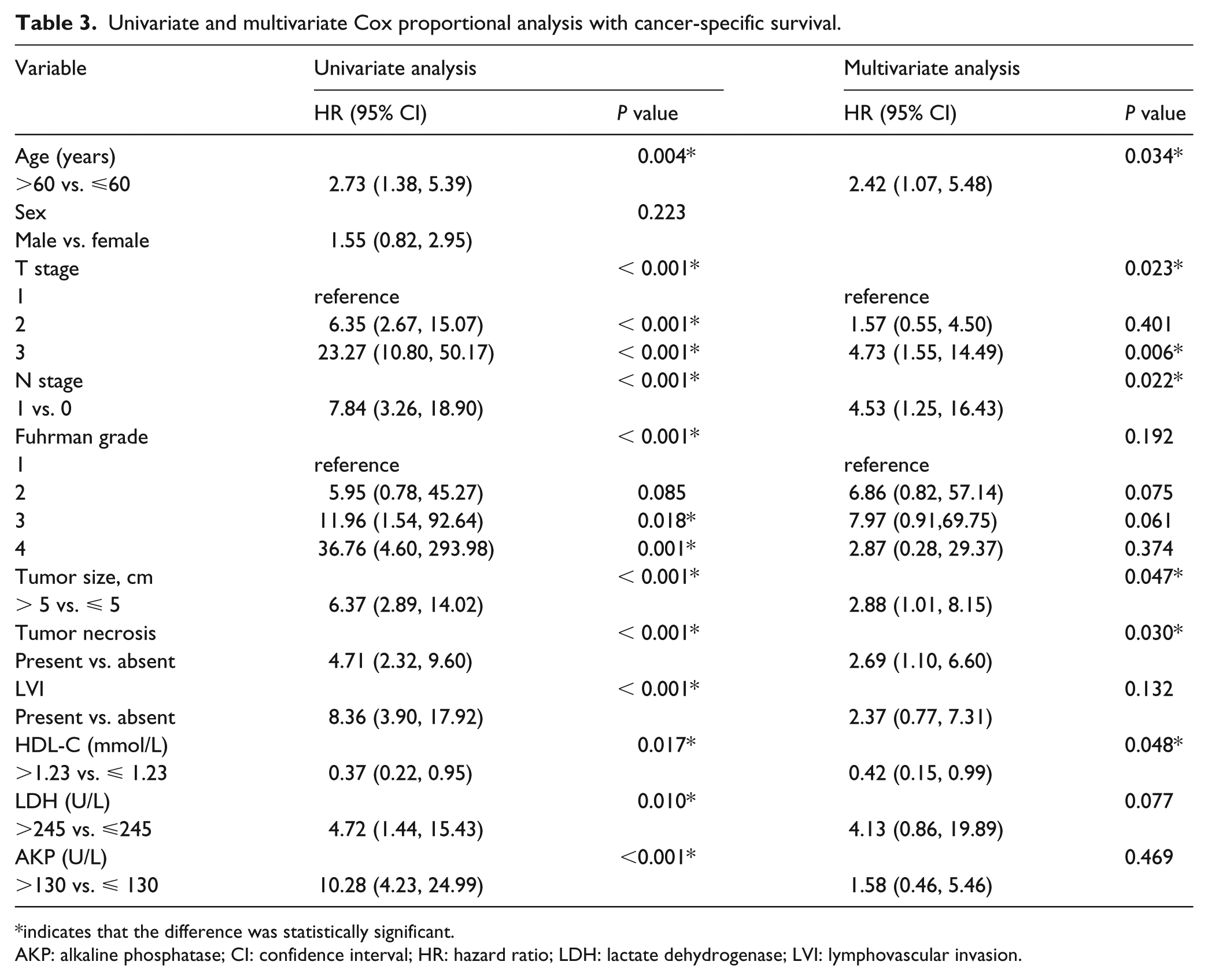
indicates that the difference was statistically significant.
AKP: alkaline phosphatase; CI: confidence interval; HR: hazard ratio; LDH: lactate dehydrogenase; LVI: lymphovascular invasion.
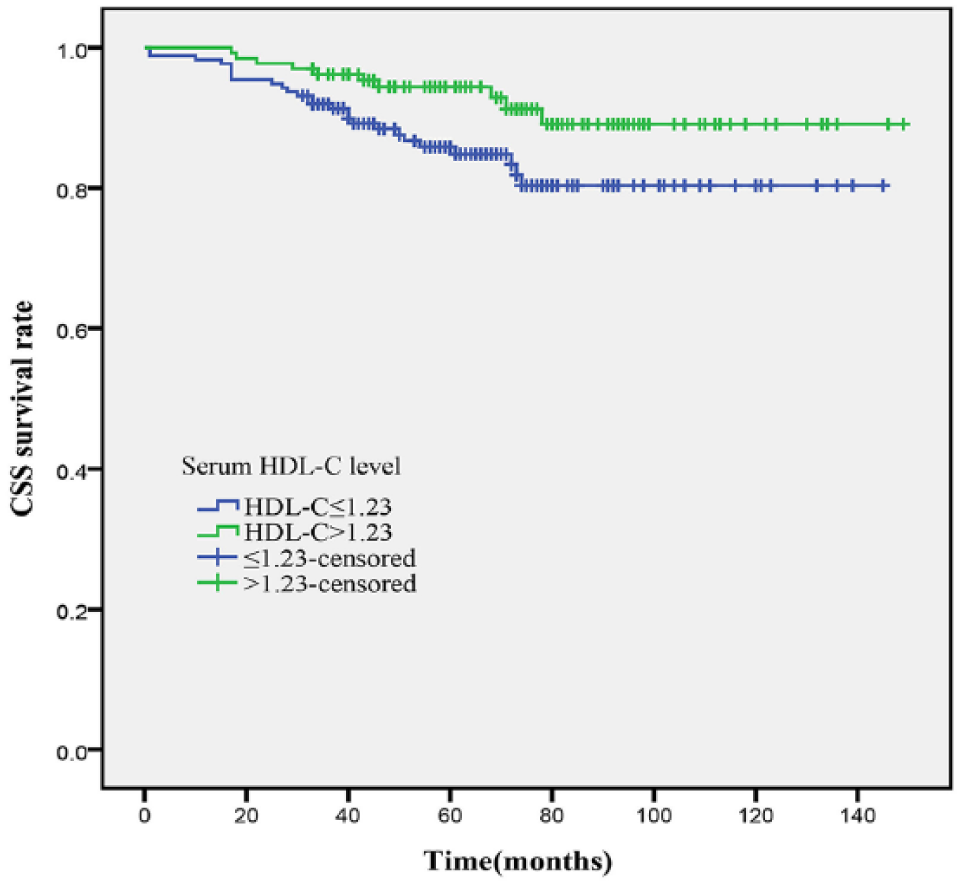
Kaplan–Meier curve for cancer-specific survival regarding high versus low HDL-C levels.
