
Abstract
Objective:
This study was performed to investigate whether CSF-1 polymorphisms influenced the risk of renal cell carcinoma in a Chinese population.
Methods:
The potentially functional polymorphisms in CSF-1 (rs333951 and rs2050462) were genotyped in this hospital-based case-control study, comprising 1512 renal cell carcinoma patients and 1691 controls in a Chinese population using the TaqMan assay. Furthermore, odds ratios (ORs) and 95% confidence intervals (CI) were used to estimate such an association. The logistic regression was used to assess the association between these genetic polymorphisms and the risk of renal cell carcinoma.
Results:
We found the genotype and allele frequency distribution of rs2050462 were significantly associated with the increasing risk of renal cell carcinoma (P = 0.007). However, no statistical significance was found in the association between CSF-1 rs333951 polymorphism and the susceptibility of renal cell carcinoma (P = 0.589). The analysis of combined risk alleles revealed that patients with two to four risk alleles showed no elevated risk of renal cell carcinoma compared to those with zero to one risk alleles (adjusted OR 1.09; 95% CI 0.95, 1.26; P = 0.226). Furthermore, compared with the genotypes containing A allele (AC and AA), the patients carrying the CC genotype in rs2050462 had a significantly greater prevalence of clinical stage II and IV (adjusted OR 0.67; 95% CI 0.47, 0.94; P = 0.021; adjusted OR 0.50; 95% CI 0.29, 0.88; P = 0.015, respectively).
Conclusions:
The functional rs2050462 in CSF-1 might have a substantial influence on the renal cell carcinoma susceptibility and evolution in the Chinese population.
Introduction
Renal cell carcinoma (RCC) is the most common occurring type of renal cancer, accounting for about 80% of all primary renal malignancies in adults. 1 Also, RCC is the most lethal of the common urological cancers, with an estimated 388,000 new RCC cases and approximately 144,000 mortalities in the USA in 2017.2,3 The epidemiological studies have demonstrated an increasing incidence of RCC, especially in young patients. 4 In addition, because of a whole range of factors, more than half the patients with RCC present with a local or even systematic metastasis, and are identified at the high-grade or advanced stages, resulting in a poor prognosis.1,3 A series of potential risk factors for RCC, including obesity, smoking, alcohol consumption, kidney stones, acquired cystic kidney disease, and hereditary factors have been described, but the pathogenesis of RCC is still needed for further research to investigate such associations.1,5-8 Although many people were exposed to these risk factors, only a small percentage of the exposed individuals eventually developed RCC in their lifetime, indicating that genetic susceptibility might play an important role in the development of RCC.9,10 Herein, it is of great clinical significance to identify more molecular markers to detect and diagnose RCC. Meanwhile, genetic polymorphisms of this candidate gene might influence the risk of RCC among the Chinese population.
Macrophage colony-stimulating factor (CSF-1) is an essential dimeric polypeptide growth factor for cells of the macrophage lineage that regulates the mononuclear phagocyte system and bone metabolism.11,12 The effect of CSF-1 is mediated via the cell surface receptor (CSF-1R) encoded by the c-fms proto-oncogene. In addition, it is expressed on mononuclear phagocytes, osteoclasts, and some cancer cells.13-16 Depending on the context and the exact cell type studied, the actions of CSF-1 at its receptor CSF-1R were originally identified as a regulator of the proliferation and differentiation of mononuclear phagocyte progenitors and the survival as well as the effector functions of macrophages and the bone marrow progenitor cells.11,17 Previous studies have primarily focused on the expression of CSF-1 or CSF-1R in breast cancer.18,19 Here, we showed that an expanded list of CSF-1 responsive genes was possibly used to identify RCC that might be uniquely sensitive to macrophage-targeted therapies. 20
In consideration of the critical role of CSF-1 genetic variants in RCC, we sought to systemically investigate the associations between single nucleotide polymorphisms (SNPs) in the CSF-1 gene and the predisposition to RCC development. However, the available studies remained conflicting. To validate this hypothesis, we genotyped these polymorphisms and determined its association with the susceptibility to RCC in a hospital-based case-control study, including 1512 cases and 1691 controls in a Chinese population. Accordingly, these two SNPs in CSF-1 (rs333951 and rs2050462) were selected and their genetic associations with RCC risk were evaluated using logistic regression analysis to identify if genetic variants in CSF-1 might be a potentially genetic marker to predict the susceptibility of RCC.
Materials and methods
Study population
In the present ongoing case-control study, a total of 1512 incident patients with histopathologically confirmed RCC and a group of 1691 age-matched controls were consecutively recruited from May 2004 to March 2017 at the Department of Urology, the First Affiliated Hospital of Nanjing Medical University, and the Department of Urology, the Affiliated Cancer Hospital of Jiangsu Province of Nanjing Medical University, Nanjing, China. In brief, all these subjects were genetically unrelated ethnic southern Han Chinese. Nevertheless, patients with a blood relationship or from the same region or the same families were excluded from this study in advance. In addition, none of the patients had a prior history of other cancers, or previous chemotherapy or radiotherapy, or metastasized cancer for other or unknown reason before. In the interim, the controls were randomly selected from healthy volunteers who were seeking physical examination in the outpatient departments at the hospital matched on age (mean 65 years) to the cases on frequency.
