
Abstract
Objectives:
Atrial fibrillation (AF) is a common arrhythmia in clinics with a high mortality rate. Recently, statins combined with amiodarone and amiodarone alone were used in the treatment of AF. This systematic review study aims to investigate the clinical efficacy and usefulness of statins combined with amiodarone and amiodarone alone in treating AF.
Methods:
Pubmed, Embase, Web of Science, Medline, Cochrane Library, and China National Knowledge Infrastructure were used to search for the relevant studies and full-text articles involved in evaluating statin-amiodarone versus amiodarone alone for AF. All included articles were quality assessed, and the data analysis was conducted with Review Manager 5.4.
Results:
Eight (8) relevant studies with 758 AF patients were included in this analysis. In the Meta-analysis, Statin-amiodarone treatment reduced AF recurrence (RR, 0.61; 95% CI, 0.50–0.75; p < 0.00001), C-reactive protein (CRP) level (MD, 0.96; 95%CI, 0.64–1.29, p < 0.00001) and Left atrial diameter (LAD) (MD, 0.81; 95%CI, 0.06–1.56; p = 0.03) compared with amiodarone alone for AF. However, no difference was observed for change of total cholesterol (TC) (MD, 1.32; 95%CI, −0.24–2.88; p = 0.10).
Conclusion:
Statin-amiodarone effectively reduced CRP level, LAD and reduced the recurrence of AF than amiodarone alone.
Introduction
Atrial fibrillation (AF) is one of the most common arrhythmias in clinical practice, which is associated with high morbidity and mortality. 1 Framingham’s study showed that the mortality of patients with AF is about twice that of healthy people. 2 Thrombotic events and heart failure are the main hazards of AF.3,4 The annual incidence of Embolism Events in patients with non-valvular AF is 2–7 times that in patients with non-AF, accounting for most cerebral embolism events. 5 In addition, new-onset heart failure is associated with high mortality in patients with AF. 6
At present, the primary treatment strategy of AF is to restore and maintain sinus rhythm, control ventricular rate and prevent thrombus.7,8 Although there are various clinical interventional treatment methods, drug treatment is still necessary.9–11 Amiodarone is the first-line drug for maintaining sinus rhythm after cardioversion of chronic AF.12,13 Studies show that the 1-year effective rate of amiodarone in maintaining sinus rhythm is 40%–60%. 14
Recent studies have shown that the occurrence and maintenance of AF are closely related to the inflammatory response.15,16 Inflammation can cause atrial myocyte degeneration, fibrosis, necrosis, and apoptosis, conducive to atrial folding. Statins are HMG CoA reductase inhibitors. They have not only lipid-lowering effects but also have many functions. Recent studies showed that statins also have antiarrhythmic effects.17,18 Statins have been used to treat AF, and its prevention rate is 35% higher (95% confident interval: 0.55–0.77, p<0.0001) compared with non-statins drugs.19,20
There are comparative studies on the efficacy of statins combined with amiodarone and amiodarone alone in treating AF, 21 but due to the small sample size and lack of systematic evaluation of the quality of the trial, the results are not conclusive. We conducted a meta-analysis of randomized controlled trials (RCT) to evaluate the efficacy and usefulness of statin-amiodarone versus amiodarone alone in the treatment of AF.
Methods
Literature search strategy
A systematic search in PubMed, Embase, Web of Science, Medline, Cochrane Library, and China National Knowledge Infrastructure was performed up to May 2021, with the following keywords: (1) statin; (2) amiodarone; (3) atrial fibrillation. Combinations of keywords using Boolean operators were adopted for search strategy. We performed a comprehensive search to identify all relevant studies regardless of language or publication status (published, unpublished, in the press, and ongoing). Additionally, we manually searched the references of the selected articles, relevant reviews, and previous meta-analyses for potentially appropriate citations.
Study selection
After the initial selection of relevant studies, we reviewed the potential relevance in the text and included those studies that are satisfied the following inclusion requirements. The inclusion criteria were RCTs statin-amiodarone with versus amiodarone alone; Patients with AF; containing indicators evaluating effectiveness; the study was a randomized controlled design, and the use of statin-amiodarone and amiodarone in the two groups could be similar and comparable.
Duplicates or reviews or letters or case reports or comments or editorials; simple description without comparison; absence of key information; and study lacking available data were excluded.
Data extraction and quality assessment
Two reviewers overviewed all titles and abstracts of the relevant manuscripts and independently extracted the data. We extracted the data in the prespecified excel forms, including first author name, publication year, treatment, number of patients (test group and control group), sex, age, follow-up (months), and primary outcome. We summarized data on endpoints from each trial, including the rate of AF recurrence, change of C-reactive protein (CRP) level, change of total cholesterol (TC), and change of Left atrial diameter (LAD). The methodological quality of included studies was evaluated using a modified version of the Cochrane Risk of Bias Tool.
Statistical analysis
Statistical calculations were performed using RevMan, version 5.4 (The Cochrane Collaboration, Oxford, UK) and STATA 14.0 (STATA Corp., College Station, TX, USA). We calculated risk ratio (RR), mean difference (MD), and 95% confidence intervals (CIs) for outcomes. A generalized Cochran’s Q statistic was used to assess the heterogeneity of the multivariate meta-analysis. A fixed or random-effect model was used depending on the absence or presence of significant heterogeneity. Sensitivity analysis was conducted by deleting a single study each time to observe the influence of the individual outcome on the overall analysis. To address publication bias, we used the funnel plots. 20 If any bias was observed, further bias quantification was measured using the Egger test.
Results
Literature search process
Initially, 535 articles were considered for our study. After duplicate elimination (n = 37), 413 studies were excluded by the careful screening of the titles and abstracts due to not fulfilling the present meta-analysis’s inclusion criteria. 65 Full Texts were assessed. Finally, eight (8) articles fulfilled the inclusion requirements and were included in our meta-analysis.21–28 Figure 1 illustrated the search process, with the associated inclusion and exclusion criteria.

