
Abstract
Introduction:
Altered expression of many E2F family members have been reported in various human cancers. In this study, we investigated the role of non-synonymous single nucleotide polymorphisms (rs3213172 C/T, rs3213173 C/T, and rs3213176 G/A) of the gene E2F1 with cervical cancer.
Methods:
A total of 181 samples including 90 cervical cancer patients and 91 healthy controls were genotyped. The genotype frequencies of these polymorphisms in collected samples were determined by either PCR-RFLP or PCR-ARFLP methods. SHEsis software was used to analyze the haplotypes.
Results:
Statistically significant differences in the alleles and the genotypes frequencies were observed in rs3213172 (C/T) and rs3213173 (C/T) polymorphisms. The rs3213172 (C/T) polymorphism was a risk factor for cervical cancer in dominant model (odds ratio (OR) 1.96; 95% confidence interval (CI) 1.07, 3.60; P = 0.02) and heterozygous model (OR 1.90; 95% CI 1.01, 3.57; P = 0.04). The rs3213173 (C/T) polymorphism increased the risk of cervical cancer in the homozygous model (OR 2.71; 95% CI 1.11, 6.58; P = 0.02). The rs3213176 (G/A) polymorphism was not associated with cervical cancer risk in any of the genotypic models. In the haplotypes analysis, three haplotypes (CTG, TCG, and TTA) were associated with the cervical cancer risk.
Conclusions:
These findings revealed that rs3213172 (C/T) and rs3213173 (C/T) polymorphisms and haplotypes (CTG, TCG, and TTA) of the E2F1 gene might play role in the susceptibility of cervical cancer. This is the first report showing an association of these polymorphisms with the cervical cancer risk.
Introduction
Worldwide, the fourth most common cancer in women is cervical cancer. The prevalence of this cancer is high especially in developing countries. 1 In India, cervical cancer is the second most common cancer among Indian women. 1 Infection with high-risk papilloma virus (HR-HPV) is a major etiological agent of this cancer.2,3 Sexually active women (~15–40%) have an infection with HR-HPV and most of these women resolve this infection, but in some cases it leads to persistent infection.4,5 Persistent HPV infection leads to squamous cell carcinoma (SCC), and infection with this virus has been reported in almost all cases of SCC of cervical cancer. 6 Apart from HR-HPV infection, other risk factors identified are social status, tobacco consumption, use of oral contraceptive, age, and environmental pollutants.7,8 Moreover, there are data indicating that along with various risk factors discussed above, the genetic background of an individual also contributes to the development of cervical malignancies.7–10
The tumor suppressor proteins retinoblastoma (pRB) and p53 are inactivated during higher expression of E6/E7 HPV oncoproteins and result in uncontrolled cell proliferation, increased cell survival, oxidative stress and DNA damage.11,12 E2F1-cyclinA complex is also one of the important controllers of cellular proliferation. The cervical cancer cell line (Caski cells) expressing high levels of HPV-16 E7 protein has been demonstrated to possess a complex of E2F1-cyclin A and E7. The latter might play an important role in E7-mediated transformation. 13 Moreover, E7 and E2F1 directly interact with the DNA and activate E2F1-mediated transcription. The E2F1 binds strongly to E7 of high-risk group HPV compared to low-risk group HPV and it strongly activates transcription of its downstream genes involved in cell cycle control. This further supports the role of E2F1 in HR-HPV E7-mediated cell transformation. 14
E2F1 exhibits a double-edged role in tumor development, with both oncogenic and tumor-suppressive activities. 15 Higher-expression of E2F1 potentially induces cell transformation, and E2F1 transgenic mice were more likely to develop cancer. 16 It also induces apoptosis via both p53-dependent and p53-independent pathways. 17 A recent study revealed that the expression level of E2F1is a key determinant of cell fate. Low levels of E2F1 are enough to induce various cell cycle-promoting genes, intermediate levels induce growth arrest genes (i.e. p18, p19, and p27), while elevated levels of E2F1 are necessary to induce the cell death by increasing the expression of apoptosis inducing key genes APAF1, PUMA, HRK, and BIM. 18
Moreover, single nucleotide polymorphisms in several genes have been shown to be an important factor in the susceptibility to various diseases.19-21 Keeping in view the cell-cycle regulatory functions of E2F1 gene, we hypothesized that these genetic variants (present in the functional domain of E2F1) might alter either the binding affinity of the E7 protein to E2F1 or interactions of E2F1 to its partners involved in cell cycle progression or apoptosis and these altered interactions may lead to a different susceptibility to cervical cancer.
