
Abstract
Objective
To determine whether polymorphisms in IL-6 and IL-12 contribute to the etiology of coal workers’ pneumoconiosis (CWP) in a Chinese Hui population, and to evaluate the efficacy and safety of high frequency oscillatory ventilation (HFOV) in the treatment of CWP.
Introduction
Genes and the environments interplay in the development of CWP, and the association between the potential functional polymorphisms in many genes and CWP have been reported.
Methods
We genotyped the IL-6-634C/G (rs1800796) and IL-12B-1188A/C (rs3212227) polymorphisms in a case-control study including 160 CWP patients and 150 dust-exposed control subjects of Chinese Hui population, and analyzed the associations between these genetic variants and CWP risk. We also evaluated the efficacy and safety of HFOV for whole lung lavage (WLL) in the treatment of CWP.
Results
Carrying the C allele of IL-6-634C/G (rs1800796) was associated with decreased risk of CWP (p < 0.05). No significant differences in allele or genotype frequencies of IL-12B-1188A/C was found between the CWP cases and control subjects (p > 0.05). Compared with CWP patients with routine WLL, CWP patients received HFOV showed better pulmonary functions. HFOV treatment also yield a significant higher efficient rate (97.50%) than WLL treatment (81.25%, p = 0.001). CWP patients receiving HFOV and WLL treatment both showed significantly increased serum contents of Clara cell protein 16 (CC16) and superoxide dismutase (SOD), and decreased serum contents of serum malonaldehyde (MDA). While the increasing of CC16 and SOD, and decreasing of MDA in patients receiving HFOV was more noticeable than patients receiving WLL.
Conclusions
Taking together, the −634C/G polymorphisms in IL-6 play a role in the etiology of CWP. HFOV, when applied in CWP patients, significant improves their pulmonary functions.
Keywords
Introduction
Pneumoconiosis, induce by chronic exposure to airborne inorganic dusts (such as free silica dust, asbestos fibers, dust from coal mines, and mixed silicate dust), is a type of restrictive lung disease. 1 One of the most common pneumoconiosis is coal workers’ pneumoconiosis (CWP) caused by inhalation and deposition of respirable coal dust and silica in the lungs.2,3 CWP is usually categorized into two stages: simple CWP and progressive massive fibrosis (PMF) according to the severity of disease. There is acceptance of the pathophysiological mechanisms implicating chronic inflammatory processes in the development of the pulmonary lesions, most notably by formation of reactive oxygen species (ROS). Coal dust reacts with epithelial and macrophage cells, resulting in the oxidation of membrane lipids, ultimately leading to destroy of the alveolar septa. These epithelial and macrophage cells secret fibrogenic factors which could induce fibroblast proliferation or collagen synthesis, and inflammatory chemokines and cytokines production which lead to the migration of macrophages and polymorphonuclear leukocytes from the pulmonary capillaries to the air spaces. Besides, alveolar macrophages engulfed coal dust could produce ROS, which leading to lipid per oxidation and lung scarring. 4 CWP can still be diagnosed in workers who have worked in poor workplace environments two to three decades ago, even the work environments improved. On the other hand, not all coal workers have CWP despite being exposed to similar environments. These findings suggest that multiple genetic and the environmental factors may interplay in the development of CWP, and individuals may have different genetic predispositions. 5 Therefore, researches in genetic variation may help us better understanding the disease pathogenesis of CWP and provide new strategies for successful treatments regimens.
Studies have reported increased amounts of IL-6 in alveolar macrophage from patients with CWP compared to controls. Compared to simple pneumoconiosis, an increased secretion of IL-6 was observed in PMF patients, suggesting that IL-6 participated in the pathogenesis of pneumoconiotic disorders.6,7 It is important in inflammatory processes through facilitating monocytes infiltration into the lung, and in the fibrotic response through inducing collagen synthesis in vivo. 8 IL-2, mainly produced by activated macrophages, centrally involves in regulating the production of type 1 or type 2 cytokines and in determining the nature of immune responses. Elevated serum levels of IL-12-related cytokines (IL12p40 and IL-12p70) were reported in silicosis patients. Moreover, elevated IL-12p40 aggravates the formation of pulmonary fibrosis through recruiting of nuclear macrophages.9,10 Distribution of single nucleotide polymorphisms (SNPs) in the 3′UTR of IL-12B has associated with severity of silicosis, rather than susceptibility. 10 To further determine whether the IL-6-634C/G (rs1800796) and IL-12B-1188A/C (rs3212227) polymorphisms contribute to the etiology of CWP in a Chinese Hui population, as well as the associations between these genetic variants and CWP risk were genotyped and detected.