Those subjects who smoked daily for more than one year were defined as ever smokers; and the others were considered as non-smokers. Individuals who drank alcohol at least three times per week for a period lasting more than six months were defined as ever drinkers; otherwise, the rest were considered as non-drinkers. A family history of cancer was defined as any cancer in first-degree relatives (parents, siblings, or children). The disease was classified on the basis of the World Health Organization criteria and stage according to tumor-node-metastasis (TNM) classification system promulgated by the American Joint Committee on Cancer (AJCC). The Fuhrman scale was used to assess tumor nuclear grade, and the disease stage was divided into localized group (stage I and stage II) and advanced group (stage III and stage IV). The research protocol was approved by the Institutional Review Board of the Nanjing Medical University, Nanjing, China, and the study was carried out in accordance with the nationally approved guidelines.
Before enrollment, all participants involved in this study were required to write a standard questionnaire by well-trained interviewers to collect demographic data, clinical data, and exposure-related information through face-to-face interviews, including age, race, tobacco use, alcohol intake, and self-reported family history of cancer. After signing a written informed consent, all subjects donated about 5 mL venous blood samples for genomic DNA extraction. The participation response rates for both case and control subjects exceeded 85%.
SNP Selection
Based on HapMap data (http://hapmap.ncbi.nlm.nih.gov/) and PubMed data (http://www.ncbi.nlm.nih.gov/projects/SNP/), some potentially functional tSNPs in the CSF-1 gene were chosen. Minor allele frequency (MAF) of each gene polymorphism was more than 5% in the Han Chinese population. When some of the SNPs were in complete linkage disequilibrium (r2 = 1), only one SNP was selected for genotyping. Finally, we included two SNPs in CSF-1 (rs2050462 and rs333951), which might be found to be significantly associated with some malignancies in the Chinese population.
DNA extraction and polymorphism genotyping
Total genomic DNA was extracted and purified from the anti-coagulated peripheral blood lymphocytes by proteinase K digestion and phenol-chloroform extraction. Before genotyping, we conducted DNA quality control and made sure that all DNA samples were qualified. The genotyping of CSF-1 polymorphisms (rs333951 and rs2050462) was performed by pre-designed TaqMan SNP Genotyping Assays (Applied Biosystems, Foster City, CA, USA). The tSNPs information, sequences of primers and probes of each SNP were available as requested. The polymerase chain reaction (PCR) conditions were two min at 50℃, 10 min at 95℃, followed by 45 cycles of 95℃ for 15 sec and one min at 60℃. Amplifications and analysis were adopted by the genotyping assay in the 384-well ABI 7900HT Real-Time PCR System (Applied Biosystems), according to the manufacturer’s instructions. Also, Sequence Detection Systems software (SDS 2.4; Applied Biosystems) was used to automatically collect and analyze the data for subsequently allelic discrimination. Positive controls by sequencing and negative controls without DNA were used in each plate, in order to ensure the accuracy of genotyping. Furthermore, four negative controls were included in each 384-well plate for quality control. Finally, two investigators performed genotyping independently in a blinded manner, and approximately 10% of the DNA samples from the cases and controls were randomly chosen for repeated genotyping for confirmation with a reproducibility of 100%.
Statistical analysis
Before analysis, deviation of genotype distribution from the Hardy–Weinberg equilibrium (HWE) for the CSF-1 polymorphisms in the controls was tested using a goodness-of-fit chi-square test. Differences in the distributions of demographic characteristics, selected variables, and frequency distributions of genotypes polymorphisms alleles and genotypes between cases and controls were analyzed using the chi-square test (for categorical variables) or the Student’s t-test (for continuous variables). The associations between CSF-1 polymorphisms and risk of RCC were estimated by computing the crude and adjusted odds ratios (ORs) and their 95% confidence intervals (CIs) from unconditional univariate and multivariate logistic regression analysis with the adjustment for possible confounders. All data were analyzed with the software SPSS (version 22.0; SPSS Inc., Chicago, IL, USA) with a two-sided test, and the adjusted P value of less than 0.05 was deemed as statistically significant.
Results
Characteristics and clinical features of the study population
The frequency distributions of the selected characteristics of 1512 patients and 1691 controls are listed in Table 1. Overall, the cases and controls appeared to be adequately matched in terms of age (P = 0.075), body mass index (P = 0.362), sex (P = 0.687), smoking status (P = 0.515), drinking status (P = 0.908), and family history of cancer (P = 0.826). The mean age of RCC patients was 56.88 years and that of controls was 56.43 years. However, a significantly higher proportion of the cases was of hypertension patients (39.48%) and diabetics (12.83%) in comparison with the controls (60.52% and 87.17%, respectively), and these differences were statistically significant (P <0.001 for hypertension and diabetes). Among the RCC cases, 1003 (66.34%) patients were diagnosed with stage I disease, 290 (19.18%) with stage II, 111 (7.34%) with stage III, and 108 (7.14%) with stage IV. In addition, the percentage of nuclear grade from I to IV was 19.71%, 51.98%, 21.56%, and 6.75%, respectively. These variables were further adjusted in the multivariate logistic regression analysis to assess the main effect of the CSF1 polymorphisms on RCC risk.
