
Abstract
The safety of vancomycin in children requires special attention. The evidence from active pharmacovigilance systems about vancomycin-related adverse drug reactions (ADRs) was rare. We aimed to investigate the association between doses of vancomycin and ADRs among children. This retrospective cohort study included a total of 643 inpatient children. Children who received vancomycin were regarded as exposed groups and classified into low-dose, normal-dose, and high-dose groups. Those who did not receive vancomycin and had similar severity of infection were classified into the unexposed group. ADR signal detection was performed by the China Hospital Pharmacovigilance System. Logistic regression analyses were conducted to explore the effect of intravenous vancomycin on ADRs. This study included 156 patients (178 ADR cases) in the exposed group and 487 patients (364 ADR cases) in the unexposed group. The top three reported ADRs were eosinophilia (n = 75, 48.1%), hemoglobin decreased (n = 72, 46.2%), and blood bilirubin increased (n = 13, 8.3%) in the exposed group. Patients in the low-dose, normal-dose, and high-dose groups showed a higher risk of hemoglobin decreased when compared with those in the unexposed group, with the fully adjusted ORs (95% CIs) of 6.91 (3.61, 13.20), 7.80 (3.87, 15.76), and 8.80 (4.08, 19.01), respectively. Besides, compared with patients in the unexposed group, those in the normal-dose and high-dose groups show a significantly higher risk of eosinophilia and blood bilirubin increased, respectively. It is important to monitor eosinophilia, hemoglobin decreased, and blood bilirubin increased in pediatrics receiving vancomycin, especially those receiving normal-dose and high-dose vancomycin.
Keywords
Introduction
Children, especially newborns, are susceptible to bacterial infections due to the immature immune system. 1 Staphylococcus is one of the main pathogenic bacteria of common infectious diseases such as septicemia, pneumonia, and bacterial meningitis in children. 2 Vancomycin, a glycopeptide antibiotic that inhibits bacterial cell wall synthesis, is a drug of last resort for the treatment of severe infections caused by Gram‐positive bacteria 3 especially methicillin-resistant Staphylococcus aureus (MRSA). 4 A previous study showed that the effective rate of vancomycin treatment in pediatric patients with severe infections in the pediatric intensive care unit was 69.1%. 5 Unlike adults with a decreasing trend of MRSA isolation rate, children have seen an increasing trend in their isolation rate in recent years in China. 6
Due to the incomplete development of organs and slow drug metabolism in children, adverse drug reactions (ADRs) are more likely to occur in children. 7 The safety of vancomycin in children requires special attention. Several studies have reported ADRs associated with vancomycin use in children. LIMA et al. 8 summarized the ADR reports from the Adverse Drug Reaction monitoring between 2008 and 2013 and found that most vancomycin ADRs occurred in children aged 0-12 years old. LIN et al. 9 found that, from 2009 to 2011, the incidence of red man syndrome in children receiving vancomycin aged 0-17 years in a hospital was 5.80%. Additionally, ototoxicity 10 and nephrotoxicity 11 associated with vancomycin use in this pediatric population had also been found. However, data from the study above were collected by spontaneous reporting systems (SRS) or population-based cohorts, which were unable to obtain the incidence of ADRs and might result in a high underreporting rate. The evidence from active pharmacovigilance systems about vancomycin-related ADRs was rare.
The dose was commonly identified as a risk factor for the occurrence of certain ADRs. Previous data suggested several risk factors of VIN, including higher daily dose. 12 A study by Dong 13 suggested that nephrotoxicity is independently associated with a vancomycin dosage >38 mg/kg/day and a serum trough level >20 mg/L in adults. Besides, the incidence of vancomycin-associated nephrotoxicity decreased after the implementation of therapeutic drug monitoring using the area under the concentration-time curve (AUC)-guided dosing strategy in adults, 14 which might be better than trough-guided strategies. 15 The trough concentrations in most children are low and do not reach the adult standard after the administration of standard doses of vancomycin. 16 Clarifying the effect of vancomycin dosage in children could lay the foundation for developing those strategies in children in the future. Nevertheless, some other ADRs may not be completely related to dose. Currently, few studies report the relationship between dosage and other vancomycin-induced ADRs. 17
As a specialized hospital, our institution recorded an average usage of approximately 800 bottles of vancomycin with different doses per year between 2018 and 2021. Considering the large amount of vancomycin used in pediatric patients, we aimed to evaluate the effect of different doses of vancomycin on ADRs and to provide evidence for the clinical application of vancomycin.