High frequency oscillatory ventilation (HFOV) is an alternative method of ventilation which achieves the goals of lung protective ventilation theoretically. 11 Early HFOV has a good performance in oxygenation improvement in the acute stage of RDS, reduces the need of surfactant administration, and decreases the injury to lung tissue even in newborns. In recent years, HFOV has been used in the treatment of burn and inhalation lung injury, and good clinical outcomes have been reported.12,13 However, the administration of HFOV in the treatment of CWP remains limited. In this study, the efficacy and safety of HFOV in the treatment of CWP were also evaluated.
Materials and Methods
Subjects
The research protocol was approved by the Ethics Committee of The Fifth People’s Hospital of Ningxia Hui Autonomous Region (No. NXDWYY2016-0012). All subjects were ethnic Hui Chinese without blood/genetic relationship, and were previously exposed to occupational silica dust from the sane mines. Informed consent was obtained from all the enrolled subjects before research. Based on the National Diagnostic Criteria for Pneumoconiosis of China (GBZ 70-2009) and 1980 International Labor Office (ILO) Classification of pneumoconiosis, high kilovolt chest X-ray and physical examinations were performed for all patients who admitted to hospital for pathologic diagnosis of CWP.
There are 160 diagnosed CWP patients and 150 dust-exposed control subjects enrolled in the current study for IL-6-634C/G (rs1800796) and IL-12B-1188A/C (rs3212227) polymorphisms analysis. The 160 CWP cases were enrolled from The Fifth People’s Hospital of Ningxia Hui Autonomous Region between May 2016 and December 2018, including 90 cases of stage I and 70 cases of stage II. Control subjects (150 subjects) were enrolled between June 2016 and November 2019 from the same department of the same hospital. The 150 control subjects had comparable dust exposure period, job types and ages with the CWP cases. Patients with autoimmune diseases, or treated with immunosuppressive or immunostimulatory drugs, or received radiotherapy or expose to asbestos were excluded from this study. The age of CWP patients was from 45 to 69 years (63.6 ± 8.1), and the age of the control subjects was from 46 to 70 years (64.6 ± 9.6). There was no significant difference in the age of the CWP case and control subjects. After informed consent form was signed by each individual participant, information on their health conditions, life style including smoking, and occupational exposure were surveyed by questionnaire. Five mL of peripheral blood were obtained from both CWP cases and matched control subjects for genomic DNA extraction.
The 160 CWP patients were scheduled for whole lung lavage, and were enrolled for further study. Conduction of the trial and whole lung lavage was approved by the Ethics Committee of The Fifth People’s Hospital of Ningxia Hui Autonomous Region. The 160 patients were randomly assigned to receive either whole lung lavage or HFOV using sealed envelopes with treatment based on random numbers. The lung function of the CWP patients before and after whole lung lavage were recorded, including forced vital capacity (FVC), conventional lung capacity (VC), forced expiratory volume in the first second (FEV1), maximal voluntary ventilation (MVV) and forced expiratory flow at 25%, 50% and 75%.
Genomic DNA isolation
Genomic DNA was extracted from 5mL of collected peripheral blood specimens using QIAamp DNA Blood Mini Kit (cat : 51104, Qiagen, German) according to the manufacturer’s instructions. The quantity of the extracted DNA was tested spectrophotometrically.
