
Abstract
Objectives and Introduction
The purpose of this study was to determine the prevalence and influencing factors of systemic lupus erythematosus (SLE) patients complicated with infection having multi-system involvement and to analyze the influencing factors of early CMV and fungal infection.
Methods
We conducted a cross-sectional study of hospitalized SLE patients complicated with infection. Participants had an average age of 44.80 ± 17.30, with 152 being female (89.94%). Clinical data and laboratory results were collected from medical records. Receiver operating characteristic (ROC) curves were plotted, and sensitivity and specificity were calculated.
Results
Univariate analysis showed that systemic lupus erythematosus disease activity index-2000 (SLEDAI-2k), red blood cell, platelets, hemoglobin, lymphocytes, IgG, IgM, C3, C4, albumin and globulin were significantly associated with SLE patients with infection complicated with multi-system involvement. After multivariable analysis, the following variables remained significant: Hemoglobin, CD4 lymphocyte, IgM and SM (p < 0.05). ROC curve analysis showed the areas under the curve of Hb, CD4 count, and IgM for the differential diagnosis of SLE with infection complicated with multisystem involvement being 0.646, 0.627, and 0.610. Then, the sensitivities of 73.3%, 53.3%, and 73.3% were observed with the specificities of 54.1%, 69.7%, and 48.6%, respectively.
Conclusions
Our results demonstrated that hemoglobin, CD4 lymphocyte value, IgM and anti SM antibody had significant value in monitoring multi-system involvement in SLE patients complicated with infection. Besides, intrinsic lymphatic count disturbances associated with SLE disease can cause infections by opportunistic pathogens such as fungi.
Introduction
Systemic lupus erythematosus (SLE) is a complex autoimmune multi-system disease with high clinical heterogeneity and significant potential incidence rate and mortality. 1 Although SLE cannot be cured, it can be effectively treated with drugs. A population-based study of SLE in the United States showed that the overall age standardized mortality rate decreased by 24.4% over a 46-year period, 2 which may be due to treatment progress and early diagnosis.
However, the mortality rate of SLE patients is still about two to three times higher than that of the general population, especially women. 2 To date, the relative risk of hospitalization for severe infection in SLE patients is 12 times that of non-SLE patients, 3 and infection has become one of the leading causes of death in SLE patients. 4 Infections can induce, exacerbate, and perpetuate SLE by decreasing immune tolerance. 5 As for the pathogenic flora, bacteria caused the most infections, followed by viruses and fungi. 6
SLE has a variety of phenotypes, with varying clinical manifestations of patients from mild mucosal skin manifestations to multiple organs and severe central nervous system involvement, 7 therefore they usually require longer hospital stays and more complex treatment options. Although factors linked to infection in patients with SLE have been extensively investigated previously,8,9 our knowledge about variables associated with SLE patients complicated with infection having multi-system involvement is extremely limited.
Therefore, the main purpose of this cross-sectional study is to further examine the influencing factors of SLE infection complicated with multi-system involvement and the influencing factors of some opportunistic pathogens.
Patients and methods
Study design
This is an observational, cross-sectional study of SLE complicated with infection patients treated in a single Rheumatology Department to evaluate the factor analysis of multisystem involvement.
Study population
A total of 169 SLE patients complicated with infection (17 males, 152 females; mean age 44.80 ± 17.30 years; range 11–89 years) according to the Systemic Lupus International Collaborating Clinics/American College of Rheumatology (ACR) 2012 10 who met the inclusion and exclusion criteria were invited to participate. The detail of specific inclusion criteria are as follows: 1. Hospitalized patients with SLE complicated with infection between 2018 and 2020; 2. These patients meet the diagnostic criteria of Systemic Lupus International Collaborating Clinics/American College of Rheumatology (ACR) 2012. The exclusion criteria are as follows: 1. Complicated with other autoimmune diseases, such as Sjögren’s syndrome, rheumatoid arthritis, etc.; 2. Patients with pregnancy or tumor.
