
Abstract
Whether serum proprotein convertase subtilisin/kexin type 9 (PCSK9) affects the prognosis of patients after the percutaneous coronary intervention (PCI) in hypertension patients remains unknown. A total of 2350 acute myocardial infarction (AMI) subjects with hypertension after PCI were enrolled. Subjects were under 30-months follow-up and divided into the major cardiovascular adverse event (MACE) Group and the non-MACE Group. Cox regression analysis were performed for the risk factors of occurrence of MACE. The relationship between the level of PCSK9 and Gensin score was analyzed by Pearson correlation. Two hundred and thirty-two patients were divided to the MACE Group. Age over 55 (hazard ratio (HR) = 2.52; p = 0.032), smoking (HR = 1.02; p < 0.001), diabetes mellitus (HR = 1.35; p < 0.001) and PCSK9 levels over 1011.3 ng/mL (HR = 1.05; ptdf < 0.001) were risk factors of occurrence of MACE. Baseline levels of PCSK9 was significantly related with Gensini score in ST segment elevation myocardial infarction (STEMI) patients (r = 0.51), all patients (r = 0.37) and non-STEMI patients (r = 0.34, p < 0.001). A high baseline PCSK9 level was the risk factor of poor prognosis of AMI patients with hypertension after PCI. PCSK9 levels were associated with the Gensini score in STEMI patients.
Trial registration: This trial was registered at clinicaltrials.gov as NCT04100434.
Keywords
Introduction
Atherosclerotic cardiovascular disease (ASCVD) is one of the most important risk factors for mortality among patients with hypertension. 1 Among the different types of dyslipidemia, a high level of low-density lipoprotein cholesterol (LDL-C) was associated with actual atherogenic burden in ASCVD patients.2,3 For patients at very-high ASCVD risk, the 2019 ESC/EAS Guidelines for the management of dyslipidemias recommended a very strict LDL-C concentration, <55 mg/dL. 4 A meta-analysis of 3,12,175 patients demonstrated that with 1 mmol/L LDL-C reduction in statin therapy the risk of major adverse cardiac events (MACE) risk reduction reduced by 23%. 5 However, according to the clinical studies and meta-analysis,6–8 it seems that statins’ effect has a “ceiling effect” on the reduction of LDL-C, that the highest dose of any statin cannot reduce the baseline LDL-C level by more than 55–60%. It is not enough for patients with high or very-high ASCVD risk.
The human proprotein convertase subtilisin/kexin type 9 (PCSK9) gene is 22-kb in length, located at 1p32.3, comprising 12 exons and 11 introns encoding a 692 amino acid protein, proprotein convertase subtilisin/kexin type 9 (pre-PCSK9). PCSK9 had been identified as the third pathogenic gene associated with familial hypercholesterolemia in 2003. Genome-wide association studies (GWASs) showed that PCSK9 polymorphisms were significantly correlated with the severity of coronary artery disease (CAD). 9 PCSK9, produced mainly in the liver, plays an important role in various vascular diseases and CAD due to elevated LDL receptor (LDL-R)-dependent LDL-C levels. It had been proved that plasma PCSK9 levels were transiently upregulated in the rat acute myocardial infarction (AMI) surgical model. 10 In humans, serum PCSK9 levels are linearly associated with fractions in CAD. 11 More recently, the monoclonal antibodies of PCSK9 were recommended by the Guidelines for the additional 15% ASCVD risk reduction with 60% LDL-C decrease from baseline, in the background of statin therapy.12,13
However, whether serum PCSK9 levels will affect the prognosis of patients after the percutaneous coronary intervention (PCI) remains unknown. In this study, we find the relationship between baseline PCSK9 levels and the severity of coronary lesions as well as the prognosis of PCI in a group of hypertension patients who were first diagnosed with AMI.
Method
Study design and sample size
This was a cross-sectional, multiple-center study in hypertension patients after PCI. The minimum sample size was calculated before the study was performed by software G power (3.1.9; Franz Faul, University Kiel, Germany). The degree of assurance 1-β was 0.95, and test level α was set to 0.05, So the minimum number of samples was 396 subjects. This study protocol was obtained permission from the Ethics Committee of our hospital and all participants signed written informed consent.
