
Abstract
Gingival overgrowth is a serious side effect that accompanies the use of amlodipine. Several conflicting theories have been proposed to explain the fibroblast’s function in gingival overgrowth. To determine whether amlodipine alters the inflammatory responses, we investigated its effects on gingival fibroblast gene expression as compared with untreated cells. Fragments of gingival tissue of healthy volunteers (11 years old boy, 68 years old woman, and 20 years old men) were collected during operation. Gene expression of 29 genes was investigated in gingival fibroblast cell culture treated with amlodipine, compared with untreated cells. Among the studied genes, only 15 (CCL1, CCL2D, CCL5, CCL8, CXCL5, CXCL10, CCR1, CCR10, IL1A, IL1B, IL5, IL7, IL8, SPP1, and TNFSF10) were significantly deregulated. In particular, the most evident overexpressed genes in treated cells were CCR10 and IL1A. These results seem to indicate a possible role of amlodipine in the inflammatory response of treated human gingival fibroblasts.
Introduction
There are many drugs, which may induce gingival overgrowth, although a large range of clinical manifestations can also result in gingival overgrowth. The drug-induced gingival overgrowth is a side effect of drugs used mainly for non-dental treatment for which the gingival tissue is not the intended target organ.1,2
The term gingival overgrowth indicates histopathological diagnosis of gum enlargement and has multiple causes. Drugs are among the most common culprit. Their effects have been associated with a patient’s genetic predisposition.3,4
More than 20 drugs are associated with gingival overgrowth.3,5 The three main classes of drugs are anticonvulsants, immunosuppressive agents, and antihypertensive agents.3–7 The first report about gingival overgrowth by administration of amlodipine was reported by Seymour et al. 8 Subsequently, Lafzi et al. 9 reported the onset of gingival overgrowth as side effect in patients who received 10 mg per day of amlodipine within 2 months. Gingival overgrowth manifests as side effect within 1 to 3 months after amlodipine administration.7,10 Amlodipine shows pharmacological profile as follows: long-acting dihydropyridine, coronary and peripheral arterial vasodilatation, headaches, facial flushing, dizziness, and edema. The main oral side effect is amlodipine-induced gingival overgrowth (AIGO).11,12
To determine whether amlodipine can alter the inflammatory responses, we investigated its effects on gingival fibroblast cell culture, analyzing the gene expression profile of treated cells.
Materials and methods
Primary human fibroblast cell culture
Fragments of gingival tissue of healthy volunteers (11 years old boy, 68 years old woman, and 20 years old men) were collected during operation. The pieces were transferred in 75 cm2 culture flasks containing Dulbecco Modified Eagle Medium (DMEM) (Sigma-Aldrich, Inc., St. Louis, MO, USA) supplemented with 20% fetal calf serum (FBS) and antibiotics (Penicillin 100 U/mL and Streptomycin 100 µg/mL: Sigma-Aldrich, Inc.).
Cells were incubated at 37°C in a humidified atmosphere with 5% CO2. The medium was changed the next day and twice a week. After 15 days, the pieces of gingival tissue were removed from the culture flask. Cells were harvested after additional 24 h of incubation.
Cell viability test
A stock solution of amlodipine 1 mg/mL was prepared. Further dilutions were made with the culture medium to the desired concentrations just before use.
Cell lines were seeded into 96-well plates at a density of 104 cells per well containing 100 µL of cell culture medium and incubated for 24 h to allow cell adherence.
Serial dilutions of amlodipine (5000, 2000, 1000, 500, and 100 ng/mL) were added (three wells for each concentration). The cell culture medium alone was used as a negative control.
After 24 h of incubation, cell viability was measured using PrestoBlue™ Reagent Protocol (Invitrogen, Carlsbad, CA, USA) according to the manufacturer’s instructions. Briefly, the PrestoBlue™ solution (10 µL) was added into each well containing 90 µL of treatment solution. Plates were then placed back into the incubator for 1 h, after which absorbance was measured at wavelengths of 570 nm excitation and 620 nm emission by an automated microplate reader (Sunrise™, Tecan Trading AG, Mӓnnedorf, Switzerland). The percentage of viable cells was determined by comparing the average absorbance in drug treated wells with average absorbance in control wells exposed to vehicle alone. The results were presented as the mean ± standard deviation of three measures.
Cell treatment
Cell lines were seeded at a density of 105 cells/mL into 9 cm2 (3 mL) wells and subjected to serum starvation for 16 h at 37°C.