Study subjects were consecutively enrolled from those inpatients attending the Department of Rheumatology, Ningbo First hospital between January 2018 and December 2020. Most patients had received hormone or immunosuppressant treatment before being included in this study. The studies were approved by our respective local ethics committees.
Definitions
Infection: The diagnosis of infection will be based on positive pathogen detection of various samples (blood, sputum, pus and urine), clear evidence of infection (pneumonic infiltration on computed tomography [CT], or abscess evidence on ultrasound, CT or MRI), and clear clinical signs related to infection. A positive response to standard anti infective therapy is also used to support the diagnosis of infection. The strains include Candida albicans, Aspergillus, Escherichia coli, Candida glabrata, Cryptococcus, etc.
Multi-system involvement: Among them, SLE patients involving two or more systems are defined as involving multiple system involvement. SLE patients with only one system involved and without involving other organ functions were defined as non multi system involved group.
SLEDAI: The disease activity of each patient was measured by the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) standard questionnaire. 11 This questionnaire Contains some clinical and laboratory findings related to SLE disease. 12 On the basis of questionnaire, if the score is score less than 6, disease is inactive form and score is equal to or greater than six until 12 reveals the mild to moderate active form of activity. If the score exceeds 12, it is considered to be serious forms of activity. 13
Data and sample collection
The baseline demographic and clinical data were collected from hospital records and reviewed by experienced physicians. Medical records of each patient were retrospectively reviewed in order to obtain the following data: age, gender, course of disease, previous and present organ involvement. Some laboratory test results: complete blood count, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), serum C3, C4, ANA, dsDNA and procalcitonin (PCT) levels.
Statistical analysis
All data were analyzed using SPSS version 21.0 software (SPSS Inc, Chicago, IL). Mean ± standard and median (interquartile range) are presented for numeric values with normal or non‐normal distribution, respectively. Scores that had normal and abnormal distributions were compared by Student’s t-test and, respectively. The Student t test or Mann-Whitney test was calculated to analyze the differences between the 2 study groups. 