In this study, we analyzed three nsSNPs (rs3213172 C/T (Arg 252 His), rs3213173 C/T (Val 276 Met), and rs3213176 G/A (Gly 393 Ser)) of E2F1 gene as risk factor for cervical cancer in Indian women. These amino acid variants are present in the marked box domain and an adjacent region of this protein. The binding affinity of these amino acid variants might be different in various variants of E6/E7 viral proteins because these variants are located in the high binding affinity region of the E2F1 protein and may play a role in the different susceptibility of individuals to cervical cancer. 14 Furthermore, the National Institute of Environmental Health Sciences (NIEHS) SNPs program also identified these nsSNPs as a disease risk.
Material and methods
Selection of SNPs
In this study, we included three nsSNPs of E2F1 gene rs3213172, rs3213173, and rs3213176 for a case-control association study. These nsSNPs have been predicted to play a role in the disease risk by the NIEHS SNPs program. The rs3213172 is highly damaging at the sequence, the structural, and the molecular dynamics simulation analysis (data not shown).
Study population
We recruited total 181 individuals including 90 cervical cancer patients with a known cancer stage of cervical tumor type, and 91 cancer-free healthy female controls, from July 2013 to November 2015. All of the cervical cancer patients had squamous cell carcinoma. The staging of the cervical cancer was done following the FIGO staging systems given by International Federation of Gynecology and Obstetrics. Patients gave their history and informed consents. The mean age of cases and controls were 55±8 years and 52±9 years, respectively, and were not statistically different (P<0.05). All the patients and the controls included in the study were from North India. The study was approved by the Institutional Ethical Committee of Jaypee University of Information Technology, Solan, Himachal Pradesh, India.
DNA isolation and genotyping
Genomic DNA was isolated from all the collected blood samples following a simple salting out method.
22
As a natural restriction site was not present to perform PCR-RFLP for the rs3213172 and rs3213173, we developed an artificial-restriction fragment length polymorphism (A-RFLP) methods following the strategy described earlier.23,24 The genotyping of rs3213172 was done following A-RFLP. The forward primer 5′
Genomic DNA (40 ng) was amplified by polymerase chain reaction (PCR) in a total volume of 25 μl that contained 0.16 mM of each primer and 12.5 μl green master mix (Promega). PCR amplification was performed following cycling parameters: initial denaturation at 94ºC for 3 minutes, followed by 35 cycles of denaturation at 94ºC for 40 seconds, annealing at 59ºC (rs3213172), 58ºC (rs3213173), and 59ºC (rs3213176) for 40 seconds and extension for 1 minute at 72ºC followed by a final extension at 72ºC for 5 minutes. The amplified PCR products were checked by 2% agarose gel electrophoresis. The amplified PCR products were digested with the respective restriction enzyme (MspI for rs3213173 and rs3213176 SNPs; RsaI for rs3213172) for detection of the genotype of the sample. The digested PCR products were resolved on 3% agarose gel electrophoresis and analyzed.
Statistical analyses
Genotypes and alleles frequencies of cervical cancer patients and healthy controls were determined. These frequencies in the cancer patients were compared with the healthy controls. Odds ratio (OR) and 95% confidence interval (CI) were calculated applying multiple logistic regression analysis to assess the association between rs3213172, rs3213173, and rs3213176 polymorphisms of E2F1 gene with the risk of cervical cancer and clinicopathological features of the patients. All statistical tests were two
Results
Distribution of alleles
All the polymorphisms included in this study (rs3213172, rs3213173, and rs3213176) were in HWE equilibrium (P>0.05). The frequency of T allele of rs3213172 (C/T) polymorphism was 30.22% and 40.56% in controls and cervical cancer patients, respectively. Data suggested that T allele was a genetic risk factor for cervical cancer (OR 1.57; 95% CI 1.02, 2.43) in our population. Polymorphism rs3213173 (C/T) was also associated with cervical cancer risk (OR 1.64; 95% CI 1.05, 2.55) with the T allele frequencies of 27.47% and 38.33% in controls and cervical cancer patients, respectively. Allele frequencies were not significantly associated with cervical cancer risk in rs3213176 (G/A) polymorphism (Table 1).