Cells were treated with 1000 ng/mL amlodipine solution for 24 h. This solution was obtained in DMEM supplemented with 2% FBS, antibiotics, and aminoacids. Cell medium alone was used as a negative control.
The cells were maintained in a humidified atmosphere of 5% CO2 at 37°C. After the end of the exposure, time cells were trypsinized and processed for RNA extraction.
RNA isolation, reverse transcription, and quantitative real-time polymerase chain reaction
Total RNA was isolated from cell lines using GenElute Mammalian Total RNA Purification Miniprep Kit (Sigma-Aldrich, Inc,), according to manufacturer’s instructions. Pure RNA was quantified at NanoDrop 2000 spectrophotometer (Thermo Fisher Scientific, Wilmington, DE, USA).
Complementary DNA (cDNA) synthesis was performed starting from 500 ng of total RNA, using PrimeScript RT Master Mix (Takara Bio, Inc., Kusatsu, Japan). The reaction was incubated at 37°C for 15 min and inactivated by heating at 70°C for 10 s. cDNA was amplified by real-time quantitative polymerase chain reaction (PCR) using the ViiA™ 7 System (Applied Biosystems, Foster City, CA, USA).
All PCR reactions were performed in a 20 µL volume. Each reaction contained 10 µL of 2× qPCRBIO SYGreen Mix Lo-ROX (PCR Biosystems, Ltd, London, UK), 400 nM concentration of each primer, and cDNA.
Custom primers belonging to the “Inflammatory Cytokines and Receptors” pathway were purchased from Sigma-Aldrich, Inc. All experiments were performed including non-template controls to exclude reagents contamination. PCR was performed including two analytical replicates.
The amplification profile was initiated by 10 min incubation at 95°C, followed by two-step amplification of 15 s at 95°C and 60 s at 60°C for 40 cycles. As final step, a melt curve dissociation analysis, was performed.