Distribution of selected variables between the renal cell cancer cases and the control subjects.
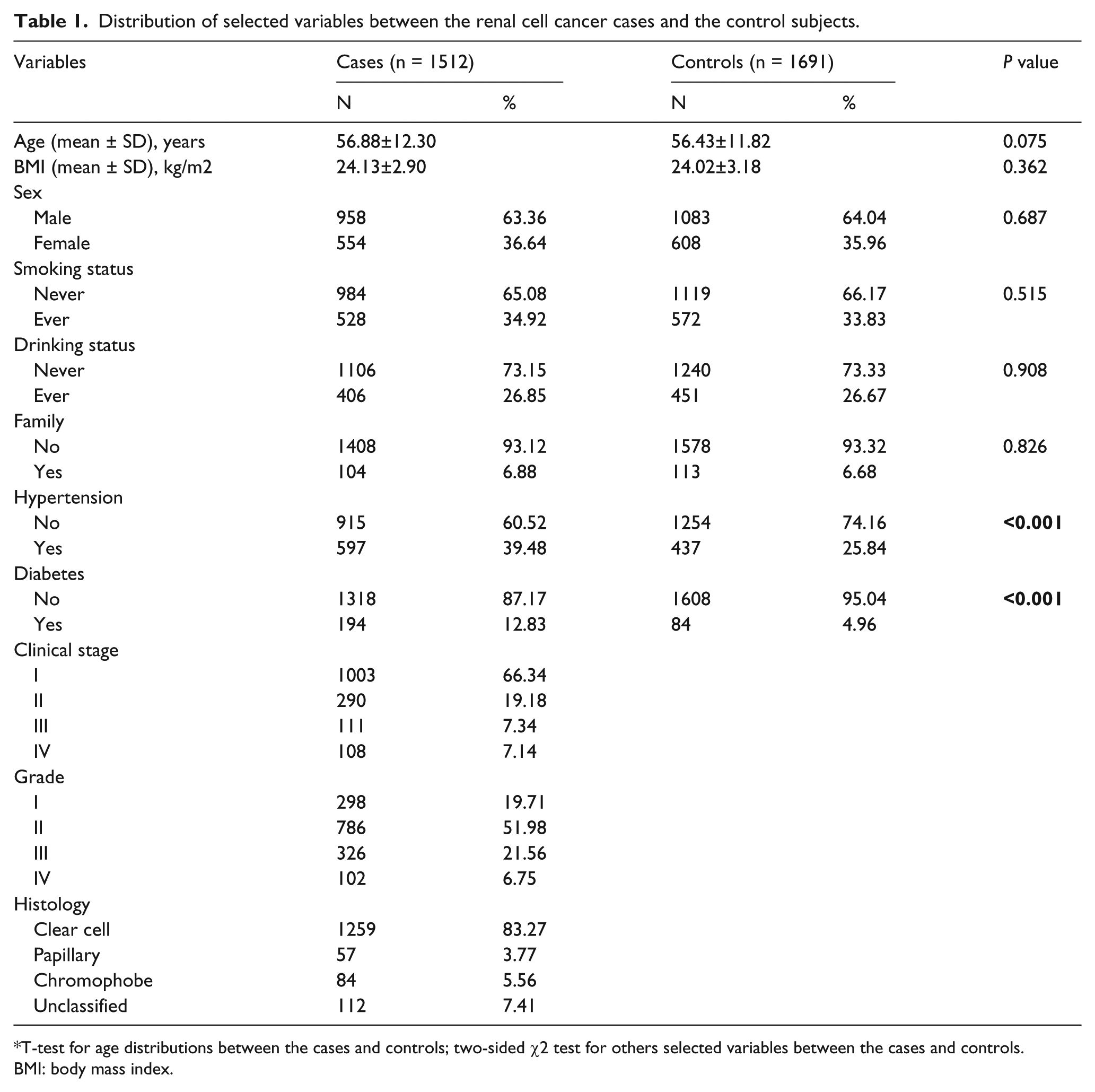
T-test for age distributions between the cases and controls; two-sided χ2 test for others selected variables between the cases and controls.
BMI: body mass index.
