
Abstract
Objective
To describe the existing knowledge on the efficacy of the different gingival retraction systems (GRSs) in gingival displacement, to know their effects on biological functions of human gingival fibroblasts (HGFs), and on the expression of inflammatory mediators (TNF-α and MCP-1) in gingival crevicular fluid (GCF), and saliva.
Methods
The protocol used for this systematic review was registered in INPLASY: 202410005. A digital search was performed in the databases PubMed/MEDLINE, Scopus, Science Direct, Web of Science, and Google Scholar of the literature published in the English language in the last 17 years (from December 10th, 2006, to May 15th, 2023), and included retrospective randomized clinical studies, prospective, and in vitro experimental studies. In addition, PRISMA criteria were followed. The methodological validity of the selected articles was assessed using Joanna Briggs Institute (JBI) critical appraisal tool, and the modified Consolidated Standards of Reporting Trials checklist (CONSORT).
Results
27 articles published between 2006 and 2023 were evaluated. Six hundred 32 subjects, aged between 18 and 65, participated in the clinical studies. 93.7% of the studies assessed periodontally healthy patients, and only 6.3% evaluated patients with mild gingivitis. Also, 882 teeth were samples, of which the majority were posterior teeth (54%). The most commonly used GRSs was aluminum chloride gingival retraction paste (74%). The GCF samples were taken in 67% of the studies, and ELISA was used in all studies (100%) to determine inflammatory mediators. The most frequently analyzed marker was TNF-α (67%).
Conclusion
The system Merocel Strips (Mystic, conn, USA) achieved the highest level of gingival displacement (1.66 ± 3.7 mm). In addition, the braided cords produced the lowest TNF-α levels (0.43 ± 0.08pg/mL). Astringent systems such as ferric sulfate had higher toxicity in HGFs.
Keywords
Introduction
The main purpose of prosthetic restorations in addition to meeting the requirements of function, esthetics, and biocompatibility with the supporting tissues of the teeth is to preserve the remaining tooth structure1,2 and not just to make the decision to extract the tooth involved for the sake of replacing what is missing. 3 Periodontal health before, during and after prosthetic treatment is an important aspect of successful rehabilitation in the patient with this type of problem. 4 The formation of dentobacterial plaque in an inadequately placed prosthesis is an important etiological factor in the inflammation and consequent destruction of periodontal tissues. It has been shown that deep subgingival (below gingival) prosthetic margins that alter the biological thickness are associated with an increase in clinical parameters such as gingival index (GI), plaque index (PI), bleeding on probing (BP), probing depth (PD) and clinical attachment loss (CAL), which often tends to increase periodontal problems and complications such as gingival recession.5,6 However, with good training regarding maintenance of thorough oral hygiene by the patient, and good management of restorative and soft tissue procedures, periodontal health can be preserved.7–10 Notably, the prosthetic margin should be 0.5 mm from the healthy marginal ridge or 3-4 mm from the alveolar bone gingiva and follow the natural scalloping of the gingiva and alveolar process.11,12
Prosthetic restorations that are well contoured and have tight margins on the finishing line of the tooth preparation, especially when they are juxtagingival (same gingival level) or subgingival, are achieved thanks to an adequate impression taking13,14 preceded by the use of an excellent gingival retraction system (GRSs).15,16 The objective of using GRSs is: (1)The displacement of the marginal gingiva, that is, they allow the folding of the gingival margin at a considerable distance from the tooth surface, providing a virtual vertical and horizontal space between the tooth surface and the junctional epithelium where the impression material is to be applied. (2) At least 0.2 mm width in the sulcus is needed to decrease the risk of tearing of the impression material and a reduction in marginal accuracy. 3)In addition, it is important that a small amount of impression material flows past the preparation, this in turn will allow precise trimming of the recovered die. 17 In the face of failure to use GRSs, this would lead to compromised marginal integrity (failure to adequately reproduce the finishing line of the previously prepared teeth), recurrent caries, inflammation and destruction of the supporting tissues of the teeth. 18