Selection of single-nucleotide polymophism (SNPs) and genotyping
In order to overall analyze the possible roles of IL-6 and IL-12B on the genetic susceptibility to CWP, one SNP (rs1800796) within the locus of IL-6 and one SNP (rs3212227) within the locus of IL-12B were selected for genotyping. SNP genotyping was identified using the polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP), followed by the Golden Gate assay on the Illumina BeadStation 500 GX (Illumina Inc., San Diego, CA) system. The primer sequences used in this study for PCR-RFLP were as follows: IL-6 5’-CAG GTG AAG AAA GTG GCA GAA-3’ (forward) and 5’- AGT GAC CAG ATT AAC AGG CTA GA-3’ (reverse), IL-12B 5’-CAC ATC AAC TTT TGG CAT TCT CTT-3’ (forward) and 5’- TCC ATA CAT CCT GGC AGA CAA-3’ (reverse). The sequencing primers were 5’- TGT ATT TGT AAA AAC CAA AG-3’ (IL-6) and 5’- GAT GAA AAT TTG GAG GAA AA-3’ (IL-12B). PCR amplification conditions were: denaturing at 94°C for 15s, annealing at 55°C for 15s, extension at 72°C for 30 s, for 35 cycles. Two μL of PCR products were used for sequencing. Genotyping was carried out by two different technicians without known of the status of the subjects. All the subjects were successfully genotyped with a 100% of reproducibility.
Anesthesia method and whole lung lavage
Thirty minutes before the surgery, patients received an intravenous injection of 1mg/kg penehyclidine hydrochloride. After entering the operating room, venous access of the patients were opened to complete the monitoring of vital signs. After standard intravenous induction of anesthesia with midazolam (Lot: 20181114, Jiangsu Nhwa Pharmaceutical Co., Ltd), fentanyl (Lot: 91A01071, Yichang Renfu pharmaceutical Co., Ltd), vecuronium (Lot: 18121921, Shanghai Hengrui Pharmaceutical Co., LTD) and propofol (Lot: 16MCO408, Fresenius Kabi Austria GmbH), double-lumen endotracheal catheter was inserted through the mouth, and the two lungs were accurately separated under bronchoscopy. After accurate separation of the two lungs, simultaneous large-volume whole lung lavage was performed.
High-frequency oscillatory ventilation (HFOV)
To facilitate left-sided whole lung lavage, the patients were maintained at supine position with a bolster placed under the right thorax to induce slight left tilt. The lavage container was hung 40cm above the midaxillary line, and the lavage solution was 0.9% sodium chloride solution at 37°C. The right lung or mild lesioned lung was first ventilated with a conventional anesthetic ventilator using synchronized intermittent mandatory ventilation. For each lavage, 1000 mL of lavage solution were used and each lung was lavaged for 8–12 times according to the turbidity degree of drainage lavage fluid. HFOV was performed after the 3rd, 6th and 9th lavage, respectively. The frequency of HFOV was 30–40 times/mins to keep the airway pressure within 25cm Hg. The lavage time was generally 25-50 min for single lung and 60-120 min for double lungs. After lavage of the first side of lung, pure oxygen pressurized ventilation was administrated and the residual fluid in the bronchial lumen was absorbed by intermittent negative pressure ventilation until no pulmonary moist rales. The contralateral lung lavage was performed when the peripheral arterial oxygen saturation was maintained above 95%.
Evaluation of clinical efficacy
The clinical efficacy of HFOV and WLL treatment was evaluated as follows: significant efficacy: residual lavage fluid volume ≤300 mL, and no complications such as cough and dyspnea; Efficacy: 300 mL < residual lavage fluid volume <600 mL, and mild cough without affecting normal life and sleep; Inefficiency: residual lavage fluid volume ≥600mL, with serious complications.
ELISA
Serum was separated from patients’ blood samples before and after HFOV or WLL treatment, and stored at −80°C. Commercially available ELISA kits (Elabscience, Wuhan, China) were used to determine the serum contents of CC16(cat: E-EL-H0744c), MDA (cat: E-BC-K025-S) and SOD (cat: E-BC-K022-M) according to the manufacturers’ instructions.
Liquid-based cytology (LBC) examination of lavage fluid
Lavage fluid of patients receiving HFOV was collected after the first lavage and after the whole lavage, respectively. 5 mL of the collected lavage fluid were centrifuged at room temperature for 5minutes at 3000 r/min. The supernatant was discarded, and the sediment was mixed using a vortex mixer for 5s. Then the centrifuge tubes containing the mixture were run on an automated ThinPrep 2000 processor (Hologic), yielding 1 liquid-based slide per patient. Modified papanicolaou staining of each slide was carried out, and diagnoses were provided by a cell tester and a physician specializing in cytological diagnosis in Department of Anesthesiology, The Fifth People’s Hospital of Ningxia Hui Autonomous Region.