Genotype and allele frequencies of CSF-1 polymorphisms in cases and controls
The genotype and allele distributions of CSF-1 SNP rs333951 and rs2050462 between RCC cases and controls are summarized in Table 2. The observed genotype frequencies of these two CSF-1 polymorphisms among the controls confirmed to the HWE (all P > 0.05). In the CSF-1 gene, the genotype of rs2050462 polymorphism distribution between cases and controls was significantly different (P = 0.007). Compared with individuals carrying the rs2050462 CC genotype, subjects with AC, AA, and AC+AA genotypes were both associated with a significant elevated risk of RCC (P = 0.001, adjusted OR 1.20; 95% CI 1.07, 1.34; P = 0.001; adjusted OR 1.44; 95% CI 1.15, 1.79 and P = 0.010; adjusted OR 1.21; 95% CI 1.05, 1.40, respectively). Nevertheless, logistic regression analysis also showed no association between rs333951 polymorphism and the risk of RCC (P = 0.589).
The basic information of the genotyped polymorphisms in four SNPs in the CSF-1 associated with the RCC risk.
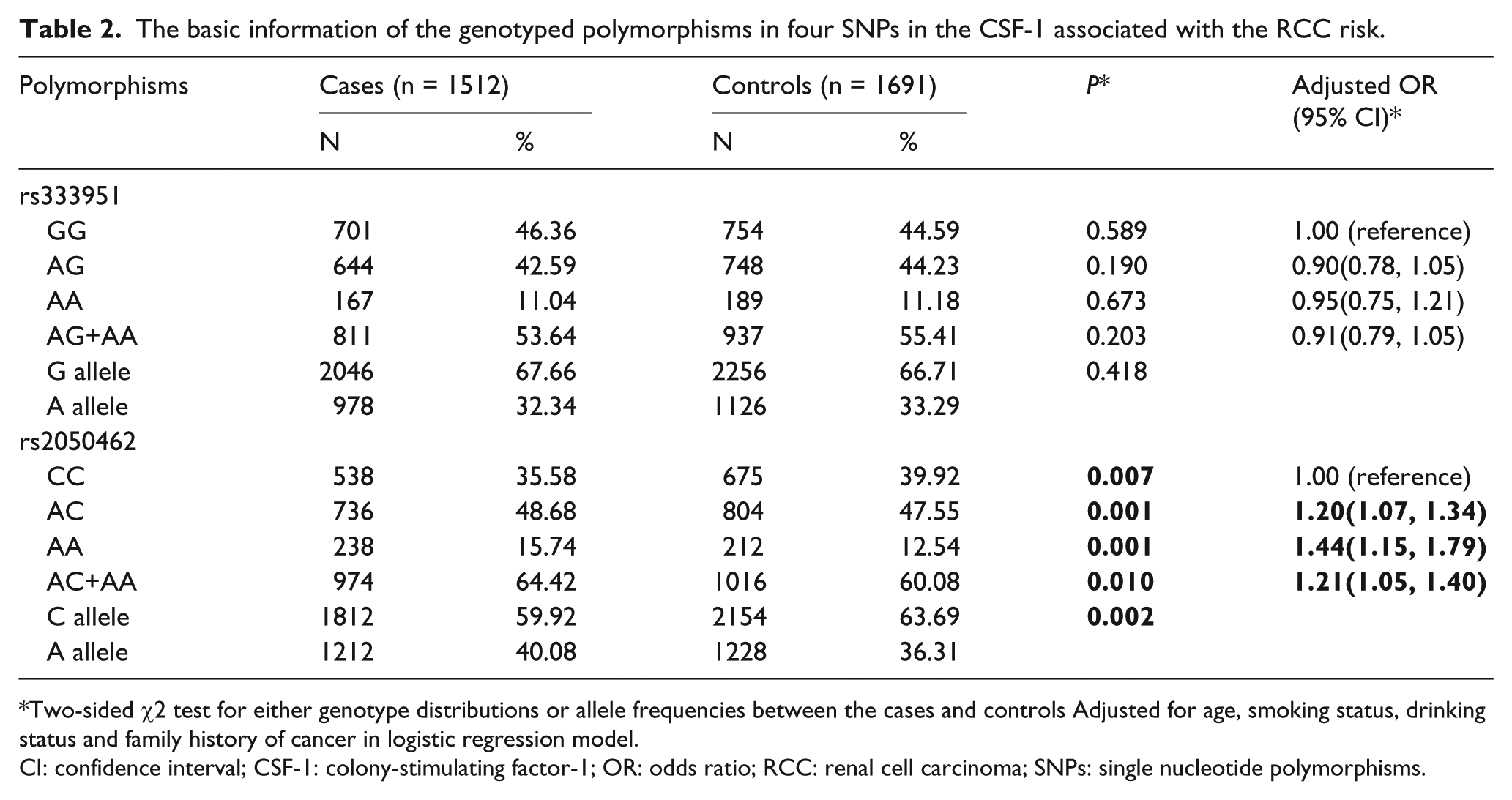
Two-sided χ2 test for either genotype distributions or allele frequencies between the cases and controls Adjusted for age, smoking status, drinking status and family history of cancer in logistic regression model.
CI: confidence interval; CSF-1: colony-stimulating factor-1; OR: odds ratio; RCC: renal cell carcinoma; SNPs: single nucleotide polymorphisms.