Currently, there are two methods of gingival retraction, which include surgical procedures using electrosurgery, rotary curettage and lasers, 19 and non-surgical procedures, which include mechanical and chemo-mechanical methods that can be used individually or in combination. 20 In relation to chemo-mechanical methods, that is the use of retraction cords and medications, the chemical substances used are classified into vasoconstrictors such as α- and β-adrenergics, 21 astringents such as ferric sulfate, chloride, aluminum sulfate and potassium, 22 as well as wireless retraction methods, which include the use of biomaterials such as magic foam cord, retraction paste, retraction capsule, among others. 23 Depending on the case and the clinical scenario, a wide variety of gingival retraction techniques are required; however, scientific evidence suggests that the most commonly used displacement method is the chemomechanical technique.24,25 Presumably, the dentist and prosthodontist are familiar with the workflow of the clinical steps for determining the degree of lateral gingival displacement. In addition, several studies have compared the clinical efficacy of different GRSs as a function of the biomaterials and techniques used.26–41
Ideally, GRSs should be easy to apply and manipulate, should be mostly inexpensive and easily accessible, as well as should have antimicrobial activities and show less negative effects on the periodontium, that is, more biocompatible with the cells that constitute periodontal tissues. 25 In this regard, several in vitro studies have evaluated the biological effects of human gingival fibroblasts (HGFs) exposed to different GRSs, including activities such as cell viability and proliferation, cytoskeleton organization and reactive oxygen species (ROS) determination. This by applying chemicals such as α- and β-adrenergic vasoconstrictors, astringents and wireless. 40 Researchers are trying to find new drugs with less cytotoxic effects on these cells,42–49 and for the most part, it has been shown that, experimental gels based on 0.05% HCI-tetrahydrozoline in different dilutions (1:10 and 1:20) are biocompatible with periodontal tissues and can be considered as new chemical gingival retraction vasocontrictor agents.42–44,46
Therefore, this systematic review aimed: • To describe the clinical aspects of different GRSs on the effectiveness of gingival displacement. • To evaluate the effects of different GRSs on the biological functions of human gingival fibroblasts. • To evaluate the influence of different GRSs on the levels of inflammatory mediators TNF-α, and MCP-1 in GCF and saliva.
Materials and methods
The present study followed the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analysis). 50 The protocol used for this systematic review was registered in the International Platform of Registered Systematic Review and Meta-analysis Protocols (INPLASY) (202410005).
Review question
The protocol aimed to answer the following three questions: “Which GRSs have the greatest effectiveness on the degree of gingival displacement?” “Do GRSs affect the biological responses of gingival fibroblasts in vitro studies?” “What are the effects of GRSs on the levels of inflammatory mediators?” The questions followed the guidelines according to the PICOS strategy: • Population: Gingival tissues around teeth to receive fixed dental prostheses from adult subjects and gingival fibroblasts. • Intervention: GRSs; retraction cords, pastes, strips, lasers, and other chemicals. • Comparison: The previously mentioned methods served for comparisons. Also, teeth without pre-displacement. • Outcomes: Degree of clinical gingival displacement, the response of gingival fibroblasts to pre-displacement GRSs exposure, and levels of inflammatory mediators.
Eligibility criteria
The research focused on which type of GRSs are ideal for gingival sulcus impressions and those that measure the degree of gingival displacement; in vitro research studying the effects of different GRSs on the biological functions of fibroblasts such as cell morphology, viability, and cytotoxicity; and research on the influence of GRSs on the levels of different inflammatory mediators were included. Articles had to be published in English and have full text available. Original research, such as retrospective and prospective randomized clinical trials and in vitro experimental studies, were included in the present investigation. Studies that evaluated the response of cells other than gingival fibroblasts were eliminated. Case reports, editorials, short communications, and research conducted in a language other than English were excluded.