Genetic association analysis of E2F1 variants with cervical cancer risk.
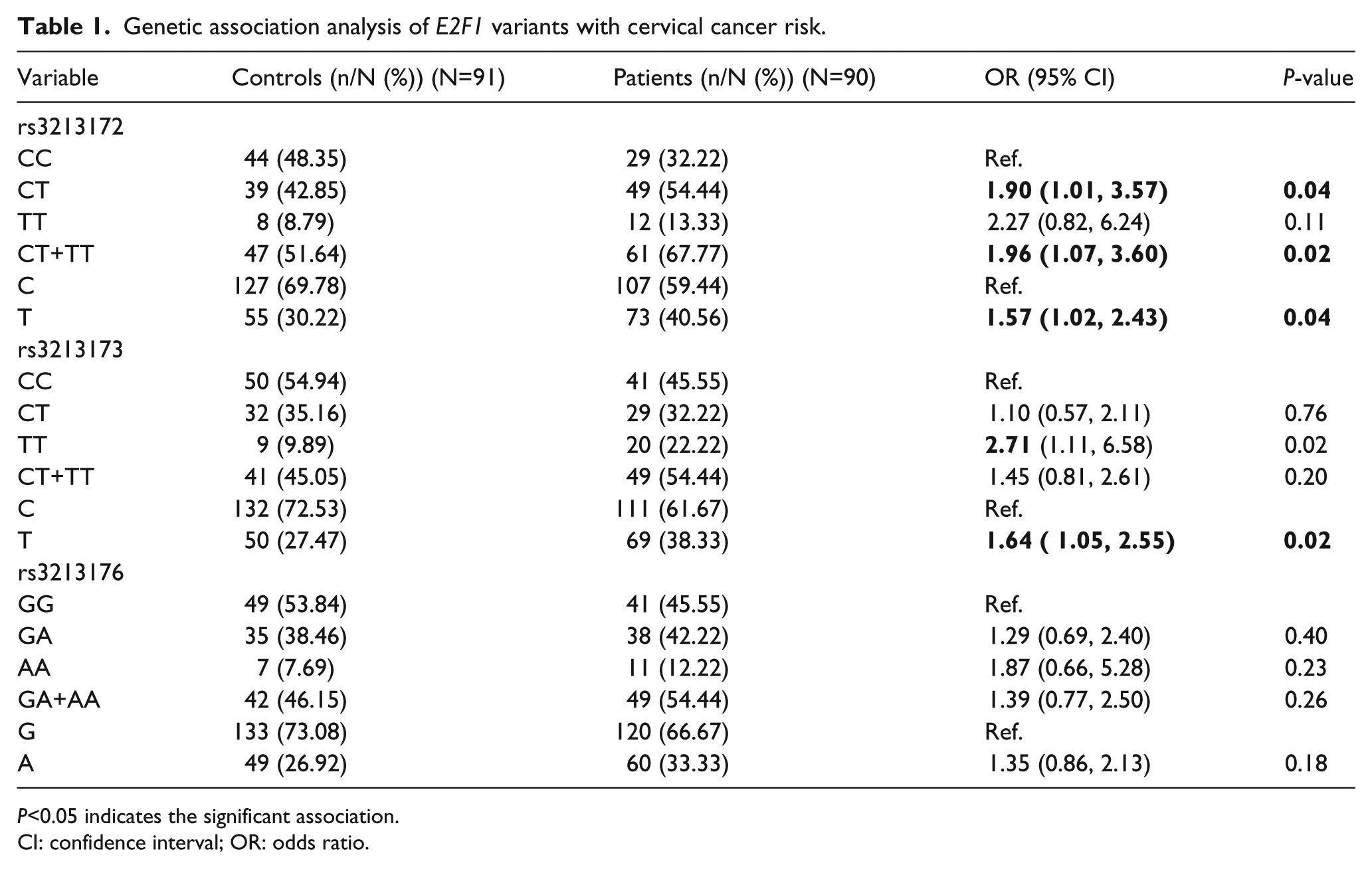
P<0.05 indicates the significant association.
