A patient presented with erythema and oedema on the right eyelid, malar region and left thigh with pruritus and pain. She was diagnosed with erysipelas and had been treated with anti-inflammatory drugs, but the symptoms did not improve. Laboratory investigation and biopsy showed that she was consistent with lupus erythematosus tumidus. It's a typical and rare diease relatively.
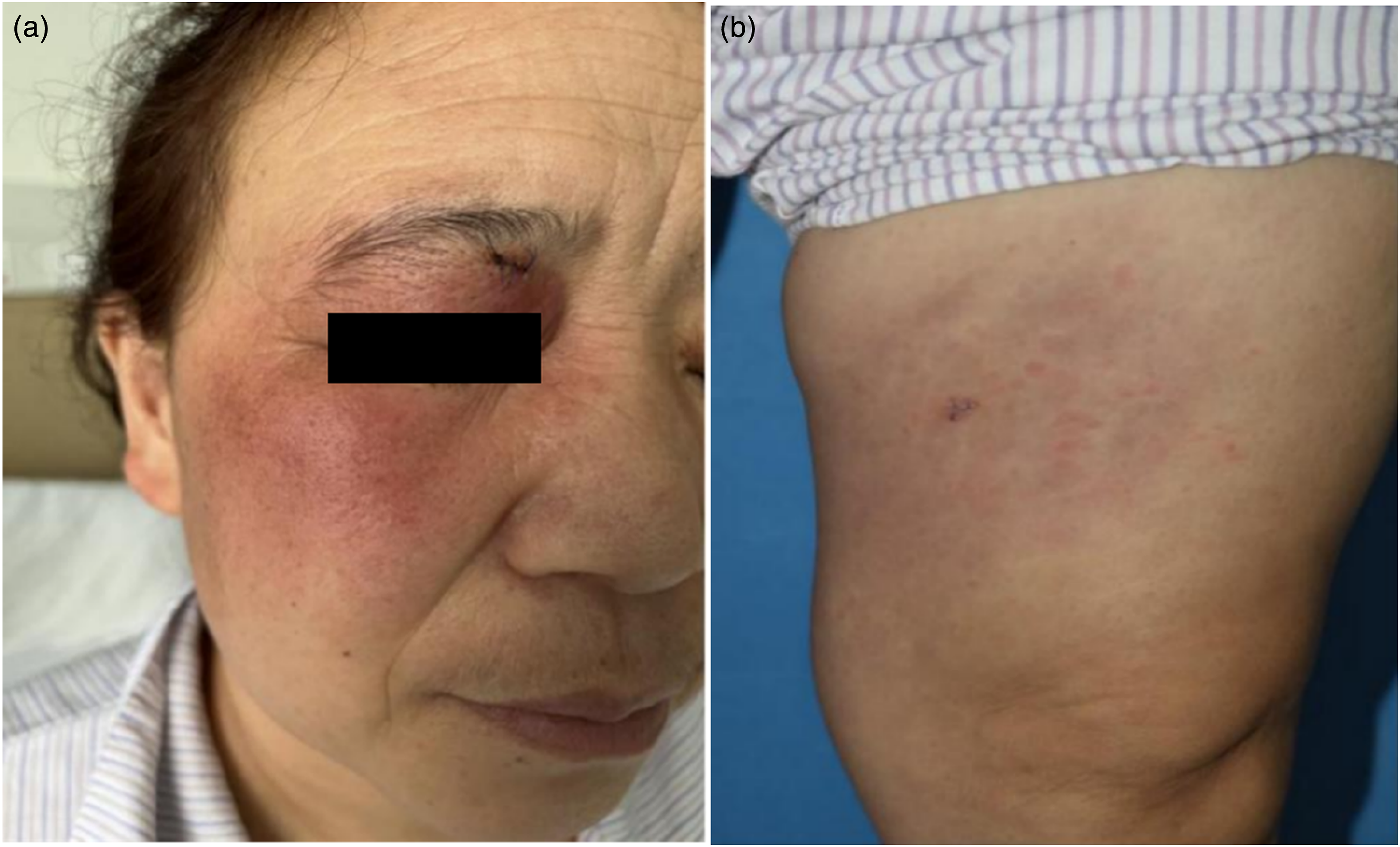
A 50-year-old female patient presented with erythema and oedema on the right eyelid, malar region and left thigh with pruritus and pain for 3 months (Figure 1
(A) Swelling purplish red patch distributed in right eyelid and malar region, with unclear boundary, smooth surface and no scaling; (B) On the left thigh, there is violaceous patch with unclear boundary.