14 Categorical variables were expressed as percentages and compared using x2 test or Fisher exact test as appropriate. Measures of association are expressed as odds ratios (OR) with a 95% confidence interval (95% CI). Receiver operating characteristics (ROC) curve was constructed and the area under curve (AUC) was performed to detect the best cutoff value between different clinical indexes and multisystem involvement in SLE patients complicated with infection. All tests performed were 2-tailed, with p < 0.05 considered to be statistically significant.
Results
Univariable analysis of factors associated with SLE patients complicated with infection having multi-system involvement.
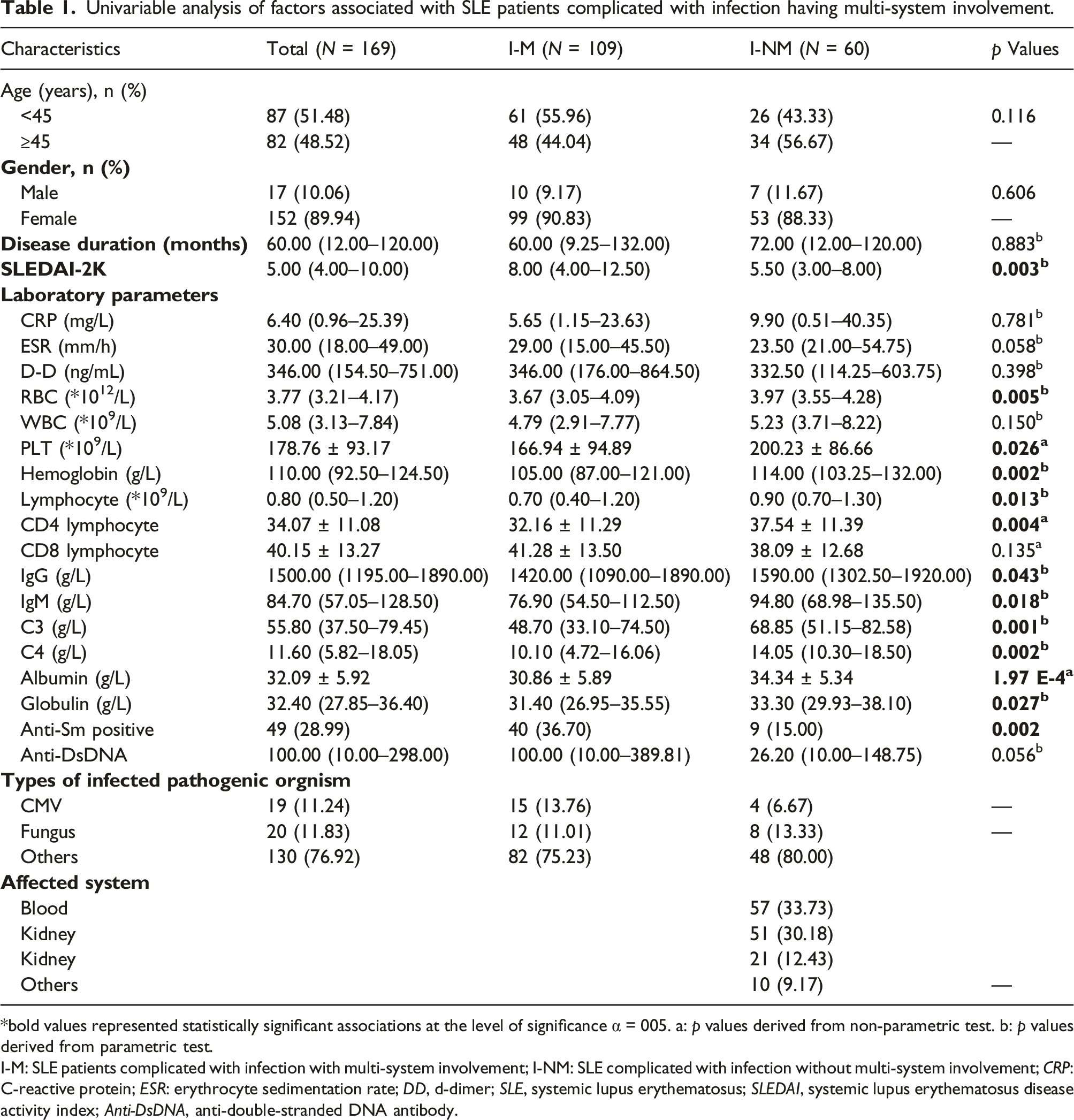
bold values represented statistically significant associations at the level of significance α = 005. a: p values derived from non-parametric test. b: p values derived from parametric test.
I-M: SLE patients complicated with infection with multi-system involvement; I-NM: SLE complicated with infection without multi-system involvement; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; DD, d-dimer; SLE, systemic lupus erythematosus; SLEDAI, systemic lupus erythematosus disease activity index; Anti-DsDNA, anti-double-stranded DNA antibody.
At the time of the study, hematological manifestations (anemia, leukopenia, thrombocytopenia, coagulopathy) were present in 33.73% of patients, renal involvement (proteinuria, renal failure) in 30.18%, lung involvement in 12.43% and others involved the liver, serosa, skin. An elevated ESR level was observed in 119 cases (119/169, 70.41%). Most of these patients had potive antinuclear antibody positive (97.63%). Anti-dsDNA antibody, anti-SSA antibody, anti-u1RNP antibody, and anti-Sm antibody was positive in 101 (59.76%), 104 (61.54%), 87 (51.48%), and 49 (28.99%) cases, respectively. Besides, we found that 117 SLE patients had used hydroxychloroquine during treatment, while 30 patients had used intravenous gamma globulin, including 9 patients with high dose (20 mg/d) and 21 patients with low dose (5 mg/d). Other demographic and laboratory data are shown in Table 1.
Univariate analysis
The SLEDAI score of SLE infected patients with multi-system involvement was 8.00, which was higher than that of patients without multi-system involvement (p = 0.003, Table 1). Similarly, the Sm positive rate was 36.70% in the group of SLE infected patients with multisystem involvement, higher than the non-multisystem involvement group (p = 0.002, Table 1). Conversely, lower RBC count (p = 0.005), platelet value (p = 0.026), hemoglobin value (p = 0.002), lymphocyte count (p = 0.004), especially CD4 lymphocytes (p = 0.004), IgG (p = 0.043), IgM (p = 0.018), C3 (p = 0.001), C4 (p = 0.002), albumin (p = 1.97E-4) and globulin count (p = 0.027) were associated with multi-system involvement.