CI: confidence interval; OR: odds ratio.
Distribution of genotypes
The genotype frequencies of wild genotype (CC 48.35%) was higher in controls than in cases (CC 32.22%) for rs3213172, while the frequencies of heterozygous genotype CT (54.44%) and combined mutant genotype CT+TT (67.77%) were higher in the cases than in the controls (Table 1). rs3213172 (C/T) was significantly associated with the cervical cancer risk in heterozygous and dominant models (heterozygous model: CC vs. CT; OR 1.90; 95% CI 1.01, 3.57; P = 0.04; and dominant model: CC vs. CT+TT; OR 1.96; 95% CI 1.07, 3.60; P = 0.02).
The rs3213173 was also associated with cervical cancer risk. The frequency of the mutant genotype TT was 22.22% in cases and 9.89% in controls. The logistic regression analysis showed that in the homozygous model (CC vs. TT) the genotype showed statistically significant association with cervical cancer risk (OR 2.71; 95% CI 1.11, 6.58; P = 0.02) while there was no significant association in the heterozygous model (CC vs. CT; OR 1.10; 95% CI 0.57, 2.11; P = 0.76), and in the dominant model (CC vs. CT+TT; OR 1.45; 95% CI 0.81, 2.61; P = 0.20). The frequency of mutant genotype (AA = 12.22%) was higher in cases than in controls (AA = 7.69%) for rs3213176 but there was no statistically significant difference in any of the genetic models tested for this SNP (Table 1).
Association of genotypes with the tumor stage
To analyze the effect of polymorphisms rs3213172 (C/T), rs3213173 (C/T), and rs3213176 (G/A) on the clinicopathological status (clinical stage), we compared the frequencies of genotypes of these polymorphisms with the clinical stage of cervical cancer. We could not find any significant association of the genotypes with the clinical stage of cervical cancer (stage I+II genotype vs. stage III+Stage IV; Supplementary Table 1).
On comparing the clinical stages of cancer with the healthy individuals, we could not find an increased risk of cancer during the early stages (stages I+II; Supplementary Table 2) while in the late stages (stages III+IV), polymorphisms rs3213172 and rs3213173 were associated with the risk of cervical cancer. The rs3213172 significantly increased the risk of cervical cancer in the heterozygous model (OR 2.33; 95% CI 1.08, 5.04; P = 0.03) and the dominant model (OR 2.34; 95% CI 1.11, 4.92; P = 0.02). The rs3213173 increased the risk of cervical cancer more than three times in the dominant model (OR 3.17; 95% CI 1.16, 8.65; P = 0.02).
Haplotype analysis
SHEsis software was used for haplotypes analysis (Table 2). In the logistic regression analysis of haplotype, we considered the wild CCG haplotype as a reference and compared all the haplotype combinations with CCG and found an interesting result. The haplotypes CTG, TCG, and TTA were associated with cervical cancer risk. The frequencies of CTG, TCG, and TTA were significantly higher in the patients than in the controls (CTG: OR 2.89; 95% CI 1.46, 5.71; P = 0.002; TCG: OR 2.89; 95% CI 1.46, 5.71; P = 0.002; TTA: OR 3.17; 95% CI 1.38, 7.28; P = 0.006). The results indicated that CTG, TCG, and TTA haplotypes might predispose individuals to the risk of cervical cancer.
Haplotype analysis of selected nsSNPs (rs3213172, rs3213173, and rs3213176) of the E2F1 gene.