). She was diagnosed with erysipelas and had been treated with antibiotics such as penicillin, azithromycin and cephalosporin (the specific treatment was unknown) in a local clinic. The symptoms did not improve, then she was admitted to our department. The patient was otherwise healthy with no fever, oral ulcer, arthralgia, alopecia, phototsensitivity. Laboratory investigation demonstrated anti-nuclear antibodies (ANA), anti-dsDNA antibodies, anti-SM antibodies, anti-SSA/Ro antibodies, anti-SSB /La antibodies, and anti-cardiolipin antibodies were all negative; routine blood tests including erythrocyte sedimentation rate (ESR), procalcitonin, C-reactive protein were within normal range. Biopsy of the left thigh revealed mild hyperkeratosis of epidermis, irregular proliferation of spinous layer, spongy edema, periadnexal and perivascular lymphocytes and histiocytes infiltrate were present with concomitant mucin deposition throughout the dermis (Figure 2
(A)The pathological examination of the left thigh showed mild hyperkeratosis of epidermis, irregular proliferation of spinous layer, spongy edema, periadnexal and perivascular lymphocytes and histiocytes infiltrate were present with concomitant mucin deposition throughout the dermis. (H&E staining, ×100); (B) Alcian blue staining revealed interstitial mucin deposition(Alcian blue staining, ×40).
). The clinicopathological findings were consistent with lupus erythematosus tumidus (LET) except for the unusual localization and absence of photosensitivity. Intravenous drip methylprednisolone sodium succinate 40 mg per day and oral hydroxychloroquine sulfate tables 0.2 g twice a day were administered to the patient for 7 days, then she responded well to treatment and discharged. The patient was instructed to avoid sun exposure, after a follow-up period of 2 months, the erythematosus subsided completely. LET is considered as a subtype of chronic cutaneous lupus erythematosus (CCLE), however, some scholars claiming that LET should be considered a separate entity from other forms of lupus. It also has been reported to co-exist with discoid lupus erythematosus (DLE), and systemic lupus erythematosus (SLE). Only tiny minority of cases have been described in which LET lesions converted to DLE type lesions over time 1 or DLE converted to LET.2 The pathogenesis of LET is still unclear, it has been confirmed that ultraviolet light,3 the use of certain medications such as angiotensin-converting enzyme inhibitors,4 long-term use of estrogen, adalimumab, infliximab,5 bortezomib,6 smoking,7 trauma and other factors may induce or aggravate LET. Clinically, it is characterized by edematous erythematous-violaceous urticarial lesions in sun-exposed areas that leave no scars or post inflammatory hyper or hypopigmentation, individual cases have symptoms of alopecia areata.2 Furthermore, LET rarely in connection with systemic disease or specific autoimmune antibodies.8 Histologically, LET shows intact epidermis or slight changes, a superficial and deep perivascular and periadnexal lymphocytic infiltration of the skin with prominent mucinous dispositions. Some changes are minimal alterations of the epidermis or the dermoepidermal junction, such as slight vacuolar degeneration, or even the absence of mucin dispositions.7 The preferred treatment is antimalarial drugs,9 which can be combined with glucocorticoids, immunosuppressants, topical steroid hormone creams, etc. It has been reported that tildrakizumab,10 and rituximab,11 were successfully used to treat refractory LET. These literature indicated that biologic may be potential therapeutic options for refractory LET. The diagnosis of LET is often delayed and can often be confused with other skin diseases because of its lack of systemic presentation. Erysipelas is characterized by acute inflammation of the skin and subcutaneous tissue with erythema and oedema present. Laboratory tests show an elevated ESR and leukocytosis with an increased percentage of polymorphonuclear neutrophils. The lesions of our patient were similar to erysipelas, but the laboratory indicators and systemic symptoms were not consistent and antibiotics therapy didn’t work. In addition, the histopathological examination showed mild hyperkeratosis of epidermis, typical periadnexal and perivascular lymphocytes and histiocytes infiltrate and concomitant mucin deposition in our case. These are all consistent with LET. So, it reminds us histopathological examination is essential in the establishing the diagnosis of LET. LET is commonly been underestimated, and neglected in clinical practice by many local clinical doctors, it’s a good case for us to learn from. A case of LET which skin lesion confined to the thigh was reported abroad.12 Sun also reported a LET manifest as a giant edematous erythema and involving half of the entire face asymmetrically.13 Chen reported a case of LET converted from DLE with prominent swelling of the eyelids, a low-grade fever and myalgia, which was also diagnosed as erysipelas at the local hospital.2 A LET patient with photosensitivity medical history presented with multiple asymptomatic erythematous plaques on her back was described.6 In this case, the lesions involved the eyelid, malar region and thigh, the distribution of skin lesions is rare. In conclusion, we report a unique case of LET characterized by unusual localization and without photosensitivity. As previously described that patients with LET were even more photosensitive than other cutaneous lupus.14
Footnotes
Acknowledgements
We would like to thank the patient for her support and consent to be published.