Methods
The China hospital pharmacovigilance system
The China hospital pharmacovigilance system (CHPS) is an information system established by the National ADR Monitoring Center to assist in the detection, reporting, and evaluation of adverse drug reactions/events, conduct key monitoring, post-marketing research, and obtain pharmacovigilance information for drugs and medical devices. 18 Compared to other SRSs, the advantage of CHPS lies in its integration with hospital-related information systems, including hospital information system, laboratory information system, electronic medical record (EMR), etc. Besides, CHPS is an active pharmacovigilance system. Researchers can discover ADRs through an intelligent search model based on Boolean logic rules, addressing issues such as high underreporting rates, poor timeliness and report quality in SRS. This allows for the scientific and comprehensive collection of ADRs associated with drugs of interest. In the current study, ADRs were obtained through CHPS to avoid omissions caused by subjective awareness and to ensure the integrity of ADR data.
Study population and data collection
The workflow of the study was shown in Figure 1. This retrospective cohort study included children under 18 who were admitted to the study hospital and received intravenous vancomycin between January 1st, 2018 and December 31st, 2021. An unexposed group of patients that did not receive vancomycin but had similar diagnoses containing “infection” or “sepsis” and similar severity of infection (based on the values of procalcitonin >2 μg/L, C-reactive protein >100 mg/L, and interleukin-6 > 1000 μg/L) during the same period was identified for comparative analysis according to expert consensus on the clinical significance of infection-related biomarkers in China.
19
Preterm newborns were excluded from our study due to significant differences in blood examinations, such as hemoglobin and bilirubin levels. Demographic and clinical data of patients, including gender, age, body weight, and concomitant medications, were collected. The collection of human data in our study was carried out in accordance with the Declaration of Helsinki. The study was approved by the Ethics Council of Human Research in the Xiamen Maternity and Child Health Care Hospital (No. KY-2023-051-K01), and informed consent was waived owing to the retrospective nature of the study. The workflow of the study. ADRs: adverse drug reactions; CHPS: china hospital pharmacovigilance System; CTCAE: common terminology criteria for adverse events; FDA: food and drug administration; MedDRA: Medical dictionary for regulatory activities; PTs: preferred terms; SmPC: summary of product characteristics.
Dose groups
The patients who received vancomycin were regarded as exposed groups and divided into three subgroups: low-dose, normal-dose, and high-dose groups. The normal dosage regimens were listed as follows: 10-15 mg/kg q12 h for newborns aged 0-7 days, 10-15 mg/kg q8h for newborns aged 8-28 days, and 40-60 mg/kg/d for children aged 29 days to 18°years.20–22 The low-dose group was defined as those who received a dose below the lower limit of the normal range listed above, while the high-dose group was defined as those who received a dose higher than the upper normal limit.
Algorithm development and ADR signal detection
ADR information for algorithm development to detect signals was obtained from the FDA-approval label or Summary of Product Characteristics (SmPC) of vancomycin (VIANEX S.A.). 20 ADRs associated with vancomycin were defined and evaluated according to Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0. Based on the definition of each type of ADR, we edited the corresponding retrieval models on the CHPS system. CHPS provided 10 categories of dimensions (patient information, laboratory data, medical orders, medical records, diagnosis, signs, examination, transfer, surgery, and function retrieval) and 55 sub-dimensions for researchers to customize multi-dimensional retrieval models, which were combined by Boolean logic rules (and, or, not). The retrieval model could help researchers find patients who meet the retrieval criteria in the medical records and display their specific socio-demographic and clinical information. The ADR signal detection results were subsequently reviewed by two trained clinical pharmacists. ADRs were described and characterized using preferred terms from the Medical Dictionary for Regulatory Activities.