Electronic search
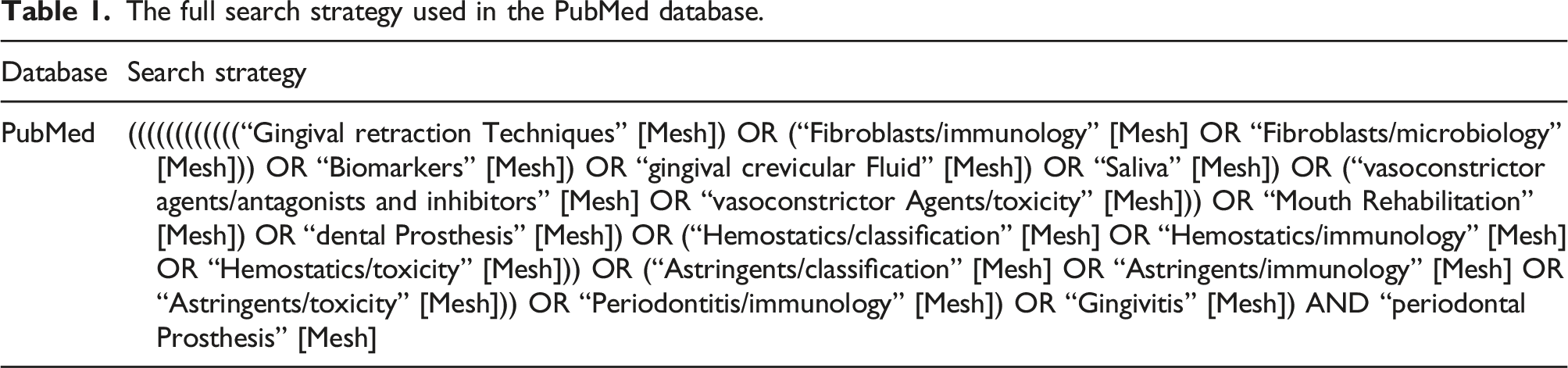
A digital search was performed in the databases PubMed/MEDLINE, Scopus, Science Direct, Web of Science, and Google Scholar for literature published in the English language in the last 17 years (from December 10th, 2006, to May 15th, 2023). The search was limited to humans and cells (gingival fibroblasts).
Manual search
The reference lists of the selected articles were checked for cross-references. In addition, additional hand searches were performed in the following journals from 2006 to 2023: Journal of Prosthodontics-Implant Esthetic and Reconstructive Dentistry, Journal of Prosthodontic Research, Journal of Advanced Prosthodontics, International Journal of Prosthodontics, European Journal of Prosthodontics and Restorative Dentistry, Journal of Esthetic and Restorative Dentistry, Journal of Prosthetic Dentistry, Journal of Indian Prosthodontics Society and Journal of Prosthodontics.
Search strategy
The full search strategy used in the PubMed database.
Methods of detection and data extraction
Two independent researchers (M.A.A.S and A.H) primarily screened the articles by reading the title and abstract. Subsequently, the content of each paper was summarized. The validity of the studies was assessed, and duplications were identified. The same investigators selected the articles that met the eligibility criteria or those with insufficient data. If any disagreement arose between the principal investigator, it was resolved by discussion with an independent third investigator. The following information was extracted for each article included: • First author, year, and country. • Type of study. • Journal. • Study population. • Age. • Gender. • Gingival retraction system used. • Location and number of teeth. • Periodontal status. • Cell type. • Technique used. • Oral fluid. • Method of detection. • Biomarkers.
Outcome measures
To evaluate the effects or influence of the different GRSs, the primary outcome was to determine the degree of gingival displacement and its possible impact on the condition of the periodontium. As a secondary outcome, articles evidencing the biological effects of gingival fibroblasts in response to GRS exposure were selected. As a tertiary outcome, articles that quantified the levels of different inflammatory mediators in response to the presence of GRSs on gingival margins were chosen.
Inclusion of evidence sources
Contribution of the selected studies to the outcome.

Quality assessment of the selected studies
The methodological validity of the selected articles was assessed independently by two investigators (M.A.A.S and A.H). For randomized clinical trials and longitudinal studies, the critical appraisal tool of the Joanna Briggs Institute (https://jbi.global/critical-appraisal-tools) was used. This tool is based on a series of questions grouped according to the type of studies included in the systematic review that can be rated as “Yes”, “No”, “Unclear” or “Not applicable”. The selected articles were ordered by their design and a specific instrument was used for each group. Whereas, for studies with an experimental design (in vitro studies), the modified Consolidated Standards of Reporting Trials (CONSORT) 51 checklist was used.
For practical purposes and according to the assessment instrument, the risk of bias was classified as high when the study reached up to 49% of the “Yes” scores, moderate from 50% to 69% and low when it reached scores above 70%.
Result
Study selection and characteristics
Initially, 2,081 articles were identified. After eliminating duplicate studies and studies with abstracts unrelated to the review’s three objectives, 81 potentially eligible articles were selected. Applying the eligibility criteria, 61 articles were selected, and 20 were excluded. After removing duplicates, a full-text analysis of the studies was performed, and 27 articles were finally obtained for qualitative research (Figure 1). Tables 3, 4, and 5 summarize the salient details of the studies.26–49,52–54 PRISMA flow diagram. PRISMA: Preferred Reporting Items for Systematic and Meta-Analyses. Summary of articles evaluating different GRSs on the level of lateral displacement and periodontal health. Summary of articles evaluating different GRSs on the biological effects of HGFs Summary of articles evaluating different gingival retraction systems on inflammatory cytokines levels. Abbreviations: Gingival crevicular Fluid-GCF; enzyme-linked Inmmunosorbent Assay-ELISA; Tumor Necrosis factor Alpha-TNF-α; monocyte Chemotactic protein 1-MCP-1; Aluminium chloride- AlCl3; ferric sulfate- Fe2(SO4)3; gingival retraction systems- GRS.