Author’s contribution
C-LZ and J-FZ performed the pathological studies, laboratory testing and clinical data collection. QZ and Y-LZ were in charge of patient care and drafted this manuscript. G-QZ revised the manuscript critically for important intellectual content. All authors contributed to the article and approved the submitted version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval to report this case was obtained from *the Ethics Committee of the First Hospital of Hebei Medical University (APPROVAL NUMBER/ID 20,221,024) *.
Informed consent
Written informed consent was obtained from the patient for her anonymized information to be published in this article.
ORCID iD
Guoqiang Zhang
References
1.
JollyMLaumannAESheaCR, et al.Lupus erythematosus tumidus in systemic lupus erythematosus: novel association and possible role of early treatment in prevention of discoid lupus erythematosus. Lupus2004; 13(1): 64–69.
2.
ChenXWangSLiL. A case report of lupus erythematosus tumidus converted from discoid lupus erythematosus. Medicine (Baltimore)2018; 97(16): e0375.
3.
GrönhagenCMNybergF. Cutaneous lupus erythematosus: An update. Indian Dermatol Online J2014; 5(1): 7–13.
4.
SchepisCLentiniMSiragusaM, et al.ACE-inhibitor-induced drug eruption resembling lymphocytic infiltration (of Jessner-Kanof) and Lupus erythematosus tumidus. Dermatology2004; 208(4): 354–355.
5.
SchneiderSWStaenderSSchlüterB, et al.Infliximab-induced lupus erythematosus tumidus in a patient with rheumatoid arthritis. Arch Dermatol2006; 142(1): 115–116.
6.
BöckleBCBaltaciMWeyrerW, et al.Bortezomib-induced lupus erythematosus tumidus. Oncologist2009; 14(6): 637–639.
PatsinakidisNGambichlerTLahnerN, et al.Cutaneous characteristics and association with antinuclear antibodies in 402 patients with different subtypes of lupus erythematosus. J Eur Acad Dermatol Venereol2016; 30(12): 2097–2104.
9.
KiriakidouMChingCL. Systemic Lupus Erythematosus, Ann Intern Med2020; 172(11): Itc81–itc96.
KreuterATiggesCHunzelmannN, et al.Rituximab in the treatment of recalcitrant generalized lupus erythematosus tumidus. J Dtsch Dermatol Ges2017; 15(7): 729–731.
12.
HashimotoTKawakamiYWakabayashiH, et al.An unusual clinical presentation of lupus erythematosus tumidus localized on the thigh. Clin Exp Dermatol2017; 42(6): 638–641.
13.
SunJYangXZhuX, et al.Hemifacial erythema: an unusual manifestation of lupus erythematosus tumidus. Rheumatology (Oxford)2021; 60(1): 476.
14.
KuhnARichter-HintzDOslisloC, et al.Lupus erythematosus tumidus--A neglected subset of cutaneous Lupus erythematosus: report of 40 cases. Arch Dermatol2000; 136(8): 1033–1041.