Statistical analysis
The χ 2 -test (for categorical variables) or Student’s t-test (for continuous variables) were used for evaluating the differences in the distributions of demographic characteristics, selected variables, and frequencies of genotypes of IL-6 and IL-12B polymorphisms between the CWP cases and control subjects. Hardy-Weinberg equilibrium (HWE) was tested using a goodness-of-fit χ 2 -test. The associations between genotypes and CWP were estimated by computing odds ratios (ORs) and their 95% confidence intervals (CIs) from unconditional logistic regression analysis with the adjustment for possible confounders. The statistical power was calculated by GraphPad Prism version 7.0.
Results
Associations between different SNPs of IL-6/IL-12B and CWP risks
Demographic and selected variables among the CWP patients and control subjects.

Distributions of genotypes of IL-6 and IL-12B and their associations with risk of CWP.
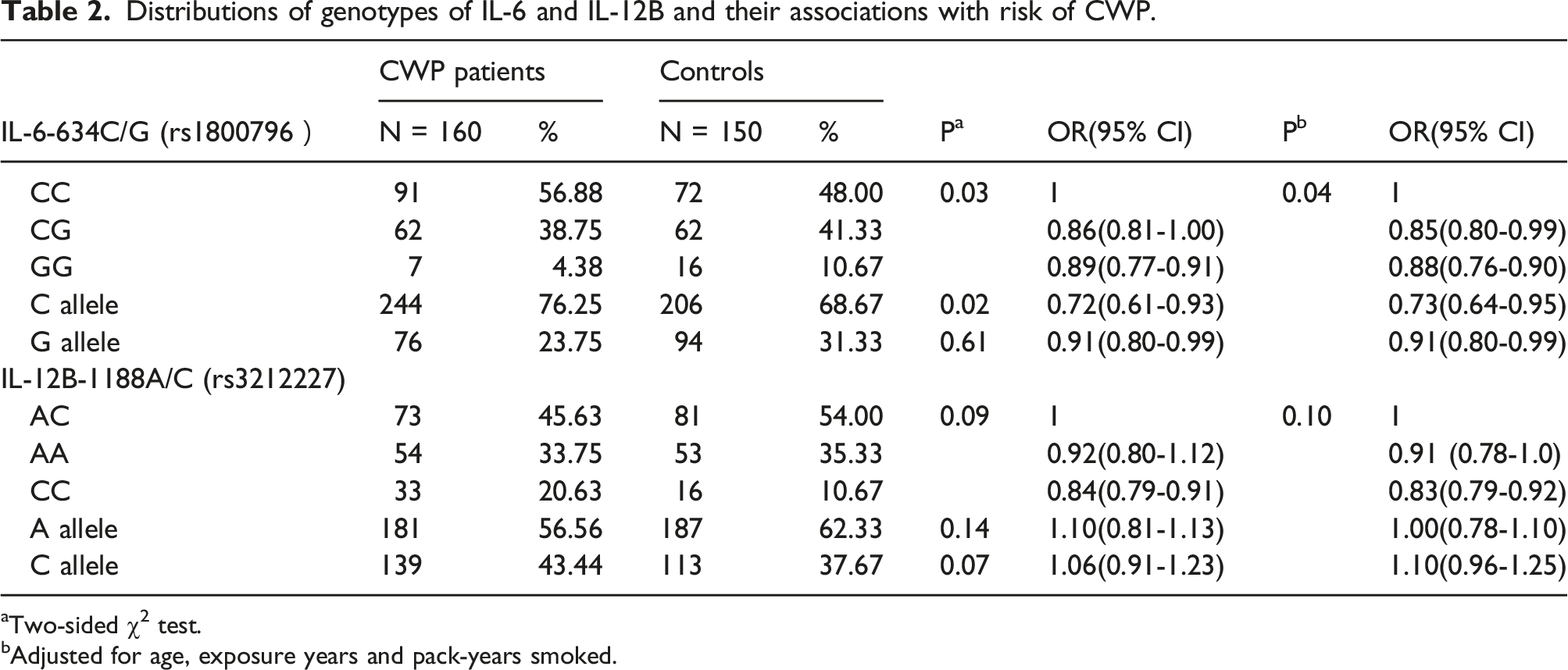
aTwo-sided χ2 test.
bAdjusted for age, exposure years and pack-years smoked.