Most of the studies were published in countries on the European continent (33.3%), and Asia (25%). The 37% of the articles were published in India, 18.5% in Poland, 7.4% in New Zealand and Germany, while the rest (3.7%) were from Pakistan, Brazil, Turkey, Egypt, Taiwan, Slovenia, Serbia and the United States.
The following were included in the studies presented: Sixteen (59.2%) correspond to studies evaluating the effects of different GRSs on the level of gingival displacement, eight (29.6%) correspond to studies evaluating the biological impact of HGFs exposed to various GRSs, and only three (11.1%) analyzed the influence of GRSs on the levels of inflammatory cytokines. Most studies were published after 2018 (20 studies: 74%). 11 articles (40.7%) were prospective randomized clinical studies, eight (29.6%) were retrospective randomized clinical studies, and another eight studies (29.6%) were in vitro experimental studies. The journals in which each of the studies included in the review were published are also summarized.
Synthesis of results
Few studies suffered from a lack of detail in their report, that is, they did not mention age, sex, number of teeth, and location. Concerning the clinical studies, it was found that 632 subjects participated in the 19 included articles, with an age range between 18 and 65 years.
Influence of the GRSs on the level of gingival displacement
Most studies (93.7%) evaluated periodontally healthy patients, and only one (6.3%) evaluated patients with mild gingivitis. Regarding the latter study, 27 the authors demonstrated that periodontal status did not influence gingival height for any of the gingival displacement methods employed. It was only found that the mild gingivitis model worsened the sulcus representation when the cord technique was used, but did not influence the sulcus representation of the paste technique. Also, a total of 882 teeth were sampled, of which the majority were posterior teeth including premolars and molars (54%), 33% were anterior teeth including central incisors, lateral incisors and canines, and 13% did not specify the type of tooth. The most commonly used GRSs was aluminum chloride gingival retraction paste (74%), followed by chemical-free gingival retraction cord (53%), polyvinyl siloxane (43.3%), polyvinyl acetate strips, Er, Cr: YSGG laser and ferric sulfate (11%), as well as polytetrafluoroethylene, naphazoline hydrochloride and tetrahydrozoline (5.3%). It was also found that the Merocel Strips system (Mystic, conn, USA) achieved the highest level of gingival displacement with a mean of 1.66 mm , 40 while the Retraction Paste system (Expasyl, Pierre-Roland, Bordeaux, France) achieved the lowest level of gingival displacement with a mean of 0.4 mm. 36
Effect of GRSs on biological responses to HGFs
In this study, HGFs were the only cells evaluated (100%). The most commonly used technique was the MTT (3-(3,4 -dimethylthiazol-2-yl)-2,5- diphenyltetrazolium bromide) assay (50%) to measure cellular metabolic activity as an indicator of cell viability, proliferation, and cytotoxicity. This technique is followed by laser scanning confocal microscopy (37.5%) to assess the organization of the cytoskeleton. HGFs have been most frequently exposed to agents such as injection with 0.01 and 0.05% adrenaline (Self-made dilution of Injec. Adrenalini 0.1%), Visine® classic (Pfizer, Warsaw, Poland), Afrin® (Schering-Plough, Brussels, Belgium), Neosynephrin-POS® 10% (Ursaphamar, Saarbücken, Germany) and Starazolin® (Polpharma, Warsaw, Poland) (37.5%). In addition, astringent systems such as ferric sulfate produced higher toxicity in HGFs.
Inflammatory mediators production in GCF and saliva as a consequence of GRSs use
Two studies (67%) sampled gingival crevicular fluid (GCF), and only one study (33%) sampled saliva for the determination of inflammatory markers. In the three previously mentioned articles, the enzyme-linked immunosorbent assay (ELISA) was performed. In addition, the most frequently analyzed marker in GCF was TNF-α (67%), followed by MCP-1 (33%) which was only measured in saliva. Smooth knitted gingival retraction cord was found to maintain increased levels of TNF-α (16.08 ± 3.13 pg/mL) in GCF 28 days after the gingival displacement process; so far, the highest levels reported in the literature,
52
whereas braided cords (Ultrapak knitted retraction cord, #0, Ultradent, Inc, South Jordan, UT) produced the lowest levels of this cytokine (0.43 ± 0.08pg/mL).