The analysis of combined polymorphisms and RCC risk
These two polymorphisms (rs333951 and rs2050462) were combined based on the number of the risk alleles to explore the genetic power on the risk of RCC. As shown in Table 3, with the increasing of the number of the risk alleles, elevation of the RCC risk was not observed and the difference was not statistically significant. Also, when we divided the patients into two groups, the patients with two to four risk alleles did not show a more remarkable growth of RCC risk than the patients with zero to one risk alleles (P = 0.226; adjusted OR 1.09; 95% CI 0.95, 1.26) comparing with other group combinations.
Analysis between combined risk alleles and RCC susceptibility.
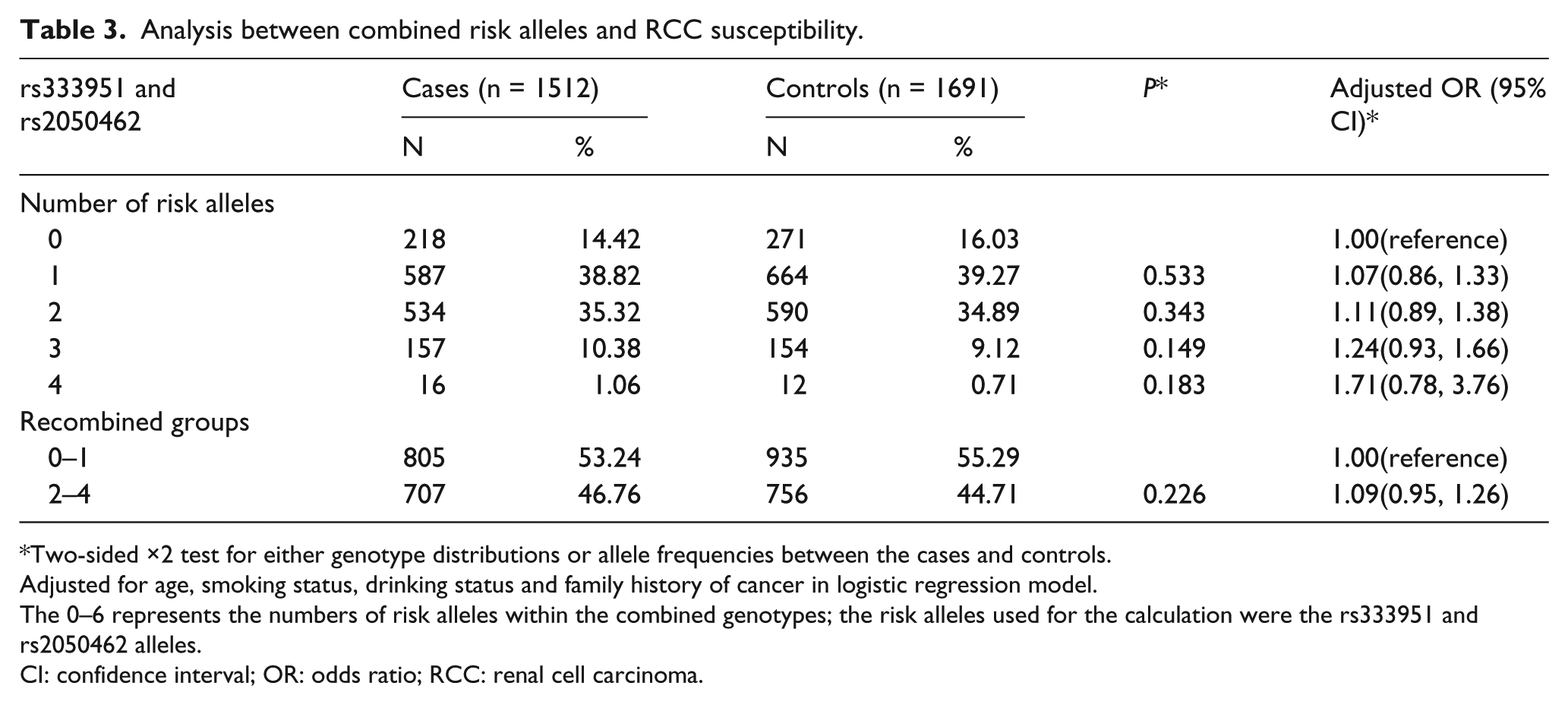
Two-sided ×2 test for either genotype distributions or allele frequencies between the cases and controls.
Adjusted for age, smoking status, drinking status and family history of cancer in logistic regression model.
The 0–6 represents the numbers of risk alleles within the combined genotypes; the risk alleles used for the calculation were the rs333951 and rs2050462 alleles.
CI: confidence interval; OR: odds ratio; RCC: renal cell carcinoma.
However, as listed in Table 4, the frequencies of patients with two to four risk alleles had a significant difference in both stage II of RCC (P = 0.031; adjusted OR 0.69; 95% CI 0.49, 0.97), and stage III (P = 0.016; adjusted OR 0.51; 95% CI 0.30, 0.88). Moreover, no significant difference appeared in the association between the two to four risk alleles and RCC patients with well-differentiated RCC (P = 0.600).