Discussion
Although recent progress has been made in the epigenetic alterations and identification of genetics, 30 the frequently used prognostic evaluation of CCRCC currently depends on pathological factors and traditional clinicopathological prognostic variables. 31 It has been reported that a significant association between a lower HDL-C level and a higher risk of incident cancer in a patient, which was independent of age, gender, body max index, serum LDL-C levels, and the presence of diabetes and smoking. 32 Zhang et al. 22 reported that, compared with the healthy controls, serum HDL-C levels tended to decrease in patients with renal cell cancer. The accumulation of studies has revealed that there was an inverse association between high HDL-C levels and the epidemiology of cancers, including breast cancer, 33 lung cancer, 20 non-Hodgkin lymphoma, 34 and overall cancer risk. 35
To clarify the relationship between HDL-C levels and CCRCC, pathological characteristics and outcome were examined in RCC patients. In the present study, we explored the effect of serum HDL-C levels on the prognosis of patients with CCRCC. Based on the cut-off value of HDL-C before treatment, both the univariate and multivariate analyses showed that a high serum HDL-C was associated with better OS. We showed that high serum HDL-C levels were also a favorable predictor for CSS in CCRCC patients. Consistent with our study, a high serumHDL also can be a favorable predictor in various cancers, such as breast cancer, 33 hepatocellular carcinoma, 24 and gastric cancer. 25
Recently, emerging evidence has shown that HDL-C was linked with the tumorigenesis and progression of cancers.36, 37 Su et al. 37 found that HDL-C reduced the viability and proliferation of colon cancer cells, and HDL-C mimetics could reduce the tumor size of colon cancer in a mouse model. Wolfe et al. 19 held that HDL-C decreased mammosphere formation and suppressed the survival via inhibiting the phosphorylation of epidermal growth factor receptor (EGFR), Akt, and forkhead box O3 (FOXO3a) in breast cancer cell lines. Sekine et al. 38 demonstrated that HDL-C promoted cell proliferation and migration in androgen-independent prostate cancer cells through the ABCA1/ERK1/2/Akt signaling pathway, whereas HDL-C had no such effects on androgen-dependent prostate cancer cells. A study by Liu et al. 27 reported that HDL-C could increase proliferation, invasion, and colony formation of nasopharyngeal carcinoma cells by a mechanism involving scavenger receptor class B member I. Thus, the exact mechanisms underlying the role that HDL-C plays in the development of tumors remain unclear. HDL-C may exert diverse effects on different tumors depending on the receptors that the tumors express.
Cholesterol plays a crucial role in membrane integrity and accumulates in discrete regions of the membrane (termed lipid rafts), which are involved in signaling cascades that were associated with cancer development.39, 40 EGFR, which is known to be closely related to tumorigenesis, can be activated by cholesterol-mediated lipid rafts in the membrane. 41 HDL-C, which plays a key role in the process of reverse cholesterol transport, removed cholesterol from peripheral tissues and transported it to the liver for metabolism. 42 HDL-C removed excess cholesterol from an intracellular pool to maintain the cholesterol homeostasis in normal cells. 43 The explanation for the reduced HDL-C level in RCC patients may be that an increasing consumption and storage of cholesterol within tumor tissues during growth resulted in lower HDL levels in proliferating tissues. We speculated that HDL-C may remove the cholesterol from tumor cells to inhibit the formation of tumor cell membranes and cholesterol-mediated lipid rafts. Numerous studies have demonstrated that high serum HDL levels are associated with a decreased risk of cancers, including colon cancer, 44 breast cancer, 45 and prostate cancer. 46 As a result, lipoprotein treatment may be a promising anti-tumor agent in patients with a low serum HDL-C level; therefore, combination therapies of HDL-C-increasing agents with targeted therapies may improve the clinical outcome of RCC patients.
There are some limitations in the present study. First, the number of patients enrolled in our study was relatively small; second, our research was a retrospective study from a single center; third, our findings need to be confirmed in future studies from multiple centers.
Conclusion
Our results suggest that the serum HDL-C levels are a significant predictive factor in patients with CCRCC. Furthermore, the development of HDL-C-increasing agents may be a promising therapeutic strategy for RCC patients.
Footnotes
Author contributions
Bo Hao, Xufeng Peng, and Baochen Bi contributed equally to this work.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Written informed consent was obtained from each patient and the study was approved by the Ethics Committee of the Third Affiliated Hospital of Soochow University.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.