Subjects
The subject inclusion criteria were as follows: 1. Patients with hypertension; 2. Diagnosed with AMI for the first time and conducted PCI with at least 1 stent between Jun 2017 and Jun 2018; Exclusion criteria included: 1. Previous diagnosed CAD; 2. Under any lipid-lowering therapies; 3. Left ventricular ejection fraction ≤30%; 4. Patients with any tumors or systemic diseases; 5. Glomerular filtration rate <60 mL/min/1.73 m2); 6. Childbearing-age women or pregnant women.
Patients with any MACE (all-cause death, reinfarction, stroke, new congestive heart failure, and recurrence of stable or unstable angina or a nonfatal arrhythmia) during follow-up up were divided into the MACE Group, with no MACE were divided into the non-MACE Group (Figure 1). The clinical data including demography characteristics, PCI history, and peri-PCI therapy regimens were collected from the electronic medical record system. The C-reactive protein (C-RP), blood lipids level, troponin I (cTnI), N-terminal pro-brain natriuretic peptide (NT-Pro-BNP), and the PCSK9 level were obtained from the clinical standardization laboratory. Cox regression analyses were conducted for the risk factors of MACE. We also performed Pearson correlations to assess the relationship between the PCSK9 level and Gensini score and compared the occurrence of MACE between different baseline PCSK9 intervals. Flow chart of this study.
PCI Procedure and Follow Up
ST-segment elevation myocardial infarction (STEMI), and non-ST-segment elevation myocardial infarction (NSTEMI) were diagnosed according to the Fourth universal definition of myocardial infarction. 14 All coronary angiographies (CAGs) and PCIs were performed in a standardized procedure and the physicians determined whether thrombus aspiration and intravascular examination should be given, the location, and the number of stents. The length and diameter of the stents used, pre-dilation of the target lesion, and post-dilation of the stent were also at the discretion of the operator. Perioperative and 1-year postoperative treatment of PCI was given according to guideline. 15
All patients enrolled in this study were under 30 months of follow-up in the clinic or with telephone interviews using pre-coded questionnaires, first, third, sixth month after discharge and every 6 months thereafter. Clinical events that occurred or were hospitalized during the follow-up were monitored and obtained from relevant medical records. The primary clinical endpoint was the occurrence of any MACE. Reinfarction, which included the target lesion as well as the non-target lesion in the first AMI, was confirmed with CAG. Stroke was diagnosed based on the 2016 AHA/ASA Guideline. 16 Congestive heart failure came from clinical and inpatient medical records based on Echocardiography and NT-Pro-BNP. Nonfatal arrhythmia was obtained from electrocardiographic examination (ECG) examination.
Coronary atherosclerosis lesion
The Gensini score system, based on the results of CAG, was used to evaluate the extent of coronary atherosclerosis lesion. 17 The Gensini score was used to quantitative the extent of the coronary lesions by three main parameters for each coronary artery lesion: severity score, region multiplying factor, and collateral adjustment factor.
Lipoprotein a (Lp[a]), PCSK9 measurements
Blood samples (5 mL) were obtained from all recruited patients before CAG. All blood samples were centrifugated (3000 r/min, 10 min) and then stored at −80°C until analysis Tina-quant Lipoprotein (a) Gen.2 system (Cobas Integra 400/800, Roche Diagnostics, Mannheim, Germany) was used to measure the level of Lp(a) by particle-enhanced turbidimetric immunoassay. The plasma PCSK9 levels (1:100 prediluted) were measured with the qualitative ELISA kits (ab215081, Abcam Corporation, UK). Quality control of the ELISA test was performed according to the instruction manual. Sample concentrations were got by generating a four-parameter logistic curve-fit. The intraassay coefficient of variation (CV) was 3.96 ± 0.83%. The interassay CV was 6.32 ± 1.17%. The sensitivity detectable concentration was 37.07 pg/mL, and calibration ranged from 250 pg/mL up to 16,000 pg/mL.
Statistical analysis
Quantitative variables were presented as mean ± standard deviation and qualitative variables were summarized with numbers (percentages). Students t-test, Pearson chi-square was used to evaluate differences between groups. The Kaplan-Meier (K-M) method and the log-rank test were performed to test the differences between MACE-free survival. Cox proportional hazard models were used to explore the risk factors of MACE in hypertension patients after PCI. Pearson correlations were conducted to determine the relation between PCSK9 levels and Gensini score within STEMI and NSTEMI patients. Statistical analysis of data obtained using STATA version 15.0 for Windows (StataCorp, College Station, Texas). p-value < 0.05 was considered to be statistically significant
Results
Main outcomes
Comparison of baseline clinical demography characteristics, lipids, PCSK9, and biological indexes.