54
Figure 2 shows a summary of the main characteristics of the clinical studies. Periodontal condition, inflammatory mediators and gingival retractions systems evaluated in the present systematic review. Abbreviations: No information: NI, Gingival Crevicular Fluid: GCF; Enzyme-linked immunosorbent assay: ELISA; Tumor Necrosis Factor Alpha: TNF-α; Monocyte Chemotactic Protein 1: MCP-1; Aluminium Chloride: AlCl3; Gingival Retraction Cord: GRC; Polyvinyl Siloxane: VPS; Polyvinyl Acetate Strips: PVA; láser Er,Cr: YSGG; Ferric Sulfate: Fe2(SO4)3; Polytetrafluoroethylene: PTFE; naphazoline hydrochloride: NH.
Quality assessment of the selected studies
Results of the quality assessment of randomized controlled trials.

Question (Q); Y, yes; N, no; U, unclear N/A, not aplicable.
Q1:Was true randomization used for assigment of participants to treatment groups?
Q2: Was allocation to treatment groups concealed?
Q3: Were treatment groups similar at the baseline?
Q4: Were participants blind to treatment assignment?
Q5: Were those delivering treatment blind to treatment assigment?
Q6: Were outcomes assessors blind to treatment assignment?
Q7: Were treatment groups treated identically other than the intervention of interest?
Q8: Was follow up complete and if not, were differences between groups in terms of their follow up adequately described and analyzed?
Q9: Were participants analyzed in the groups to wich they were randomized?
Q10: Were outcomes measured in the same way for the treatment groups?
Q11: Were outcomes measured in a realible way?
Q12: Was appropriate statistical analysis used?
Q13: Was the trial design appropiate, and any deviations from the standard RCT design (individual randomization, parallel groups) accounted for in the conduct and analysis of the trial?
Results of the quality assessment of longitudinal studies.

Question (Q); Y, yes; N, no; U, unclear N/A, not aplicable.
Q1: Were two groups similar and recruited from the same population?
Q2: Were the exposures measured similary to assign people to both exposed and unexposed groups?
Q3: Was the exposure measured in a valid and reliable way?Q4: Were confounding factors identified?
Q5: Were strategies to deal with confounding factors stated?
Q6: Were the groups/participants free of the outcome at the start of the study (or at the momento of exposure)?
Q7: Were the outcomes measured in a valid and reliable?
Q8: Was the follow up time reported and sufficient to be long enough for outcomes to occur?
Q9: Was follow up complete, and if not, were the reasons to loss to follow up described and explored?
Q10: Were strategies to address incomplete follow up utilized?
Q11: Was appropriate statistical analysis used?
Results of the quality assessment of experimental studies.

Answer; Y, yes; N, no; U, unclear N/A, not aplicable.Items
1: Abstract
2: Introduction
3: Methods (Intervention)
4: Methods (Outcomes)
5: Methods (sample size)
6: Methods (Randomisation: Sequence generation)
7: Methods (Randomisation: Allocation concealment mechanism)
8: Methods (Randomisation: implementation)
9: Methods (Randomisation: blinding)
10: Statistical methods
11: Results (outcomes and estimation)
12: Discussion (limitations)
13: Other information (funding)
14: Other information (protocol)
Discussion
Periodontitis is an inflammatory and destructive disease affecting the teeth’ supporting tissues. 55 It is multifactorial and has a high prevalence worldwide, estimated at 62.3%. 56 One of the factors leading to its development is the use of prosthetic restorations with poor marginal and internal fit, 57 whose influence is preceded, in addition to other factors, by the use of a poor gingival displacement technique. 17