Statistical analysis
The gene expression levels were normalized to the expression of the reference gene (RPL13) and were expressed as fold changes relative to the expression of the untreated cells. Quantification was done with the delta/delta Ct (threshold cycle) calculation method. 13
Results
PrestoBlue™ cell viability test was conducted to determine the optimal concentration of amlodipine to be used for cell treatment that did not significantly affect cell viability. Basing on this test, the concentration used for the treatment was 1000 ng/mL.
The gene expression profile of 29 genes belonging to the “Inflammatory Cytokines and Receptors” pathway was analyzed using real-time PCR (Figure 1). Table 1 reported the list of the investigated genes and their fold change.
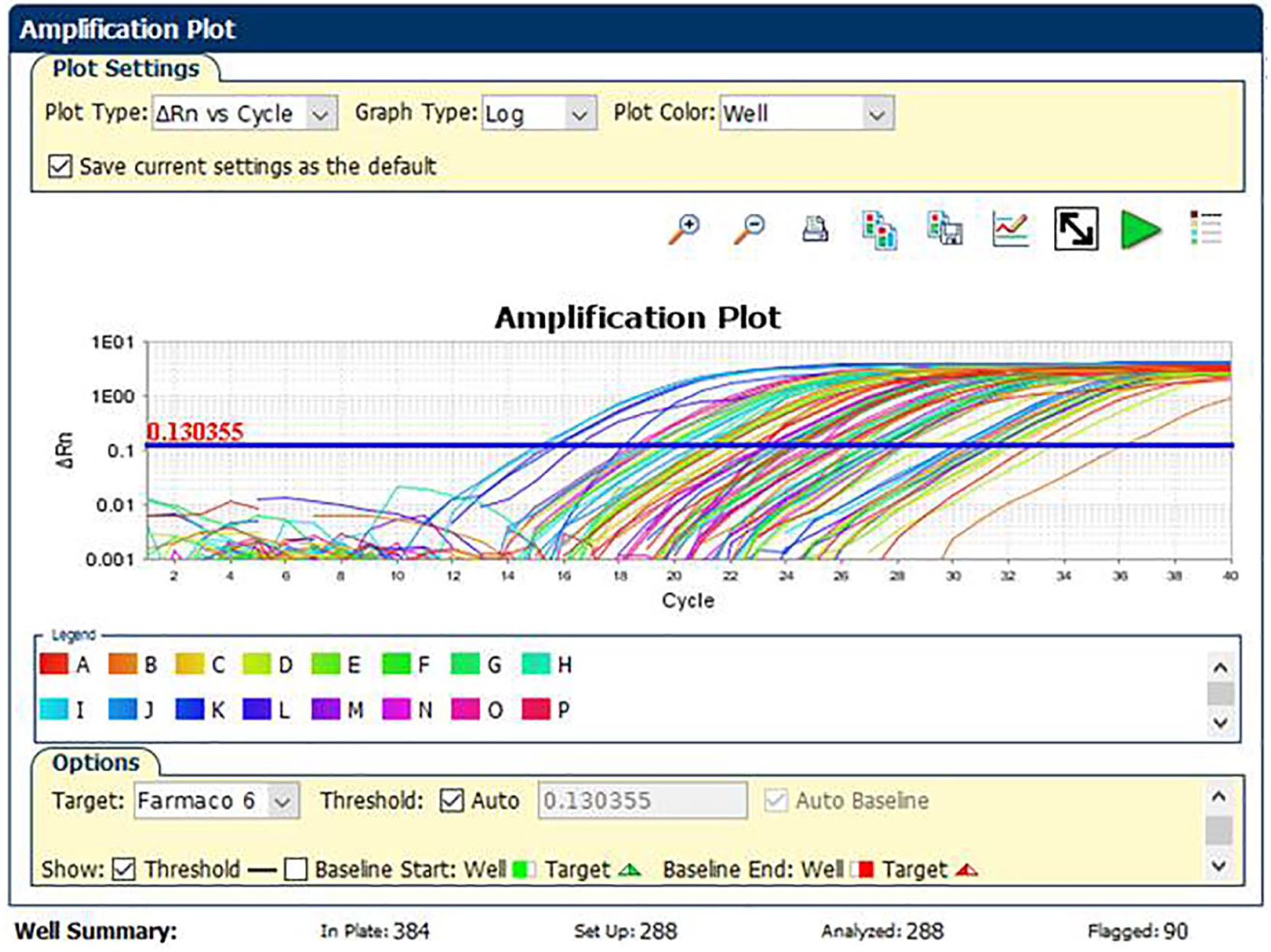
Amplification plot curves of the 29 genes belonging to the “Inflammatory Cytokines and Receptors” pathway analyzed using real-time PCR.
Selected genes tested in real-time PCR and belonging to “Inflammatory Cytokines and Receptors” pathway.

PCR: polymerase chain reaction.
In bold the fold change of significant gene expression level.
Bold font indicates significant variation of gene expression level: fold change ⩾2 and P value ⩽0.05 for upregulated genes, and fold change ⩽0.5 and P value ⩽0.05 for significantly down-regulated genes. Table 2 reported the only significantly deregulated genes.
Significant gene expression levels after 24 h treatment with amlodipine, as compared with untreated cells.

SD: standard deviation.
In particular, the following genes were significantly down-regulated: CCL1, CCL2D, CCL5, CCL8, CXCL5, CXCL10, CCR1, and IL8 (Table 2, Figure 2).
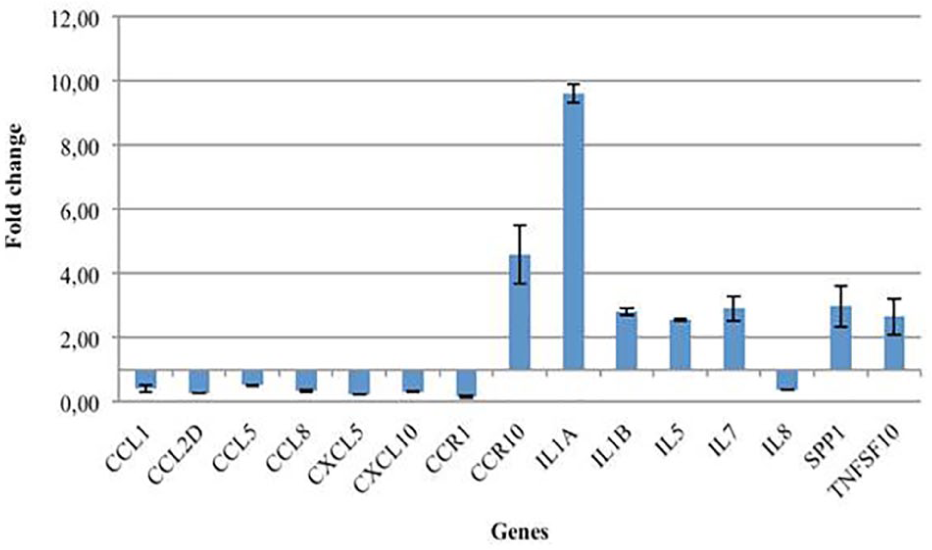
Gene expression profile of fibroblasts treated with amlodipine 1000 ng/mL.