aOverweight was defined as body mass index (BMI) > 28 (BMI = weight (kg)/height (m)2).
bFamily history was defined as the age of onset of coronary heart disease less than 55 for men and less than 65 for women, in the immediate family members of patients.
TC: total cholesterol; TG: triglyceride; LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein cholesterol; non-HDL-C: none high-density lipoprotein cholesterol; ApoA1: apolipoprotein A1; ApoB: apolipoprotein B; Lp(a): lipoprotein a; cTnI: troponin I; NT-Pro-BNP: N-terminal pro-brain natriuretic peptide; C-RP: C-reactive protein; PCSK9: proprotein convertase subtilisin kexin 9.
TG, HDL-C, ApoB, Lp(a), NT-Pro-BNP, C-RP, and PCSK9 were skew distribution and shown as median (25th percentile, 75th percentile). Before the Student’s t-test for the difference between groups, the nonnormal distribution variables were converted into natural logarithm form.

Kaplan-Meier survival curves for the major advanced cardiovascular events. PCSK9 intervals were divided into three equal parts, low, medium, and high, according to the baseline PCSK9 concentration. Bars and numbers above the follow-up time point showed the number of MACE in each PCSK9 group. P1, the statistical probability of the comparison between PCSK9-high group and PCSK9-low group; P2, the statistical probability of the comparison between PCSK9-high group and PCSK9-Medium group; *p < 0.05.
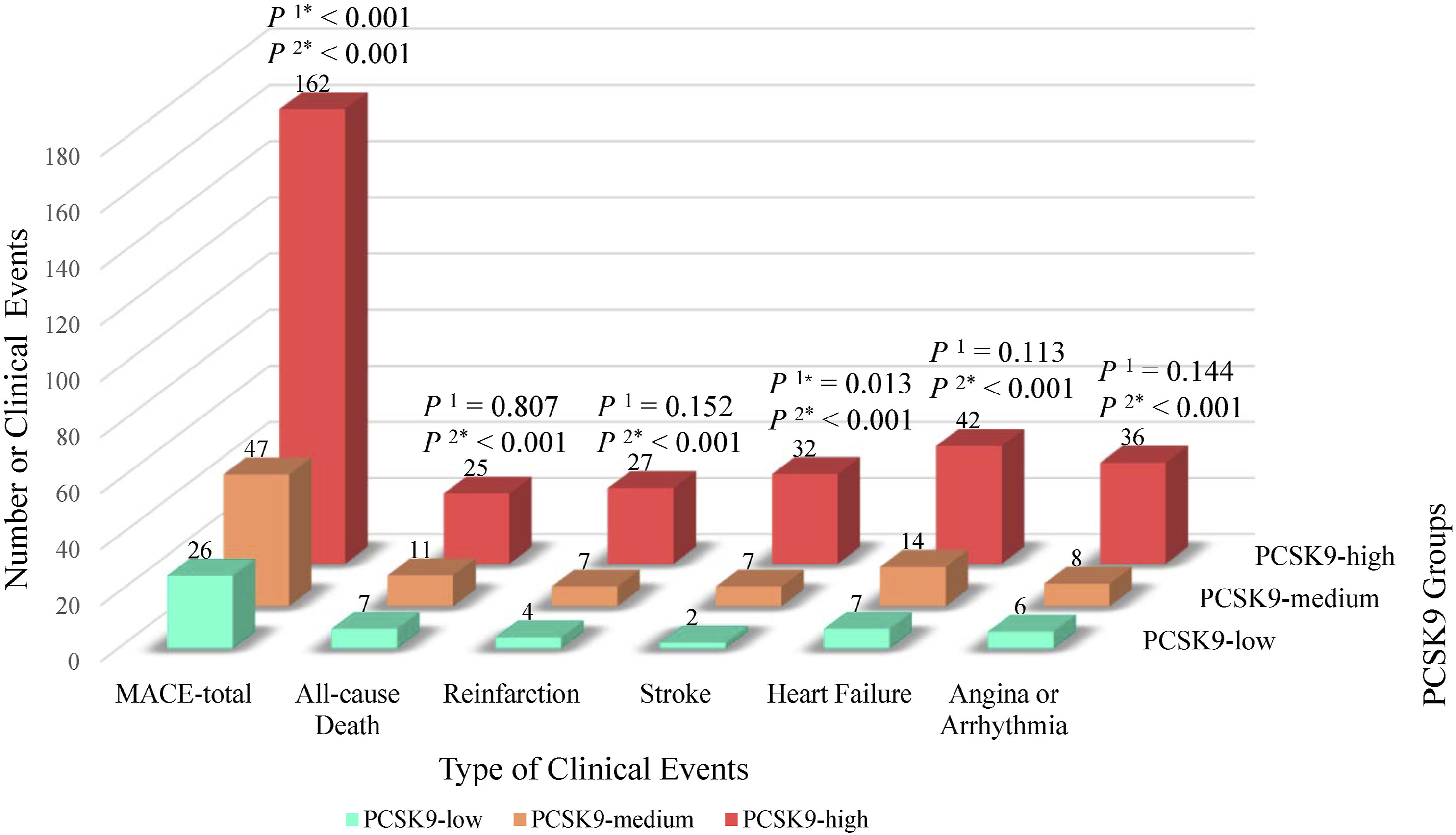
Major advance cardiovascular events comparison between PCSK9 Groups. PCSK9 intervals were divided into three equal parts, low, medium, and high, according to the baseline PCSK9 concentration. P1, the statistical probability of the comparison between PCSK9-high group and PCSK9-low group; P2, the statistical probability of the comparison between PCSK9-high group and PCSK9-Medium group; *p < 0.05.