Association between the combined genotypes of rs333951 and rs2050462 polymorphisms and clinicopathological characteristics of clear cell renal cell carcinoma.
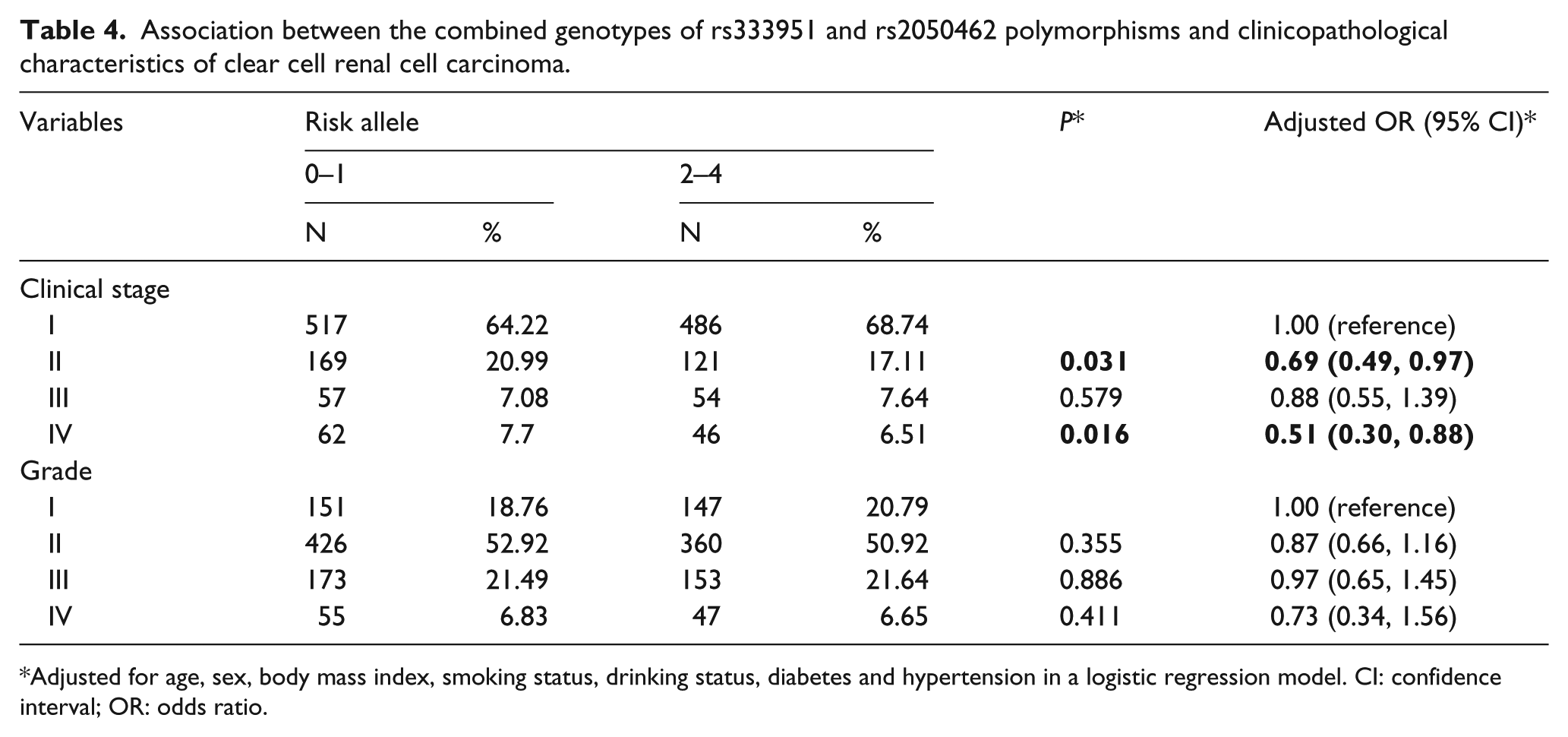
Adjusted for age, sex, body mass index, smoking status, drinking status, diabetes and hypertension in a logistic regression model. CI: confidence interval; OR: odds ratio.
We then investigated the association of the CSF1 rs2050462 polymorphism and clinicopathological characteristics of RCC patients. As shown in Table 5, no significant difference was observed in patients with moderately (grade I and II) or poorly differentiated (grade III and IV) nuclear grade. Interestingly, the rs2050462 CC were significantly more frequent in patients with clinical stage II and IV (P = 0.021; adjusted OR 0.67; 95% CI 0.47, 0.94; P = 0.015; adjusted OR 0.50; 95% CI 0.29, 0.88, respectively) compared with individuals carrying AC+AA.
The association of CSF-1 rs2050462 polymorphism and clinicopathological characteristics of RCC patients.