Flowchart of literature search.
Study inclusion characteristics
Studies comprised of 8 RCTs involving 758 patients were available for the meta-analysis, of which 332 received statin-amiodarone treatment (test group) and 426 received amiodarone treatment alone (control group). The follow-up duration extended from 3 months to 12 months. All these studies were published from 2008 to 2021. The mean age ranged from 43 to 65 years (test group) and 44 to 65 years (control group). The percentage of females ranged from 31-54% (test group) and 28 to 56% (control group). Among the selected studies, the patient’s numbers were quite variables. The selected studies' criteria are summarized in Table 1.
Basic characteristics of included studies in the systematic review.

. 1, rate of AF recurrence; 2, change of C-reactive protein level; 3, change of Left atrial diameter; 4, change of total cholesterol.
Results of the quality assessment
The Cochrane bias risk assessment tool was used to assess the selection, performance, detection, attrition, and reporting bias among the considered trials (Figures 2 and 3). 29 One attrition bias and another reporting bias were detected by one study (Figure 2). Considering the bias sum-up, there were few selection, performance, and detection biases. However, only two trials were at risk of bias, and the remaining six trials identified no risk.
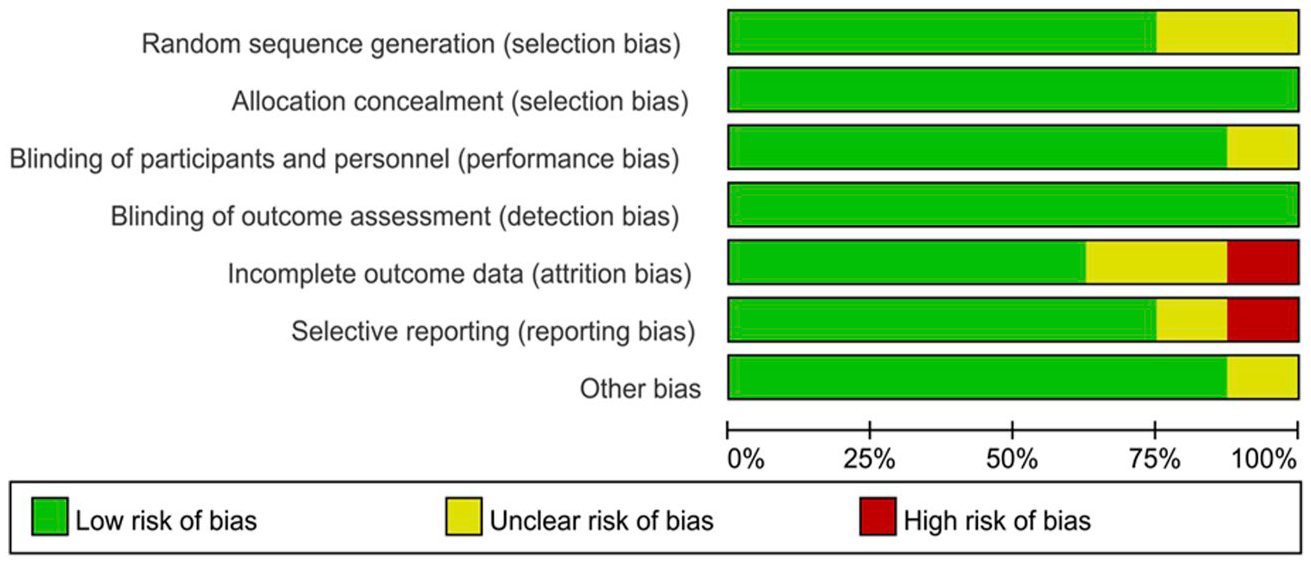
Quality assessment of the studies in this meta-analysis high, low, and unclear risk of bias were marked in red, green, and yellow.