Statistical analysis
Non-normally distributed continuous variables (age and weight) were presented as medians (P25, P75) and analyzed with the Kruskal-Wallis H test. Categorical variables were described as frequencies (%) and analyzed with the Pearson chi-square test, continuity correction test, or Fisher’s exact test. A univariate binary logistic regression was performed to screen confounders, including patient demographic factors such as gender (male/female), weight (continuous), and age (continuous), as well as the use of concomitant medications (yes/no) such as levocarnitine, furosemide, meropenem, phenobarbital, and piperacillin-tazobactam among all patients, including the exposed group and the unexposed group. These confounding factors were included in the model separately when conducting univariate binary logistic regression. Moreover, the multivariable logistic regression models were used to estimate odds ratios (ORs) and 95% confidence intervals (CIs) of the dose of vancomycin in relation to the top 3 ADRs among pediatric patients. Variables with p-values less than 0.05 on univariate analysis were subjected to multivariate binary logistic regression analyses. Concomitant use of levocarnitine, furosemide, meropenem, phenobarbital, and piperacillin-tazobactam were adjusted for analyzing the association between the dose of vancomycin and hemoglobin decreased. Age, weight, and concomitant use of phenobarbital were adjusted to analyze the association between dose of vancomycin and eosinophilia. Concomitant use of furosemide, meropenem, and phenobarbital were adjusted for analyzing the association between the dose of vancomycin and blood bilirubin increased. Tests of the trend for ORs across dose categories were performed by including 0 (unexposed group), 1 (low-dose group), 2 (normal-dose group), and 3 (high-dose group) values as a continuous variable in the logistic regression models. All statistical analyses were conducted using IBM SPSS (version 21.0.0.0). A p-value less than 0.05 was considered statistically significant.
Results
Demographic characteristics of the study population
Demographic characteristics of including study population.
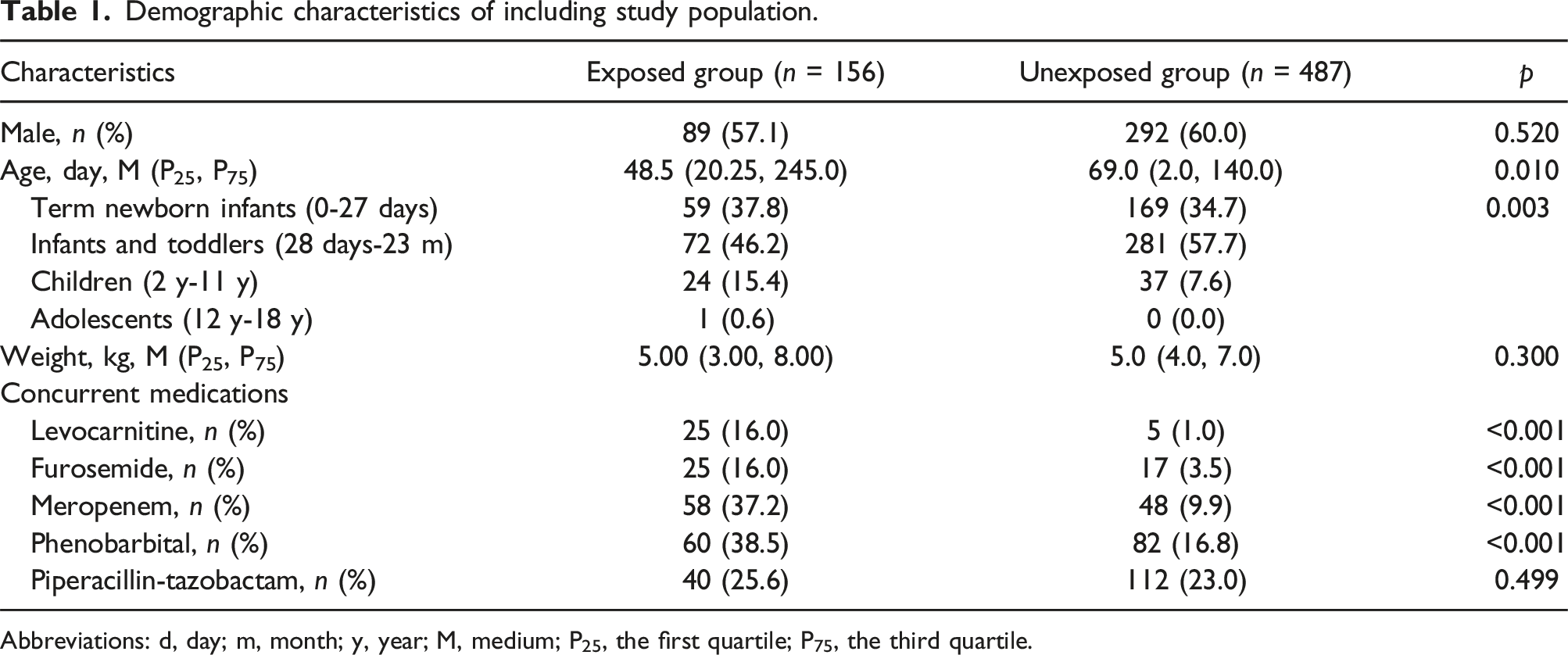
Abbreviations: d, day; m, month; y, year; M, medium; P25, the first quartile; P75, the third quartile.
Incidence of ADRs in pediatric patients