Amlodipine treatment seems to increase the expression of CCR10 and of many genes coding for interleukins such as IL1A, IL1B, IL5, and IL7. Other significantly up-regulated genes are SPP1 and TNFSF10. In particular, the most significant results were obtained for the CCR10 and IL1A genes, fold change of which is, respectively, 4.59 and 9.61.
Discussion
The prevalence of AIGO might be as high as 38%. AIGO is 3.3 times more common in men than in women. 14 Since the mechanisms of action may be different for different drugs, the oral manifestation of AIGO is similar. AIGO starts as an enlargement of the interdental papilla of keratinized portions of the gingiva, followed by the increase of connective tissue components and gingival inflammation. This suggests that AIGO is a consequence of the interaction between gingival fibroblasts, cellular and biochemical mediators of inflammation, and drug metabolites.15,16
Gingival overgrowth is a more frequent side effect of anticonvulsant such as nifedipine and also of drugs such as amlodipine, verapamil, nicardipine, nitrendipine, oxodipine, felodipine, and diltiazem. 15 Furthermore poor oral hygiene is indicated as an important risk factor for the expression of AIGO.17,18
The underlying mechanism of AIGO still remains to be fully understood; however, two main inflammatory and non-inflammatory pathways have already been suggested.19,20 One hypothesis of pathogenesis of AIGO is referred to alteration of collagenase activity as a consequence of decreased uptake of folic acid, blockage of aldosterone synthesis in adrenal cortex, and consequent feedback increase in the adrenocorticotropic hormone level and upregulation of keratinocyte growth factor. Besides, inflammation may be as a consequence of toxic effect of amlodipine in periodontal pocket associated with periodontal pathogens leading to the upregulation of several cytokine factors such as transforming growth factor–beta 1 (TGF-β1).9,19,21 Current studies on the pathogenetic mechanism of AIGO are focusing on the direct and indirect effects of these drugs on gingival fibroblast metabolism. Only a subgroup of patients treated with amlodipine will develop AIGO, so it has been hypothesized that these individuals show an abnormal susceptibility to the drug. In fact, elevated levels of protein synthesis, most of which is collagen, characterize fibroblast of AIGO in these patients.
To determine whether amlodipine alters the inflammatory responses, we investigated its effects on gingival fibroblast gene expression as compared with untreated cells.
The genes analyzed belong to the pathway of “Inflammatory Cytokines and Receptors.” Fibroblasts derived from gingiva of healthy volunteers were treated for 24 h with a solution of amlodipine 1000 ng/mL.
The most significantly deregulated genes indicating an inflammatory action of amlodipine are IL1A, IL1B, IL5, IL7, and CCR10 that turned out to be upregulated in treated cells respect to control.
In particular, the most significant results were obtained for the CCR10 and IL1A genes, fold change of which is, respectively, 4.59 and 9.61.
CCR10 is normally expressed by melanocytes, plasma cells, and skin-homing T cells. Its ligand CCL27, synthesized by keratinocytes, is induced by tumor necrosis factor–alpha and IL1B. CCR10–CCL27 interaction is involved in T-cell migration during skin inflammation and is overexpressed in patients with psoriasis and atopic and allergic dermatitis.22,23
Another gene significantly upregulated in fibroblast treated with amlodipine was IL1A.
IL-1 is a proinflammatory cytokine that regulates several genes that amplify or support inflammation, such as prostaglandins, metalloproteinases, adhesion molecules on leukocytes, and chemokines which are needed to recruit circulating leukocytes.
The inflammatory activity of IL1A has been widely demonstrated in vivo experiments conducted on mice, in which the deletion of the gene leads to a reduction of the inflammatory response exposing them to many types of infections.24,25
The results obtained in this study seem to indicate a possible role of amlodipine in the inflammatory response of treated human gingival fibroblasts.
Treatment of AIGO is generally targeted on drug substitution and preventive protocols.12,26,27 When these measures fail to cause resolution of AIGO, surgical intervention is recommended.
Finally, the emphasis is that AIGO could be a side effect even with a very short-term and low-dose administration. 18
Gingival overgrowth is associated with periodontal disease also, and periodontal disease is of underestimated importance for global health.28,29 A thorough and early diagnosis of periodontal disease allows a more accurate risk calculation for developing systemic pathologies.30 –32 If a causative relationship is established between periodontal disease and these pathologies, therapeutic management of periodontal disease will become part of their prevention.33 –35
Dentists should be able to identify the changes in the oral cavity related to the general health of their patients. Patients must be informed of the tendency of certain drugs to cause gingival overgrowth and the associated oral changes, and the importance of effective oral hygiene.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.