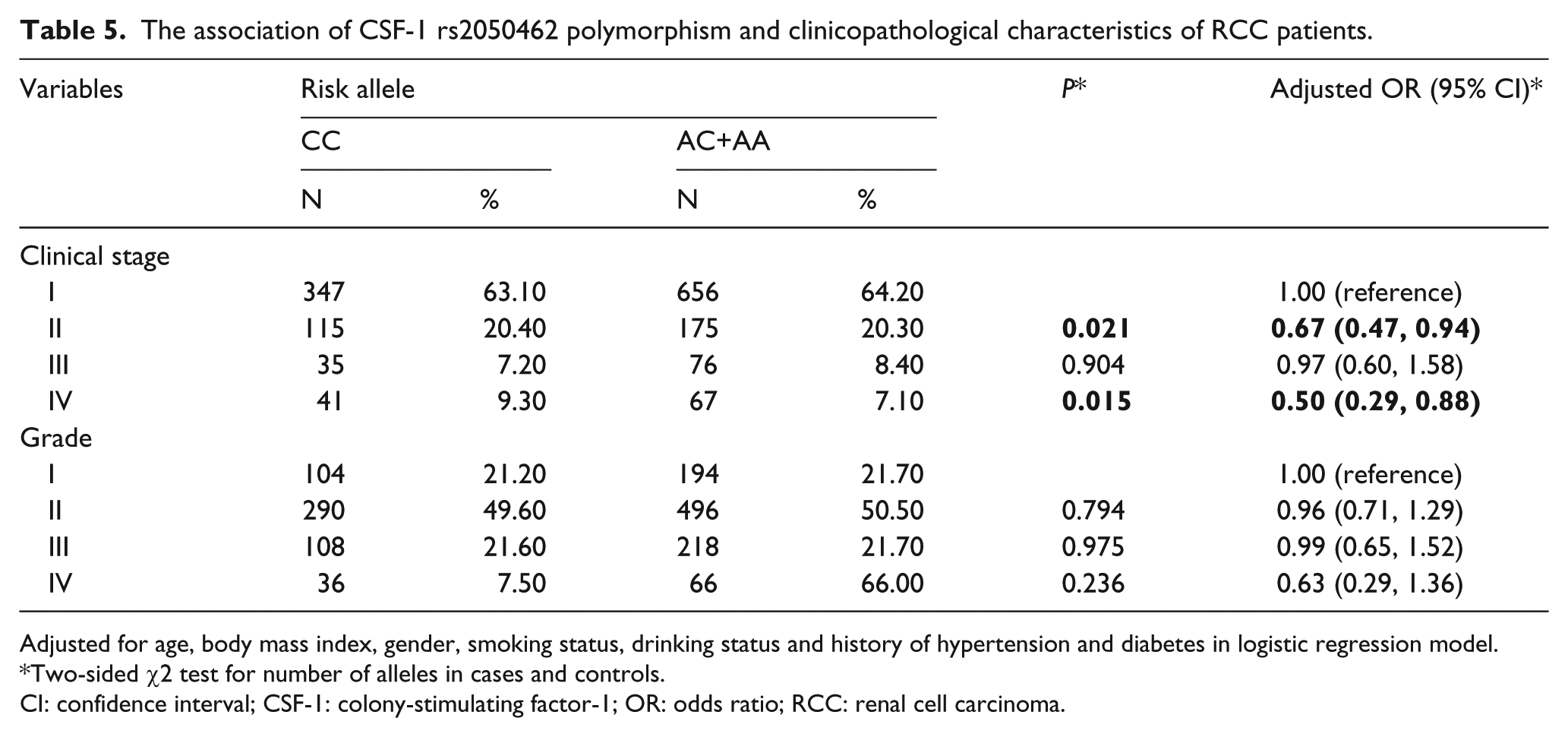
Adjusted for age, body mass index, gender, smoking status, drinking status and history of hypertension and diabetes in logistic regression model.
Two-sided χ2 test for number of alleles in cases and controls.
CI: confidence interval; CSF-1: colony-stimulating factor-1; OR: odds ratio; RCC: renal cell carcinoma.
Discussion
In this hospital-based case-control study, the function of CSF-1 polymorphisms is studied to clarify the risk and manifestation of clinicopathological characteristics of RCC. We found that a significantly increased susceptibility of RCC was associated with CSF-1 rs2050462 genotypes, compared with the rs2050462 CC genotypes. Nevertheless, we could not find any significant difference in the CSF-1 rs333951 genotype frequency between the RCC patients and controls. Moreover, we evaluated rs333951 and rs2050462 together and found that there was no statistical significance associated with the two CSF-1 polymorphisms and the risk of RCC. To the best of our knowledge, this is the first study to investigate the relationship between CSF-1 polymorphisms and the risk and occurrence of RCC in a Chinese population.