Baseline characteristics of the MACE group and non-MACE group
Comparison of diagnosis and treatments Peri-PCI.

STEMI: ST-segment elevation myocardial infarction; NSTEMI: non-ST-segment elevation myocardial infarction; LM: left main coronary artery; LAD: left anterior descent coronary artery; LCX: left circumflex coronary artery; RCA: right coronary artery; OAC: oral anticoagulants; β-Blocker: β receptor inhibitors, ACEI/ARB: angiotensin-converting enzyme inhibitors/angiotensin II receptor antagonist; PPI: proton pump inhibitors.
In the comparison of PPCI-related treat characteristics, the proportion of diagnosis of STEMI (p < 0.001), stents in the left anterior descent coronary artery (LAD) (p < 0.001), and clopidogrel treatment were significantly higher in the MACE Group. Meanwhile, the non-MACE Group had a higher proportion of stents in the left circumflex coronary artery and the right coronary artery (p < 0.001) and treatments of ticagrelor or beta-blocker (p < 0.001).
Risk factors for MACE during follow-up in this study
Before multivariate Cox regression analysis performed, the cutoff of age (<55 vs ≥55 years), non-HDL-C, and apoB were given according to 2019 ESC/EAS Guidelines for the management of dyslipidemias.
4
And the PCSK9’s cutoff was the median level of all patients. Meanwhile, the cutoff of NT-Pro-BNP was given by the laboratory, considering the patients’ age. The Cox regression reveals that age over 55 (hazard ratio (HR) = 2.52; 95% confident interval (95% CI): 1.08–5.86; p = 0.032), smoking (HR = 1.02; 95% CI: 1.01–1.03; p < 0.001), diabetes mellitus (HR = 1.35; 95% CI: 1.15–1.59; p < 0.001) and the level of PCSK9 over 1011.3 ng/mL (HR = 1.05; 95% CI: 1.03–1.06; p < 0.001) were risk factors of MACE (Figure 4). Forest plot of the baseline characteristics risk factors of major advance cardiovascular events.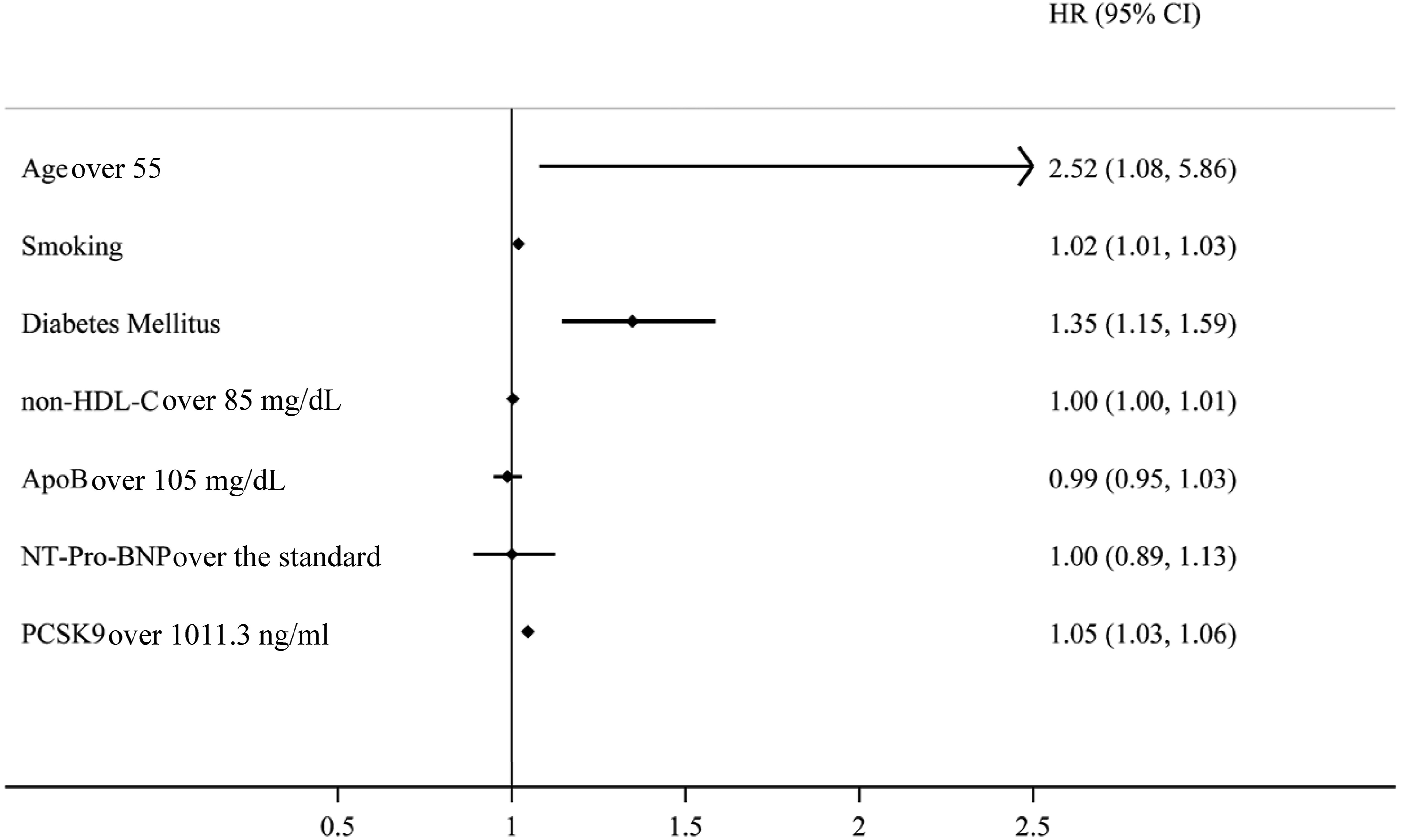
In the Cox regression of PCI-related treatments, the diagnosis of STEMI and stents in the LAD were independent risk factors related to MACE during follow-up in this study, while the use of ticagrelor was the protective factor against MACE.
PCSK9-gensini correlation analysis
Figure 5 showed the positive correlation between baseline PCSK9 levels and Gensini score (p < 0.001) The significant correlations ranked as in STEMI patients (r = 0.51), in all patients (r = 0.37) and in NSTEMI patients (r = 0.34). Pearson correlation plot between PCSK9 and Gensini Score. The Pearson correlation efficient r of PCSK9 levels and Gensini score were 0.37 for all patients, 0.51 for STEMI patients, and 0.34 for NSTEMI patients (p < 0.001).
Discussion
In the present study, we analyzed the relation between the baseline levels of PCSK9 and the prognosis of the AMI in patients with hypertension after PCI in a large sample size cohort. Because our hospital is a top hospital in our region, the present work has the largest sample size as far as we know. Our data confirmed that the baseline PCSK9 levels were not only the risk factor of the long-term poor prognosis in patients with hypertension after PCI but also positively correlated with the severity of the coronary lesion.