Treatment Efficacy of HFOV and WLL treatment
Pulmonary function indexes of CWP patients received HFOV or WLL.
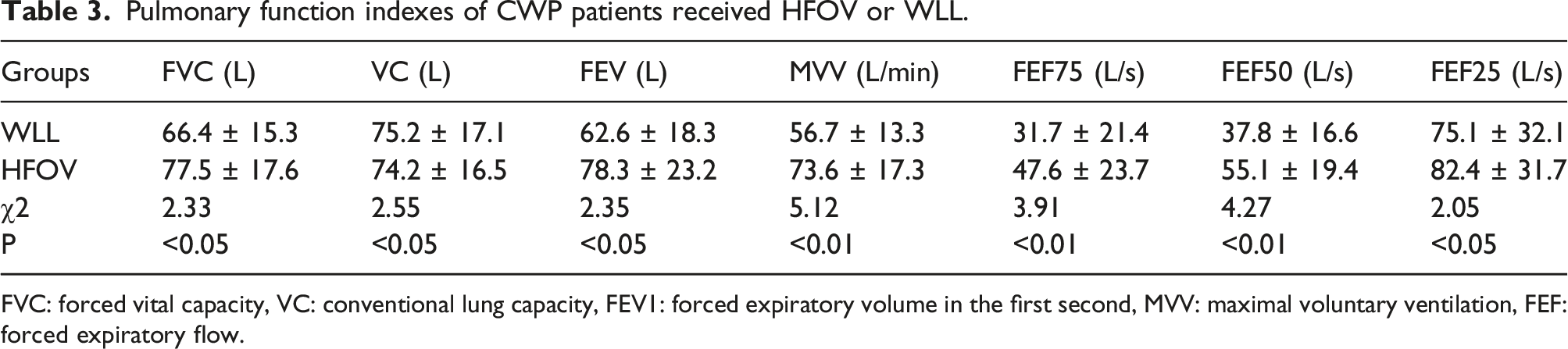
FVC: forced vital capacity, VC: conventional lung capacity, FEV1: forced expiratory volume in the first second, MVV: maximal voluntary ventilation, FEF: forced expiratory flow.
The clinical efficacy rate of HFOV or WLL.

CC16, expressed by nonciliated airway epithelial cells, is a biomarker of high interest in airway disease. It plays protective and anti-inflammatory roles by suppression of cell recruitment in upper airway inflammation. To further evaluate the efficacy of HFOV, the serum contents of CC16, MAD and SOD were determined. As shown in Figure 1, compared with patients before HFOV, significantly increased serum CC16 and SOD and significantly reduced serum MAD were observed after HFOV. Similar results were found in patients receiving WLL. Interestingly, the increasing of serum CC16 and SOD and the decreasing of serum MAD were more noticeable in patients receiving HFOV. However, there was no significant difference observed between patients receiving different treatment. Serums levels of CC16, MDA and SOD in CWP patients before and after HFOV or WLL. *p < 0.05, compared with patients before HFOV. #p < 0.05, compared with patients before WLL.
LBC examination showed that after HFOV, the numbers of macrophages engulfed coal were significantly decreased (Figure 2), further conforming the treatment efficacy of HFOV. Represented pictures of liquid-based cytology examination of lavage fluid from patients receiving HFOV. A&B: Lavage fluid of patients receiving HFOV after the first lavage (a) and after the whole lavage (b). C: The numbers of macrophages engulfed coal.
Discussion
The current case-control study demonstrated the association of two functional polymorphisms in the IL-6 and IL-12B genes with risk of CWP in a Chinese Hui population. The C allele of IL-6-634C/G was found to be significantly associated with risk of CWP. We also found that compared with routine WLL, HFOV yields a significant higher efficient rate in CWP patients.