As a dimeric polypeptide growth factor, CSF-1 is secreted by macrophages, epithelial, fibroblasts cells, and cancer cells.12,21 In addition, CSF-1—located on the long arm of chromosome 5—is mediated by a tyrosine kinase receptor (CSF-1R) encoded by the c-fms proto-oncogene that spans 20 kb and contains 10 exons.22,23 CSF-1 is a primary regulator that influences hematopoietic stem cells to differentiate into macrophages or other related cell types, and plays an important role in regulating mononuclear phagocyte maturation and skeletal metabolism.11,12,17,24,25 Moreover, CSF-1 plays vital roles in normal development, and functions as mediators of intercellular communication by diffusible molecules. 26 Nevertheless, in addition to its normal role in mononuclear phagocyte biology, the elevated circulating CSF-1 is found extracellularly as a disulfide-linked homodimer, and has been reported to be correlated with tumor progression, high grade, and poor prognosis in many cancers. 27 CSF-1 can stimulate cancer cells directly, and can promote tumorigenesis indirectly through mobilizing and adjusting the host immune system responding to cancer cells. 28 In addition, previous studies have demonstrated that a strong correlation of CSF-1 expression with dense leukocytic infiltration, which contains a large percentage of CSF-1R-bearing cells, has been found in the increased inflammation and poorer prognosis in patients with breast cancer.29,30 The coexpression of CSF-1 and CSF-1R in these cells suggest that CSF-1 might be involved in tumor invasion through its direct influence on CSF-1R-bearing tumor cells. 31
With a growing interest in the association between the CSF-1 polymorphisms and RCC risk, we determined whether or not CSF-1 polymorphisms were associated with the risk of RCC. In our study, we genotyped the polymorphisms in CSF-1 to explore the association between CSF-1 genetic variants and RCC susceptibility in a Chinese population. The CSF-1 rs2050462 significantly differed between RCC patients and control participants, indicating that the risk of RCC was increased in participants with the AA, AC, or AA+AC genotypes of rs1944129, compared to CC genotypes. However, CSF-1 rs333951 had not increased the risk and occurrence of RCC, which was possibly because CSF-1 rs333951 was not an SNP in the promoter region, which might affect the expression of CSF-1. The further analysis of the combining risk alleles in CSF-1 polymorphisms rs333951 and rs2050462 showed that the group of patients with two to four risk alleles was no more susceptible to RCC compared with those with zero to one risk alleles. In addition, the frequencies of patients with two to four risk alleles had a significant difference in stage II and III of RCC. There was no correlation between the combined genotypes and the clinical grade. No significant association between the polymorphisms and the tumor nuclear grade of RCC was observed; we surmise that the effect of rs2050462 on the expression of CSF-1 is not powerful enough to influence the tumor nuclear grade of RCC. However, compared with individuals carrying AC+AA, the rs2050462 CC was significantly more frequent in patients with clinical stage II and IV.
As mentioned above, CSF-1 in the cancer cells could increase the migration ability of macrophages through the autocrine loop, thus promoting the tumor invasion and metastasis, and further stimulating the secretion of CSF-1. 32 Consequently, we proposed that the release of CSF-1 might not only act in an autocrine manner to enhance proliferation and invasion of the tumor, and to modify the host immune function in a paracrine manner, but also act as a bone-stored factor. The release of CSF-1 from resorbed bone might further recruit macrophages to the tumor site where they promoted tumor expansion. 33 The overexpression of CSF-1 could accelerate tumor progression and metastasis, and was associated with the aggressive behavior of malignancies, including breast, uterine, and ovarian cancer.34,35 A marked leukocytic infiltration in these tumors also correlated with poor prognosis with the majority of these cells being macrophages.29,36
When interpreting our results, several potential limitations should not be ignored in the present study. First, as our study was a hospital-based study, the possibility of inherent selection bias and recall bias of subjects could not be entirely excluded. Nevertheless, the genotype distributions of CSF-1 polymorphisms in our controls were similar to that in the HapMap database of the Chinese population, suggesting that the selection bias of subjects associated with a particular genotype was unlikely to be substantial. Second, we have no detailed information on cancer risk factors, such as diet, physical activity, and occupational exposure, to further evaluate the relationship between environmental factors and the risk of RCC. Accordingly, considering the low frequency of variant alleles, the sample size might be not large enough, so that bias existed in analyzing the multiple comparisons in the present study.
Conclusion
In conclusion, the present study provides evidence to elucidate the association between CSF-1 polymorphisms and the susceptibility and pathogenesis of RCC. We found CSF-1 rs2050462 has a significant influence on the occurrence and progression of RCC in the Chinese population, but a lack of association between CSF-1 rs333951 polymorphism and the risk of RCC was found in our population. Meanwhile, the combination of risk alleles in CSF-1 rs2050462 and rs333951 indicated no significant difference in the risk of RCC. More importantly, additional studies with larger sample sizes and more environmental and survival factors are warranted to further validate the association of the polymorphisms with the elevated risk of RCC to confirm our findings.
Footnotes
Author contributions
Xiao Li, Zhiqiang Qin and Jianxin Xue contributed equally to this work.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.