Risk of bias summary of the studies included.
Results of heterogeneity test
Eight studies with 758 patients reported the rate of AF recurrence. Overall, the pooled estimate showed that compared to control group, test group can significantly reduce the rate of AF recurrence (RR 0.61, 95%CI [0.50, 0.75]; p < 0.00001), without significant heterogeneity among the included studies (I 2 = 0%, p = 0.81) (Figure 4).
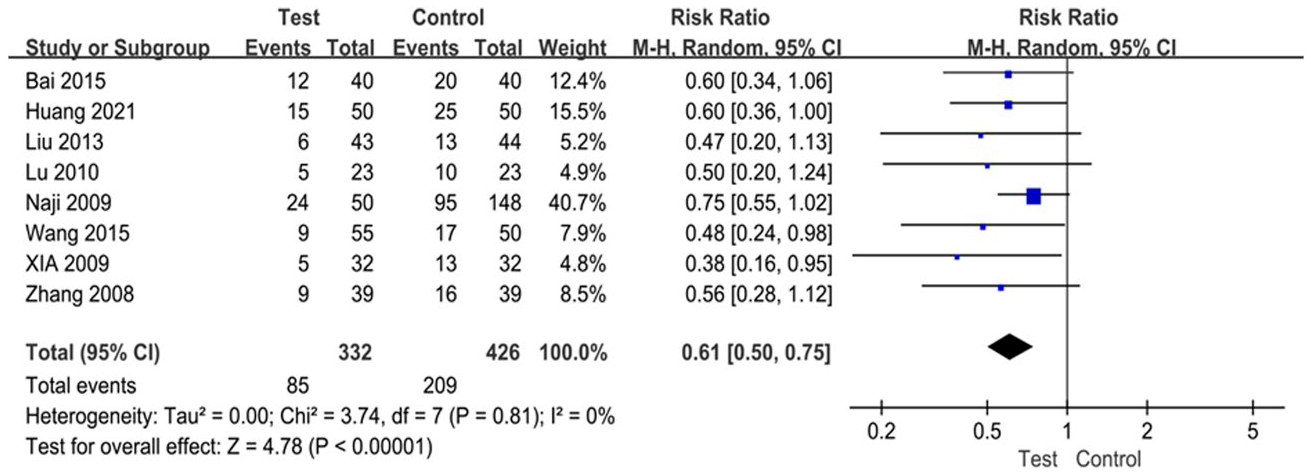
Forest plot showing the risk ratio of rate of AF recurrence.
In the evaluation of the difference in CRP change between the test group and control group, five articles involved 396 patients were included. Meta-analysis showed that compared to control group, test group had a higher reduction of CRP level (MD: 0.96, 95%CI [0.64, 1.29], p < 0.00001, random-effect model), with significant heterogeneity (I 2 = 83%, p < 0.0001) (Figure 5).

Forest plot showing the mean difference of C-reactive protein change.
Similarly, a meta-analysis for the difference of TC change between the test group and control group was conducted. A random-effect model analyzed the difference. The MD was 1.32 with 95%CI [−0.24, 2.88] (p = 0.10) and high heterogeneity among the included studies (I2 = 99%, p < 0.00001) (Figure 6). This showed that there was no significant difference in TC change between the two groups.

Forest plot showing the mean difference of TC change.
In terms of LAD change, 4 studies involving 291 patients contributed to the analysis. A random-effect model was used to evaluate the heterogeneity of LAD change due to the significant heterogeneity among included studies (p = 0.02, I 2 = 70%). The pooled analysis showed that the test group had a better improvement of LAD than the control group (MD: 0.81, 95%CI [0.06, 1.56], p = 0.03) (Figure 7).

Forest plot showing the mean difference of Left atrial diameter change.
Results of sensitivity analysis and publication bias
The included studies excluded one by one for sensitivity analysis. The heterogeneity of meta-analysis result for CRP change was decreased when Liu et al., 2013 was excluded, I 2 changed from 83% to 37% (p = 0.19), suggesting that the meta-analysis results were not robust and Liu 2013 was one the sources of heterogeneity. However, the pooled result did not change significantly. The p-value of the overall effect was still less than 0.00001.
The funnel plot for the rate of AF recurrence seemed to be asymmetric (Figure 8), but the Egger’s regression indicated no obvious publication bias (p = 0.78).