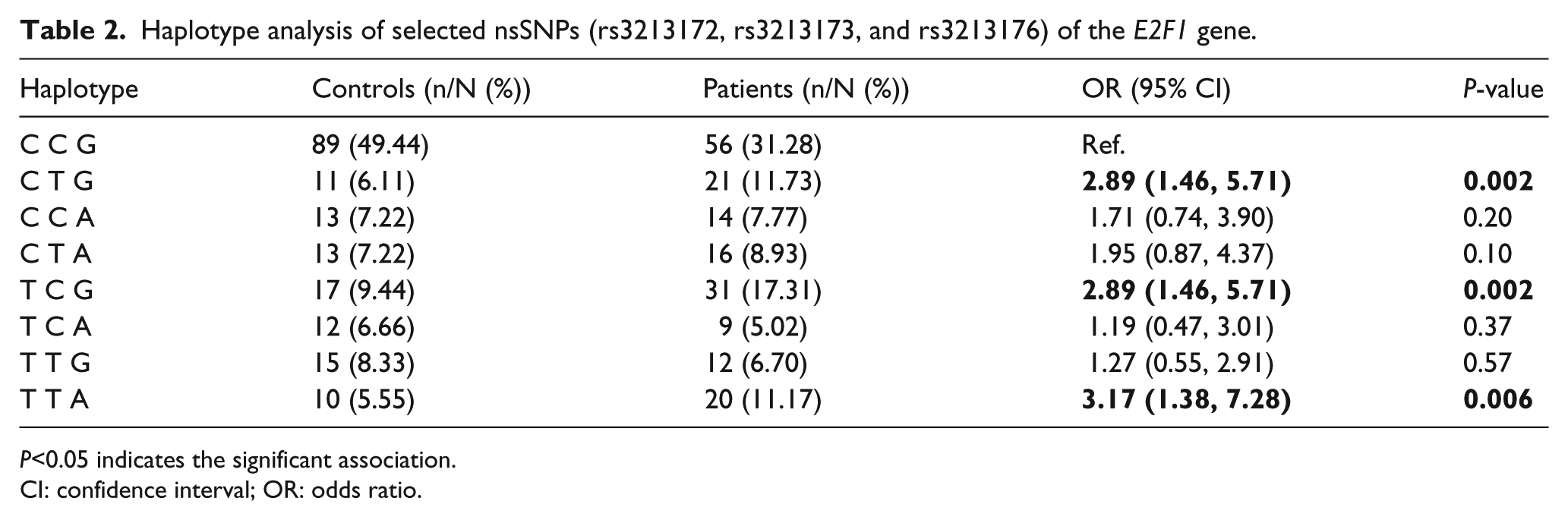
P<0.05 indicates the significant association.
CI: confidence interval; OR: odds ratio.
Discussion
Several mutations in the cell-cycle regulatory genes are associated with cancer as this machinery controls the cellular proliferation. 25 The E2Fs are the transcription factors that regulate the expression of many genes involved in cell growth and differentiation.26-28 During DNA damage responses, ATM/ATR and Chk2 kinases mediated phosphorylation stabilized E2F1, which further activates the DNA repair pathway. 29 If the DNA damage is not rectified by the DNA repair pathway, it leads to apoptosis; other members of this family are not significantly involved in this process. 30 Marked box and an adjacent region of E2F1 are responsible for strongly inducing apoptosis through its interaction with Jab1. 29 As mentioned earlier, E6 and E7 HPV viral proteins are two of the major risk factors for cervical cancer.11,12 The HPV E7 protein binds with E2F1 protein with high affinity and this interaction favors the transformation of infected cells to cancer cells.
The analyzed nsSNPs are present in the high affinity binding region of E2F1. 14 Polymorphisms in this region of E2F1 might change its binding affinity with the HPV E7 protein and alter the susceptibility to cervical cancer in individuals with different genotypes. In this study, we analyzed three polymorphisms of this gene present in a marked box domain (rs3213172 C/T; Arg252His), rs3213173 C/T; Val276Met) and an adjacent region (rs3213176 G/A; Gly393Ser). Moreover, these nsSNPs were also identified as disease risk variants by the NIEHS SNPs program. We found a significant association of rs3213172 (C/T) and rs3213173 (C/T) polymorphisms with cervical cancer risk. The rs3213172 (C/T) was associated with cervical cancer in the heterozygous (OR 1.90; 95% CI 1.01, 3.57; P = 0.04) and dominant (OR 1.96; 95% CI 1.07, 3.60; P = 0.02) models, while rs3213173 (C/T) was associated with cervical cancer risk in the homozygous model (OR 1.90; 95% CI 1.01, 3.57; P = 0.04) (Table 1). The CC and CT genotypes of rs3213172 and rs3213173 were less frequent in the cases than in the controls, whereas the frequency of the TT genotype was higher in the cases compared to the controls (Table 1). We did not find the role of rs3213176 (G/A) in cervical cancer in any of the tested genetic models. Although A allele of this SNP is not significantly associated with the risk of cervical cancer, it is present in higher frequency in cancer patients.