In the clinic, it is not uncommon to find periodontal disease in the tooth at the time of gingival retraction and impression-taking. 58 This is the case in patients with poor oral hygiene or those who received a temporary fixed prosthesis before definitive prosthetic restoration and accumulated more dental bacterial plaque than usual, producing an inflammatory response.59,60 A study 27 proved that, under the influence of mild gingivitis, better gingival displacement in the vertical direction was achieved when the aluminum chloride double cord technique was used before the conventional impression. On the other hand, Thimmappa et al., 2018 in their study showed that employing chemomechanical methods using Merocel Strips (Mystic, conn, USA) achieved a gingival displacement of 1.66 mm, optimal for excellent reproduction of the post-impression tooth preparation line. The Merocel strips system is a synthetic material chemically extracted from the polymer hydroxylated polyvinyl acetate. This biomaterial expands with the absorption of the GCF, exerting moderate pressure on the adjacent gingival tissue, thus ensuring gingival displacement. On the other hand, in our study we found that, according to the results of Bennani et al., 2020, the use of gingival retraction paste (Expasyl, Pierre-Roland, Bordeux, France) achieved the lowest level of displacement with a medium of 0.4 mm. These results are similar to those reported by Kazemi and Loran, 61 who found greater gingival displacement with the use of cords presatured with AICI3, compared to Expasyl paste, however the latter caused less damage to the gingival tissues. In this sense, it has been shown that the GRS Expasyl, and Magic Foam Cord are two of the most biocompatible systems, as evaluated histologically, with respect to the periodontium. 62 Furthermore, contrary to these results, another study showed that good gingival displacement can be achieved with the use of Expasyl paste. 63 The Expasyl system is effective, and atraumatic, its viscosity has been calculated to open the gingival sulcus effectively, without damaging the epithelial insertion. Additionally, it is an excellent tool for CAD/CAM, ensuring a clearer aperture for taking digital impressions. It has a fast, simple, and affordable protocol, without the need for additional anesthesia or homeostasis, and guarantees good performance, that is, it generates a pressure 1.7 to 9.2 times higher than other retraction compounds avaibles on the market, sufficiente to allow the opening of the sulcus . 64
Therefore, it remains a controversial topic, which is why it deserves more research. It is important to choose a biomaterial that can offer adequate displacement, but at the same time is not so harmful to periodontal tissues. The findings of the present systematic review will further help to identify retraction biomaterials that are viable, can be used safely, and guarantee minimal impact on the periodontal health of the tooth. 65
The antimicrobial properties of GRSs have been little investigated compared with the degree of gingival displacement and their effects on the periodontium. 66 During placement of different GRSs in the gingival sulcus, laceration with consequent tissue inflammation may occur, facilitating the penetration of microorganisms (bacteria, viruses, fungi, protozoa) through the junctional epithelium and then reaching deeper gingival tissues.4,6,67 Therefore, a practical antimicrobial effect could reduce these complications. 68 It has been shown that systems such as Racestyptine, Retrax, Astringedent, and Astringedent X showed inhibitory activity against bacterial species such as Escherichia coli, Pseudomonas aeruginosa, Streptococcus gordonii, Streptococcus mitis and Streptococcus mutans, at the first and third minute of exposure, whereas, other agents (Hemodent) showed variable effects after 10 minutes. In addition, the most active systems reduced, but did not completely prevent, the metabolic activity of a monospecific biofilm. This study concluded that biofilm bacteria are less sensitive to the antimicrobial effects of the tested systems; however, more research is needed to clarify these observations in clinical practice.69,70 It would be interesting to evaluate the effects of other GRSs on putative and recognized periodontopathogenic (Porphyromonas gingivalis, Tannerella forsythia, and Treponema denticola) species (Campylobacter, Prevotella, and Fusobacterium species), as part of the bacterial species representative of gingivitis and periodontitis. For now, the clinician should be aware of the possible antimicrobial effects of some GRSs for use after tooth preparation and before conventional impression taking.