Incidence of ADRs in the exposed group and the unexposed group.

Abbreviations : PT, Preferred Terms (MedDRA).
aDifference between groups were analyzed with continuity correction test.
bDifference between groups were analyzed with Fsiher’s exact test.
Vancomycin and the top 3 ADRs in pediatric patients
Due to the limited sample size, we only further explored the relationship between intravenous vancomycin and the top 3 ADRs in the exposed group (eosinophilia, hemoglobin decreased, and blood bilirubin increased). The univariate regression analyses revealed that compared to the unexposed group, normal-dose were associated with a higher risk of eosinophilia. The low-, normal-, and high-dose groups showed an increasing risk in the incidence of hemoglobin decreased (P-trend<0.001). Normal-dose and high-dose were associated with a higher risk of blood bilirubin increased (P-trend<0.001) (Supplementary Table 3). Besides, weight, age, and the concomitant use of phenobarbital were associated with eosinophilia. The concomitant use of levocarnitine, furosemide, meropenem, phenobarbital, and piperacillin-tazobactam was associated with a higher risk of decreased hemoglobin. In addition, the concomitant use of furosemide, meropenem, and phenobarbital were associated with a higher risk of increased blood bilirubin (Supplementary Table 4). These factors were further included in the multivariate logistic regression analyses.
Multivariate logistic regression analysis for the top 3 ADRs.

a“NA”: the relevant risk factor with p > .05 on univariate analysis were not included in the multivariate logistic regression.
Discussion
In this study, we investigated the possible ADRs caused by vancomycin and their relationship in inpatient children. A total of 104 patients in the exposed group (156 patients) had ADRs with an incidence of 66.67%, of which the most common ADRs were eosinophilia, followed by hemoglobin decreased and blood bilirubin increased. Normal-dose of vancomycin was associated with eosinophilia. Intravenous vancomycin increased the risk of hemoglobin decreased regardless of dose. High-dose of vancomycin increase the risk of blood bilirubin increased. Due to the unclear relationship between dosage and serum vancomycin concentration in children, it is necessary to combine the results of this study with therapeutic drug monitoring in subsequent research and clinical practice.