Multivariate analysis
Multivariable analysis of factors associated with SLE patients complicated with infection having multi-system involvement.

OR: Odds Ratio; CI: Confidence interval.
CMV infection
Univariable analysis of influential factors associated with SLE patients complicated with CMV infection.

S-C: SLE patients complicated with CMV infected; S-NC: SLE patients incomplicated with CMV virus.
Fungal infection
Univariable analysis of influential factors associated with SLE patients complicated with fungal infection.

S-F: SLE patients complicated with fungal infected; S-NF: SLE patients incomplicated with fungus.
ROC curve
Results of ROC curve analysis showed that the area under the curve for differential diagnosis of detecting multi-system involvement in SLE patients with infection was 0.646, 0.627, 0.610, respectively, with the sensitivities of 73.3%, 53.3%, 73.3% for Hb, CD4, and IgM, and the specificities of 54.1%, 69.7%, 48.6%, respectively (Figure 1). The area under the curve of the combined prediction was 0.834, with a sensitivity of 78.0%, and a specificity of 76.7%, showing that the combined value was significantly higher than any of the single factors. ROC curves for (a) Hemoglobin, (b) CD4, (c) IgM, (d) Multi factor mixed model. ROC was the receiver operating characteristic curve. AUC was the area under the curve. (A): The AUC of hemoglobin count in SLE patients complicated with infection having multi-system involvement was 0.646 with a sensitivity of 73.3% and a specificity of 54.1%. (B): The AUC of CD4 lymphocyte in SLE patients complicated with infection having multi-system involvement was 0.627 with a sensitivity of 53.3% and a specificity of 69.7%. (C): The AUC of IgM in SLE patients complicated with infection having multi-system involvement was 0.610 with a sensitivity of 73.3% and a specificity of 48.6%. (D): The AUC of multi factor mixed model in SLE patients complicated with infection having multi-system involvement was 0.834 with a sensitivity of 78.0% and a specificity of 76.7%.
Discussion
According to the statistics of the national database of the United States, infection (37%) is one of the most common causes of hospitalization for SLE patients. 15 The majority of SLE patients were female, with men comprising only 10.06% of all patients. It should be noted that there was no significant difference in the mortality of male patients, while among female patients, the mortality of early and late SLE patients was much higher than that of middle-term SLE patients, showing a double peak valley structure. 16 Therefore, clinical control of patients with early infection of SLE is essentially critical for the long-term prognosis of patient.
Several previous studies have implied a potential association between SLE and infection.17,18 A large number of studies have shown that some clinical markers can be used to distinguish infection from SLE activity, such as PCT, 19 ESR/CRP ratio 20 and neutrophil-to-lymphocyte ratio. 21 This is the first study we aimed to evaluate the correlation between SLE patients complied with infection and multi-system involvement.