HGFs are essential cells in the periodontium 71 because they are responsible, on the one hand, for modulating the immune response against periodontopathogenic bacteria that invade the gingival tissue by producing a wide variety of inflammatory mediators leading to inflammation and destruction, as occurs in periodontitis 72 and on the other hand, the maintenance of tissue structure and integrity, since they produce most of the extracellular matrix, which is an essential aspect in the processes of repair, regeneration and wound healing. 73 Due to these properties, the biological response of HGFs after exposure to different GRSs is an essential scientific topic that requires detailed investigation. 74
It has been shown that different hemostatic agents based on aluminum chloride, aluminum sulfate, and ferric sulfate did not down-regulate HGF viability or proliferation and also did not show changes in cytoskeleton reorganization, except for Expasyl, which induced oxidative stress, demonstrated by increased nitrite level. Incubation with the previously mentioned agents significantly increased the RNA expression of some antioxidant enzymes such as SOD1, SOD3, and GPX1; however, no significant influence on the expression of SOD2 and HMOX1 was detected. The authors demonstrated that injectable forms of chemical retraction agents revealed biocompatibility with HGFs, suggesting their potential usefulness in the clinic for pre-impression gingival margin retraction. 42 Another study demonstrated by MTT assay that ferric sulfate-based GRSs were the most cytotoxic, followed by aluminum chloride and aluminum sulfate.45,48
On the other hand, vasoconstrictor-type agents such as α- and β-adrenergic solutions 0.05 and 0.01 epinephrine-HCI, 0.05% tetrahydrozoline-HCI, 0.05% oxymetazoline-HCI, 10% phenylephrine-HCI and three experimental gel formulations (EG-1, two and 3) based on 0.05% tetrahydrozoline-HCI, were used to treat HGFs. The experimental shrinkage gels did not limit the expression of type I and III collagen. GE-3 induced the synthesis of both types of collagen. An assay using the dichlorofluorescein fluorescent probe indicated oxidative stress similar to control cells for most of the selected retraction agents. 43 Another study published by the same working group found that the highest protein damage when using different chemical agents was observed in cells incubated with 0.1%, 0.01%, and 0.05% adrenaline. Also, they found a higher percentage of viable cells for HGFs incubated with the experimental gel n° 2, an increase in the expression of manganese dismutase superoxide enzymes in fibroblasts incubated with all GRSs and phenylephrine-HCI at 10% reduced the number of cells and abnormal rough actin appeared. Finally, they propose that the new 0.05% tetrahydrozoline-HCI-based gels are more biocompatible with periodontal tissues and can be applied as new chemo-mechanical vasoconstrictor-type GRSs.44–49
Gingival retraction procedures can cause direct damage to keratinocytes and fibroblasts of the gingival tissue with consequent production of inflammatory cytokines and chemokines and immunoglobulins in oral fluids (GCF, saliva and serum), as well as an increase in the number of immune cells such as; neutrophils, macrophages, dendritic cells and B and T cells, which leads to structural changes in the tissue, that is, the inflammatory and destructive process is initiated.6,75,76 It has been shown that using a single-point cord as a method of gingival retraction could modify some periodontal and inflammatory clinical parameters. On the one hand, it transiently increased the gingival index 1 day after its placement; however, it recovered to baseline at 14 days. On the other hand, TNF-α levels in GCF peaked on day one and then decreased in subsequent days; however, they were still elevated to 58% above baseline at day 28, suggesting persistence of the inflammatory state or a subclinical level of inflammation. 54 Similarly, in a clinical study published by Mathew et al., 2022 they compared the levels of TNF-α in GCF at three different times (30 min, 7 days, and 28 days) after gingival retraction by three methods by placing Expasyl retraction paste, Magic foam, and smooth point cord for identification of the least damaging system, they found that the minimum amount of inflammatory response was achieved with the Magic foam gingival retraction cord, where the levels of this cytokine reached almost baseline values in 28 days. The Expasyl retraction system, mainly through the use of the single stitch cord, increased TNF-α levels, nearly doubling at 28 days compared to baseline levels of this cytokine.