There have been few studies on the incidence of vancomycin-related ADRs. Most research reported individual cases or only focused on a specific type of ADR such as nephrotoxicity,23,24 and red person syndrome. 9 In our study, the incidence of vancomycin-related ADRs was 66.7%, which was comprehensive. First of all, we employed the CHPS for data collection, which integrated with hospital-related information systems, including the hospital information system, laboratory information system, EMR, etc. This allows for the scientific and comprehensive collection of ADRs associated with drugs of interest and the total number of individuals taking the specific drug. Besides, to increase the comprehensiveness of vancomycin-related ADRs, we searched for all ADRs reported in FDA-approval labels or SmPC of vancomycin (VIANEX S.A.). The incidence of vancomycin-related ADRs in children still needs further validation with large-scale real-world data.
Only the normal-dose group showed a higher risk of eosinophilia. It was speculated that increased eosinophil count might indicate allergic reactions, which was a type 2-targeting biologic 25 that varied greatly among individuals and have less correlation with the dose. Previous studies have reported the association between vancomycin and eosinophilia and systemic symptoms (DRESS) syndrome, but these studies were mostly conducted in adults.26–28 It was reported that younger age was a risk factor for DRESS in adults. 26 Whether children are more likely to develop DRESS than adults still needs to be confirmed by large-scale studies. These studies speculated that vancomycin-induced eosinophilia might be related to genetic polymorphism and immune pathogenesis. Little evidence of the relationship between vancomycin and eosinophilia was reported. There was a case report that described a case of antibiotic-associated diarrhea in a 2-month-old infant treated with oral vancomycin. 29 After oral vancomycin treatment, the number of eosinophils increased significantly and the levels gradually recovered after drug withdrawal. 29 Similarly, the current study suggested that vancomycin use in children might lead to eosinophilia. Other antibiotics can be used instead for children with a potential risk of eosinophilia. When using vancomycin, physicians could reduce dosage while ensuring therapeutic efficacy and monitor the changes in eosinophil levels at the same time to reduce the risk of eosinophilia and even DRESS. On the other hand, monitoring eosinophils helps physicians detect eosinophilia as early as possible so that eosinophilia can be differentiated from other infections and treated promptly.
Anemia is the most common hematologic abnormality identified in infants and children. 30 Infection is an important cause of anemia in children. 30 To eliminate the impact of infection on the results, we matched the severity of infection between groups. The results showed that the incidence of hemoglobin decrease in the exposed group was higher than that in the unexposed group. Previous studies have established a two-step method for detecting the relationship between drugs and anemia using EMRs. 31 The incidence of anemia in this study among children was 54%, which was similar to that in the current study. Since hemoglobin levels may reflect the oxygenation of multiple organs, including the kidney, heart, and liver, and affect the excretion of vancomycin, 32 the hemoglobin level before and after using vancomycin should be closely monitored to prevent the occurrence of anemia among pediatric patients.
The current study found that using a high-dose of vancomycin increased the risk of blood bilirubin increased. The bilirubin level is one of the liver function indices. In previous meta-analyses of vancomycin and hepatotoxicity in the pediatric population, it was found that there was no statistically significant difference in the incidence of hepatotoxicity between the high trough concentration group and the low trough concentration group. 16 However, the relationship between dose and elevated bilirubin levels remains to be explored. A case analysis of hepatotoxicity caused by vancomycin found a total of 17 patients had abnormal aspartate aminotransferase/alanine aminotransferase levels, and 9 patients also had abnormal bilirubin levels among 4562 patients who received vancomycin. 33 These 9 patients were all adults. Blood bilirubin increased might be a new signal of vancomycin-related ADR in children. The potential mechanism is not yet clear. The mechanism of hepatoxicity is linked to oxidative stress and mitochondrial malignant lesions. 34 Previous studies have suggested that drugs with a high protein binding ability can result in significantly reducing the reserve albumin-bilirubin conjugates and further upregulating the bilirubin levels. 35 This situation only happened when the drug concentration and daily dosages were high. Since vancomycin has a medium protein binding ability, whether vancomycin affects bilirubin levels through this mechanism remains to be verified through further research. According to our results, clinical physicians and pharmacists should pay attention to the dosage of vancomycin and avoid using high-dose vancomycin in children with abnormal liver function or hyperbilirubinemia.