Funnel plot for publication bias in this meta-analysis.
Discussion
In our study, we comprehensively reviewed and pooled results from 8 RCTs with a total of 758 patients who compared statin-amiodarone treatment and amiodarone treatment alone for AF patients in terms of AF recurrence CRP change, TC change, and LAD change. The results revealed that for patients with AF, statin-amiodarone resulted in a significant improvement in the decrease of AF recurrence (RR = 0.58, 95%CI [0.48, 0.73]; p < 0.00001), CRP level (MD: 0.96, 95%CI [0.64, 1.29], p < 0.00001) and LAD (MD: 0.81, 95%CI [0.06, 1.56], p = 0.03) compared with amiodarone alone.
At present, the pathogenesis of AF has not been clarified. Still, in recent years, more and more studies show that inflammation plays an important role in the occurrence, development, and maintenance of AF and is an independent pathogenic factor of AF.30,31 Frustaci observed inflammatory infiltration in atrial muscle tissue of patients with AF, which confirmed the relationship between inflammation and AF at the tissue level. 32
Shiroshita confirmed in animal experiments that glucocorticoid anti-inflammatory drugs could prevent the progression of AF. 33 As an important indicator of inflammation in vivo, CRP is not only related to the persistence and development of AF but also related to the recurrence of AF and the enlargement of the left atrium. Chung found that the serum CRP level of patients with persistent AF was higher than that of patients with paroxysmal AF. 34
Several studies have reported that statin therapy was beneficial in patients with AF.35–37 Our study showed that statin-amiodarone was more effective than amiodarone alone in reducing serum CRP and maintaining sinus rhythm, which may be related to statins reducing the level of inflammatory mediator CRP. As an important inflammatory marker, CRP participates in local or systemic inflammatory responses. 34 Statins inhibit atrial remodeling induced by AF through anti-inflammatory, anti-oxidation, endothelial function regulation, and ion channel conduction to reduce the recurrence of AF and better maintain sinus rhythm.38,39
Although our study confirmed the advantages of statin-amiodarone, we should pay special attention to the drug interactions. Amiodarone and statins have some rare and serious adverse reactions.40–42 The combination of the two drugs may cause new adverse reactions or make the adverse reactions superimposed. For example, the combination of simvastatin and amiodarone will increase the risk of rhabdomyolysis and liver and kidney injury.43,44 Therefore, liver function, chest X-ray, and electrocardiogram should be reviewed regularly during the treatment.
Several limitations to our study should be noted. Firstly, the number of RCT literature about statin-amiodarone and amiodarone alone in the treatment of AF is small, and the total sample size is small, so it is not possible to further analyze the effects of different types of AF. Secondly, although we found that the conclusion is stable through sensitivity analysis, we cannot ignore the significant heterogeneity between studies. Thirdly, due to the different follow-up time after intervention in included studies, the recurrence rate of AF may be inaccurate, which may lead to some problems in the evaluation of pooled recurrence rate of AF. Fourthly, since there is no matching comparison between the test group and the control group for the risk factors of AF, we cannot know their impact on our results. Therefore, it is necessary to carry out larger sample, randomized, double blind controlled trials.
Conclusion
In sum up, we found that statin-amiodarone was better than amiodarone alone in the treatment of AF. It can more effectively reduce CRP level, LAD and reduce the conversion of AF. Limited by a number and quality of included studies, the reliability of the conclusions was reduced. Therefore, in the future, multi-center, large sample RCTs should be carried out to verify the conclusion.
Footnotes
Acknowledgements
YW and ZN participated in the conception and design of the study, library searches and assembling relevant literature, critical review of the paper, supervising the writing of the paper, and database management. XZ participated in data collection, library searches and assembling relevant literature, writing the paper, and critical review of the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by
(1) Pudong New Area Health Committee discipline leader training program (PWRD2020–20).
(2) Key specialty projects of Shanghai Municipal Health Commission (ZK2019B25).
(3) Key sub-specialty of Pudong New Area Health Committee (PWZy2020-08).
(4) Pudong New Area Health Committee peak discipline construction (PWYgf2021-04).
(5) Epidemiological investigation of atrial fibrillation in Pudong New Area and prospective cohort study on the whole process management of atrial fibrillation under the mode of graded diagnosis and treatment (PKJ2021-Y33).
Ethical approval
This study is a Meta-analysis. We have obtained a statement from the ethics committee of Shanghai Pudong Hospital that ruled that no formal ethics approval was required in this particular Meta-analysis.