TNF-α is a proinflammatory and pleiotropic cytokine that serves different functions, 6 including promotion of myeloid cells and suppression of osteoblastic activity through negative regulation of osteocalcin, alkaline phosphatase, and the transcription factor RUNX2, which prevents osteoblast differentiation. However, it can also inhibit the wnt signaling pathway, downregulating osteoblast function and increasing apoptosis. Also, TNF-α increases osteoclastic activity by up-regulating the expression of RANKL or by RANKL-independent autocrine/paracrine signaling, mechanisms that result in bone resorption.72–74 Another vital function is the production of cytokines and chemokines, such as MCP-1/CCL2, a chemokine that attracts other immune cells to the site of injury, producing an inflammatory infiltrate that further perpetuates the inflammatory-destructive state of the periodontium.75–77 In fact, it has been shown that the rate of gingival bleeding and MCP-1 levels increase after chemical-mechanical gingival retraction procedures, with a tendency to decrease over time. In this case, clinical and immunologic changes were more evident after using ferric sulfate, although these changes were not significant. 53
It is worth mentioning that, in fixed dental prostheses, 18 different inflammatory mediators have been identified to date, such as IL-1α, IL-1β, IL-6, IL-8, TNF-α, IL1ra, CRP, PGE2, MIP-1, IgG, CX3CL1, resistin, aspartate aminotransferase, alkaline phosphatase and matrix metalloproteases such as MMP-2, MMP-8, aMMP-8 and MMP-9 in GCF and blood serum with the primary purpose of knowing and evaluating the inflammatory response as a consequence of their use and thus, to determine which biomaterials produce a less harmful effect on the supporting tissues of the teeth, a fact that is very relevant to improve the success of prosthetic therapy. Therefore, these molecules induce and maintain the inflammatory response in the periodontium, creating a vicious circle that accelerates the pathogenesis of the disease.6,78,79
To date, only three studies have been published that comparatively evaluate the effects produced by different gingival retraction systems (chemical-mechanical methods: Expasyl retraction paste, Magic foam, smooth point cord, single point, aluminum chloride, and ferric sulfate) on the amount of inflammation produced in response to TNF-α and MCP-1 levels in GCF and saliva. It would be fascinating to carry out future studies on the long-term effects of gingival retraction, with the use of other biomaterials and inflammatory mediators that show the dynamics of inflammation at the local level, that exert less damage to the periodontium and allow obtaining good results at the time of impression taking, all of the above to achieve the success of the prosthetic treatment.80,81
Limitations
The present systematic review shows some limitations that reflect the high heterogeneity observed. With respect to the primary outcomes, it is important to highlight that some studies did not take into account clinically relevant factors such as the type of tooth where the GRS is used, ease of application, retraction time, costs, and possible complications such as the existence of tissue trauma, and gingival recessions. These factors must be taken into account when it comes to the selection of biomaterials or gingival retraction methods, therefore more controlled studies are needed where such comparisons can be made. With respect to the secondary outcomes, the biological activities of other cell types such as gingival keratinocytes, which also constitute an important part of the cells of the gingival sulcus, were not taken into account. Finally, with respect to the tertiary outcomes, the small sample sixe, the period of time recorded, the biological samples collectes, and the lack os analysis of other inflammatory mediators that reflect the dynamics of infla,,ation upon exposure to different GRSs must be taken into account in future studies to achieve more consistent and representative results.
Conclusions
With the limitations of the present study, three primary outcomes were evaluated: The amount of gingival displacement, the biological effects of HGFs, and the levels of inflammatory cytokines in response to the use of the different GRSs. Despite the heterogeneity of the results, the following conclusions were • Molars and premolars were the teeth most frequently used to test GRSs. • The GRS most used by the authors was a gingival retraction paste with aluminum chloride. • The system: Merocel Strips (Mystic, conn, USA) achieved the highest level of gingival displacement (1.66 ± 3.7 mm), while the retraction paste system (Expasyl, Pierre-Roland, Bordeaux, France) achieved the lowest level of gingival displacement with a mean of 0.4 mm. • Astringent systems such as ferric sulfate produce more significant toxicity in HGFs. The experimental gels based on 0.05% HCI-tetrahydrozoline in different dilutions (1:10 and 1:20) are biocompatible with periodontal tissues and can be considered as new chemical gingival retraction vasocontrictor agents. • The most frequently analyzed biomarker was TNF-α in GCF. In addition, smooth knitted gingival retraction cord was found to maintain increased levels of TNF-α (16.08 ± 3.13 pg/mL) in GCF 28 days after the gingival displacement process, while braided cords (Ultrapak Knitted retraction cord, #0, Ultradent, Inc, South Jordan, UT) produce the lowest levels of this cytokine (0.43 ± 0.08pg/mL).
We encourage continuing to carry out randomized controlled trials of high-quality in vivo and in vitro studies to generate sufficient data to find the appropriate GRSs with less harmful effects on the periodontium but at the same time achieving good levels of gingival displacement, which will allow a better impression of the dental preparation line. An exact reproduction of this anatomical structure, in combination with the use of CAD/CAM technology, will generate better prosthetic devices.
Footnotes
Author contributions
Mario Alberto Alarcón-Sánchez: Conceptualization, Methodology, Software, Validation, Formal analysis, Investigation, Resources, Data Curation, Writing - Original Draft, Writing - Review and editing, Visualization, Supervision, Project administration. Artak Heboyan: Formal analysis, Writing - Review & Editing, Project administration. Giuseppe Minervini: Formal analysis, Writing - Review & Editing, Project administration.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The data supporting this study’s findings are available from the corresponding author upon reasonable request.