In this study, SLE patients complicated with infection were divided into two groups according to whether there was multisystem involvement or not. It was found that SLEDAI increased significantly in the multi system involvement group, while the counts of erythrocyte, platelet, hemoglobin, lymphocyte, IgG, IgM, C3, C4, albumin and globulin in the multi-system involvement group were significantly lower than the other group. Analysis of the reason showed that SLEDAI scoring points, which includes the changes of C3 and C4, lupus nephritis, anemia and hypoproteinemia, reflecting the disease activity of SLE patients.22,23
White blood cells are the sum of nucleated cells, including neutrophils, lymphocytes, monocytes and another karyocyte in peripheral blood. It is an essential defense line of the body against foreign body invasion including pathogenic microorganisms. 24 Clinically, various inflammatory responses and infections could modulate leukocyte levels. Lymphopenia has been shown to be associated with neurological diseases, renal involvement and vasculitis.25,26 Repeated and continuous stimulation of antigens in SLE patients could increase the expression of T cells in CD8+ and decrease the expression of T cells in CD4+. This condition in patients with SLE is more vulnerable to mitogen stimulated activated cell induced cell death and high risk of infection. 27 The changes of T lymphocytes affect IgG, resulting in tissue damage. 27 Notably, a large number of studies have confirmed that there is a correlation between lymphopenia and anti SM and low complement28,29 Over activation of complement can lead to tissue damage, and the occurrence of SLE is usually related to congenital defects in early components of the classical complement pathway. 30
The statistics of SLE inpatients in Beijing showed that CMV infection was the most common viral infection (61.1%), followed by fungal infection (29.6%). 31 This is consistent with our study (Table 1). CMV infection triggers SLE onset not only through direct cytopathic effects of viral replication in host cells, but also through inflammatory processes that can lead to systemic and organ-specific disease. 32 The research 33 showed that stimulating peripheral blood mononuclear cells of SLE patients before CMV specific antigen treatment in vitro would further significantly increase the percentage of CD4 T cells, mainly CD4+ memory T cells. In contrast, our subgroup analysis of SLE patients with CMV infection showed no significant difference in lymphocyte proportion, this could be explained by CMV infection is caused by multiple factors, which requires a larger sample size.
SLE patients complied with infection is mainly mixed infection, 34 fungal infection could exist alone or mixed with pathogens such as bacteria and viruses. 23 A study, in which 112 hospitalized SLE patients were included, showed that Candida albicans was the most common fungal species in invasive fungal infection. 23 To study this further, we divided SLE patients with or without fungal infection into two groups. The results showed that lymphocytes in the fungal infection group were lower than those in the non-fungal infection group, which is consistent with previous studies by others that SLE patients with severe lymphopenia are more prone to opportunistic infections, especially CD4+ lymphopenia. 35
Some limitations of the present study should be mentioned. One of the main limitations is that this study was conducted in inpatients in a single tertiary hospital, and our findings may not generalized to outpatients with SLE or patients in other regions. More, this is a cross-sectional study, therefore the temporal relationship between influential factors and outcome of interest is unclear. Actually, this study was performed mainly based on the medical records of the SLE patients with infection and hospitalized in Ningbo First Hospital from 2018 to 2020. Therefore, we did not estimate sample size initially. For instance, we studied the related factors of SLE patients complicated with fungal infection (Table 4), but the research usefulness of the study findings is limited due to the small sample size and low computational efficiency, which increases the probability of false negatives in the results.
Conclusions
In conclusion, our study is the first population-based cross-sectional study to explore the relationship between SLE complicated with infection and multi-system involvement in the hospitalized population. Our study emphasizes that hemoglobin number, CD4 level, IgM and SM may be independent influencing factors of multi-system involvement. However, there are significant age group differences in special pathogens infected groups, such as CMV or fungi. Abnormal immunity could easily lead to infection by opportunistic bacteria. Therefore, clinicians should be vigilant for the changes of indicators when managing patients with SLE in hospitals. Prospective studies are required to confirm the analysis of influencing factors involved in multiple systems in patients with SLE patients complicated with infection.
Supplemental Material
Supplemental Material - A cross-sectional study of systemic lupus erythematosus patients complicated with infection
Supplemental Material for A cross-sectional study of systemic lupus erythematosus patients complicated with infection by Hang Yu, Qinwen Wen, Xiaolu Zhang and Xiudi Wu in European Journal of Inflammation
Footnotes
Author’s note
All of our authors reiterate that written informed consent has been obtained from all subjects, including legally authorized representatives of minor subjects, prior to the start of the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Planned Science and Technology Project of Zhejiang Province (Grant No. 2019KY570).
Ethical approval
Ethical approval for this study was obtained from Ethics Committee of Ningbo First Hospital (2021-R090).
Informed consent
Written informed consent was obtained from all subjects before the study. All of our authors reiterate that written informed consent has been obtained from all subjects, including legally authorized representatives of minor subjects, prior to the start of the study.
Supplemental Material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.