This evidence could be converted into CHPS trigger rules, embedded in daily diagnosis and physician prescriptions for early warning, prompting, and restriction. The system could automatically indicate that the child is at high risk of experiencing certain ADR when the physician prescribes vancomycin. It could also prompt that certain examinations should be conducted at the corresponding time point after using vancomycin. Using the systems above could prevent the occurrence of vancomycin-related ADRs in clinical practice. However, as the current study was a single-center study, the generalizability of the results would be limited. It is necessary to further conduct large-scale cohort studies in conjunction with multiple centers to explore the high-risk factors and high-risk populations of vancomycin-induced ADRs, providing more evidence for refining the CHPS trigger rules, guiding clinical medication, and accurately preventing vancomycin-related ADRs.
There were several strengths in our study. First of all, the utilization of the CHPS system to establish detection algorithms ensured comprehensive ADR signal detection in pediatrics receiving vancomycin. Moreover, the inclusion of an unexposed group facilitates correlation analysis to a greater extent. However, certain limitations of the study also should be noted. First, the causal relationship between doses of vancomycin and ADRs among children should be explored further due to the retrospective design. Though the nature of the retrospective cohort study is from cause to effect, some confounding factors may not be collected under control. Missing or nonstandard of this information might affect the results of the current study. A relatively small sample size for certain ADRs during the data collection phase might decrease the statistical power of the analyses and limit our exploration of more confounding factors and the effect of vancomycin dose in different subgroups. After collecting more sample data in the future, more in-depth research will be conducted to improve the reliability of our research. Besides, the current study did not explore the effect of serum vancomycin concentration on the ADRs due to missing therapeutic drug monitoring data on about 30% of patients. We will investigate the impact of serum concentration on ADRs in future research. Furthermore, due to limitations in the CHPS system, outpatient patients cannot be included in the analysis. The omission of outpatient patients with mild symptoms might cause an overestimation of ADR incidence. We will promote the integration of CHPS with the hospital outpatient system to obtain data from these patients. Finally, the data were derived from one center in Southeastern China. Most patients seeking medical treatment are from southern China, and there are differences in lifestyles and genetic information between the southern Chinese population and those from northern China or even Western countries. It might cause selection bias and limit extrapolation to other populations. The generalizability of the results to populations from northern China or even Western countries would be cautious. The multicenter studies are needed to increase the generalizability of our results.
Conclusions
The use of vancomycin in children is prone to ADRs. It is recommended to carry out routine medication monitoring. In addition to serious ototoxicity and nephrotoxicity, eosinophils, hemoglobin, and bilirubin also needed to be closely monitored.
Supplemental Material
Supplemental Material - Safety profiles of vancomycin in pediatrics based on China hospital pharmacovigilance system: A retrospective cohort study
Supplemental Material for Safety profiles of vancomycin in pediatrics based on China hospital pharmacovigilance system: A retrospective cohort study by Xiuming Pan, Zhijie Huang, Yao Chen, Weida Chen, Quanyao Chen, Zhiyi Huang, Jiemin Chen, Jianhui Yang and Can Cai in European Journal of Inflammation.
Footnotes
Acknowledgments
We appreciated the guidance of CHPS engineers.
Author contributions
Xiuming Pan and Zhijie Huang designed the study and drafted the manuscript. Weida Chen, Quanyao Chen, Zhiyi Huang, and Jiemin Chen contributed to the acquisition, analysis, and interpretation of the study. Yao Chen, Jianhui Yang, and Can Cai assisted in conception and designing, critically revised the manuscript, and gave final approval of the study. Jianhui Yang and Can Cai agreed to be accountable for all aspects of work, ensuring integrity and accuracy. All authors approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fujian provincial health technology project [2023QNB015].
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.