CWP is a chronic inflammatory lung disease caused by long-term inhalation of coal dust. 4 In China, CWP accounts for over 50% of all the reported pneumoconiosis, and the incidence of CWP patients remains the highest. 14 However, not all the workers exposed to coal dust or silica develop CWP, suggesting that various environmental and genetic factors such as polymorphisms can influence the CWP phenotype and contribute to the extent or severity of CWP(1). Many gene polymorphisms have been reported to be associated with CWP in Chinese population. C-590T polymorphism in the promoter region of IL-4 is significantly associated with CWP, and the association was more evident in younger workers with a long exposure history. 15 Vitamin D receptor polymorphisms of T allele and GT or TT genotype increased the risk of CWP. 16 Many other gene polymorphisms, such as high-mobility group box 1, NAF1, CYBA and MMP1-MMP3, were reported to be associated with the susceptibility to CWP in Chinese Han population.5,17,18 In current study, we first found that the IL-6-634C/G polymorphism is associated with the risk of CWP in a Chinese Hui population. IL-6-634C/G is one of the two polymorphisms that were reported to be associated with IL-6 production, and the other one is −174 G/C. Studies have shown that alveolar macrophages and blood monocytes from patients with CWP secret higher levels of TNF-α and IL-6. Compared with control subjects, serum IL-6 level in CWP patients was higher, while soluble IL-6 receptor level showed no obvious change. 19 IL-6-634C/G polymorphism in CWP patients may be associated with changed levels of serum IL-6, which is an important indicator of the immune functions of CWP patients. The detection of IL-6 polymorphisms, as well as the level of IL-6 may provide guidelines for the selections of treatment for different CWP patients.
We also summarized the experience with HFOV and routine WLL in CWP treatment. Whole lung lavage is an efficient and safe technique which protects and maintains pulmonary function and delays the progression of pneumoconiosis lesions. 20 However, due to long lavage time and large volume of lavage fluid, a large amount of fluid remains in the lung after whole lung lavage. Residual lavage fluid is likely to damage lung and induce multiple complications, thus affecting the outcome of lavage. 21 Strategies have been described for reducing residual lavage fluid after whole lung lavage, including manual ventilation of partially fluid-filled lungs and intermittent ventilation of both lungs. In this study, we compared the outcome of HFOV and WLL. HFOV is a form of high-frequency ventilation that delivers very small subtidal volumes at high frequencies. 12 It has two unique features: the presence of a gas-driven piston which acts as both an inspiratory and expiratory valve and the passive exhalation of subtidal volumes. It has been reported that HFOV improves clearance of airway debris and secretion. 22 We found that HFOV therapy significantly improved pulmonary function, with fewer complications. As an effective lavage method, more rigorous clinical trials are needed to support the use of HFOV therapy in patients with CWP.
Conclusion
Our study demonstrated that the functional IL-6-634C/G polymorphism is associated with CWP risk in a Chinese Hui population. And HFOV therapy significantly improved pulmonary function of CWP, with fewer complications. Several limitations should be addressed. First, although this case control study was adjusted for age, gender, exposure years, tobacco consumption and others factors, other potential biases such as lacking information and confusion bias could have affected the outcomes. Secondly, all the participants were from Ningxia Hui Autonomous Region, and the sample size was only moderate. Thus, power analysis and sample size calculation was not done before the project due to limited sample size. Further studies are needed to endorse our conclusion in larger Hui population from all over China.
Footnotes
Authors’ contributions
X XD and L MZ designed experiments and wrote the manuscript; X XD and Y J collected the blood samples; Z JL communicated with the patients and collected the signed informed consent form; carried out experiments; X XD and X SL performed PCR-RFLP; Y YW analyzed PCR-RFLP results; H XY isolated genomic DNA; X XD, Y YS and L RR performed HFOV and WLL.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by Key Research and Development Projects of Ningxia Hui Autonomous Region (No. 2018BEG03059). The funding source had no involvement in the study design, the collection, analysis and interpretation of the data, the writing of the report or decision to submit this paper for publication.
Ethical approval
All experimental protocols were approved by the Ethics Committee of The Fifth People’s Hospital of Ningxia Hui Autonomous Region (No. NXDWYY2016-0012).