Hwang et al. 14 have demonstrated that HPV E7 interacts with the 191aa -368aa region of E2F1. Two of the SNPs analyzed in this study, rs3213172 (C/T) (Arg252His) and rs3213173 (C/T) (Val276Met), are located in this region and predispose individuals to the risk of cervical cancer. The rs3213176 (G/A) (Gly393Ser) is not present in the HPV E7 interacting domain of E2F1 and is not a risk factor for cervical cancer. This further supports that these SNPs might play a role in cervical cancer susceptibility. The haplotype analysis is more informative than single-association studies. 31 Therefore, we analyzed the haplotypes of E2F1 genetic variants. In this study three haplotypes, TCG, CTG, and TTA of the E2F1 genetic variant were strongly associated with cervical cancer risk (TCG: OR 2.89; 95% CI 1.46, 5.71; P = 0.002; CTG: OR 2.89; 95% CI 1.46, 5.71; P = 0.002; and TTA: OR 3.17; 95% CI 1.38, 7.28; P = 0.006). These findings suggest that TCG, CTG, and TTA haplotypes of the E2F1 gene may serve as a potential biomarker for genetic susceptibility to cervical cancer (Table 2).
This is the first study that reports the association of these polymorphisms with cervical cancer risk. One previous study conducted in the American population revealed the association of combined risk genotypes of promoter region polymorphisms (rs3213182, rs3213183, rs3213180, rs321318121, rs2742976, rs6667575, rs3218203, rs3218148, rs3218211, and rs3218123) of the E2F1 and E2F2 genes with an increased risk of head and neck cancer. 32 Another recent study in the Chinese population revealed that the association of the E2F1 gene polymorphism (rs35301225 (C/A)) with colorectal cancer. 33 Furthermore, promoter polymorphisms (rs3218121, rs3218123, rs3218148, rs2742976, and rs6667575) of this gene have been shown to be associated with the risk of squamous cell carcinoma of the oropharynx (SCCOP; >5.0-fold) in HPV16 positive patients. The risk further increases (OR 21.3) in a high-risk group (patients having four to five combined risk genotypes) while these polymorphisms were not associated with squamous cell carcinoma of the oral cavity (SCCOC) (OR 0.8; 95% CI 0.4, 1.5). 34
Further, the analysis of these polymorphisms with the clinical stage of tumor compared with healthy controls showed an association of rs3213172 and rs3213173 with the late stages of the tumor (III and IV; Supplementary Table 2). These were not associated with the early stages of the tumor (I+II), but there were higher frequencies of the mutant alleles in the earlier stages of cancer. It is possible that these polymorphisms might be playing a role in the cervical cancer progression in our population, which further needs to be tested in a greater number of samples.
Conclusions
We have reported for the first time, an association of rs3213172 (C/T), rs3213173 (C/T), and rs3213176 (G/A) polymorphisms with cervical cancer risk. In addition, we have reported cost-effective artificial-restriction fragment length polymorphism methods to genotype rs3213172 (C/T) and rs3213173 (C/T). This study demonstrated the significant association of rs3213172 (C/T) and rs3213173 (C/T) polymorphisms of the E2F1 gene with the risk of cervical cancer. These nsSNPs are a genetic risk factor for cervical cancer for women from the North Indian population; therefore, it could be used as a biomarker for this cancer, but this should be tested with a greater number of samples and in various replication studies.
Supplemental Material
Supplementary_Tables – Supplemental material for E2F1 genetic variants and risk of cervical cancer in Indian women
Supplemental material, Supplementary_Tables for E2F1 genetic variants and risk of cervical cancer in Indian women by Sanjay Singh, Manish Gupta, Rajeev Kumar Seam and Harish Changotra in The International Journal of Biological Markers
Footnotes
Acknowledgements
H.C. is thankful to the Department of Biotechnology, Government of India, and the Department of Science and Technology, Government of India, for the grants BT/PR6784/GBD /27/466/2012 and SB/FT/LS-440/2012, respectively. The Junior Research Fellowship from the Jaypee University of Information Technology, Solan, Himachal Pradesh, India to S.S. is duly acknowledged.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.