The main source of PCSK9 in the blood is produced by the liver. At the same time, PCSK9 is the main regulator of the level of low-density lipoprotein receptor (LDLR) on the surface of hepatocytes, which can inhibit the LDLR circulation pathway. 18 More recently, studies support the role of PCSK9 in eliciting pro-inflammatory effects on macrophages.19,20 These pieces of evidence suggest that elevated levels of PCSK9 may lead to severe coronary artery lesions and poor prognosis after PCI treatment. After PCSK9 the binding of LDL to the LDLR, both are transported into the endosome in which LDL is degraded to cholesterol and amino acids while LDLR returns to the cell surface. LDLR will be recycled about 150 times physiologically, but this cycle path could be blocked by PCSK9. The expression of PCSK9 is mainly regulated via the cholesterolemia pathway through sterol-regulatory element-binding protein (SREBP)-2. SREBP-2 is a membrane transcription factor upregulating PCSK9 expression.
Statins and other lipid-lowering drugs can reduce intracellular cholesterol biosynthesis and up-regulate PCSK9 throughout the recruitment of SREBP. 21 Besides, dietary saturated fatty acids, glucagon, and insulin also would regulate PCSK9 expression.22–24 Therefore, to avoid the effect of statins and other drugs, the patients enrolled in this study were under no lipid-lowering therapies and the blood samples were taken in a fasting state. To ensure the baseline PCSK9 levels were under minimal interference.
Besides the discrepancy of total occurrence of MACE between PCSK9 intervals, we also found that the higher baseline level of PCSK9 was associated with a higher incidence of death, reinfarction, stroke, angina, and arrhythmia, although not statistically significant. This finding was in line with the results of ATHEROREMO‐IVUS, 11 PCSK9‐REACT, 25 and the recent results reported by Minana. 26 And the research results of studies on PCSK9 inhibitors can also confirm our research results.12,13
Another clinical impact of the baseline level of PCSK9 we found in the present study is that PCSK9 levels were associated with Gensini score and a strong positive correlation was found in STEMI patients. The reason for this correlation may be the LDL-R related LDL-C up-regulation and the pleiotropy of PCSK9 including promoting endothelial apoptosis, 27 stimulating inflammatory cells to secrete pro-inflammatory factors, 28 raising the expression of scavenger receptors on monocytes and macrophages, 27 and inducing monocyte migration. 27 A recently published study reported that PCSK9 inhibitor can reduce attenuates cardiac arrhythmia, infarct size, and improve cardiac function in rats model of ischemia/reperfusion injury. 29 Nevertheless, the role of PCSK9 in the pathogenesis of STEMI and NSTEMI remains unclear.
The average age of subjects included was younger. This may be due to the subjects included in the present study being under no lipid-lowering therapies with the first diagnosed with AMI, and, which differs from the general population. On the other hand, the incidence rate of AMI in young is increasing year by year. Due to changes in lifestyle, diet structure and environmental stress, the incidence of smoking, obesity, and hyperlipidemia in people increased gradually, resulting in a significant increase in morbidity and mortality of AMI, and the trend of younger-onset is becoming increasingly evident. 30
The certain limitations of our study mainly include the following: (1) Some of the results of our follow-up were based on a telephone interview. This can introduce a criterion bias, especially in death, angina, and other clinical events. (2) As PCI is a complex and variable procedure, we can’t include all the variables in this study. Due to the difference between doctors’ working experience and technology, the comprehensive of CAD and PCI cannot be unified. (3) Although we have strict restrictions on the inclusion criteria of patients, the baseline level of PCSK9 still cannot reflect the normal level, as it is also affected by inflammation, physical activity, stress state, etc. (4) Due to the difference between the ELISA kit we used, patients have a higher average PCSK9 concentration compared with that reported previously. Additionally, we did not add PCSK9 inhibitor to the treatments after PCI. That makes it impossible to determine the causal relationship between PCSK9 levels and poor prognosis after PCI.
Conclusion
In this study, we found high baseline PCSK9 levels were the risk factor of poor prognosis of AMI patients with hypertension after PCI, and the PCSK9 levels were associated with Gensini score, especially in STEMI patients. The subgroup analysis showed the patients with the highest tri-sector of PCSK9 level had the highest occurrence of MACE.
Footnotes
Authors' contributions
All authors contributed significantly to this study. X-QW, L-XW, and BG designed the trial. X-QW, KH, JL, L-XW, and BG have conducted the work and are involved in data collection. X-QW, JL, L-XW, and BG analyzed the data. X-QW, KH, and BG interpreted the data. X-QW and KH wrote the manuscript. All authors revised the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The study was obtained permission from the Ethics Committee (Ethics approval number: 2017-0071).
Informed consent
The study conducted with the signed consent of all participants before the start.