
Abstract
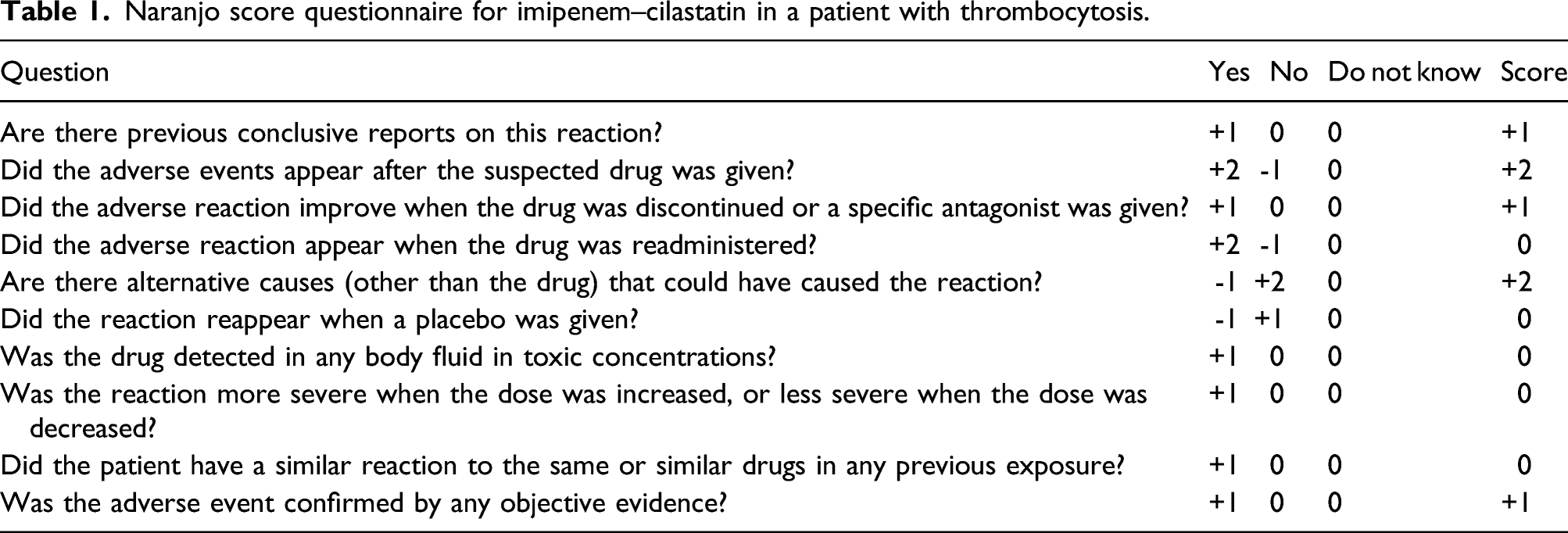
Drug-induced thrombocytosis is difficult to identify and is rarely reported. Here, we report a probable rare case of imipenem–cilastatin-induced thrombocytosis in a 51-year-old female. The patient received imipenem–cilastatin treatment because of an intra-abdominal infection, following which the platelet count increased to a peak value of 1058×109 cells/L in 14 days. When imipenem–cilastatin was replaced by levofloxacin and amikacin, the platelet count decreased progressively and remained within the normal range until the 6-month follow-up. Moreover, platelet counts were independent of the infection. Thrombocytosis was probably attributable to imipenem–cilastatin with a Naranjo score of seven. This is a probable rare case in which the thrombocytosis was likely an adverse reaction induced by imipenem–cilastatin. We suggest that clinicians need to be vigilant concerning the impact of imipenem–cilastatin on platelet count in patients with thrombocytosis.
Introduction
Imipenem-cilastatin is a commonly used broad-spectrum carbapenem for the treatment of complicated infections. 1 It has shown good safety and efficacy; however, rare adverse effects, induced by one or both components, have been discovered gradually as it becomes more widely used. Common adverse events reported with imipenem–cilastatin include irritation at the injection site, diarrhea, rash, nausea, and vomiting. 2 A rare adverse event of imipenem–cilastatin is a hematologic reaction, including thrombocytopenia and thrombocytosis.3,4 The rare effect of imipenem-cilastatin on platelets appears as thrombocytopenia at a rate of <1% in adults. 5 Thrombocytosis caused by imipenem–cilastatin is rarer than thrombocytopenia but may be related to a thromboembolism or a hemorrhagic event. 6 Thrombocytosis can be defined as the abnormal accumulation of platelets in the blood with a threshold of >450 × 109 cells/L for adults and can be further categorized into primary (essential) and secondary (reactive) thrombocytosis.7,8 Potential factors that can contribute to secondary thrombocytosis include acute blood loss, infection, inflammation, hemolytic anemia, and drug reaction.9,10 Drugs may cause thrombocytosis, but this is rarely reported. 9 Although thrombocytosis was found in patients with infections receiving imipenem–cilastatin, this adverse event was not attributed to imipenem–cilastatin because of coexisting confounding factors, mainly infection. 3 Here, we report a rare case of thrombocytosis that was probably attributable to imipenem–cilastatin treatment.
Case presentation
Naranjo score questionnaire for imipenem–cilastatin in a patient with thrombocytosis.
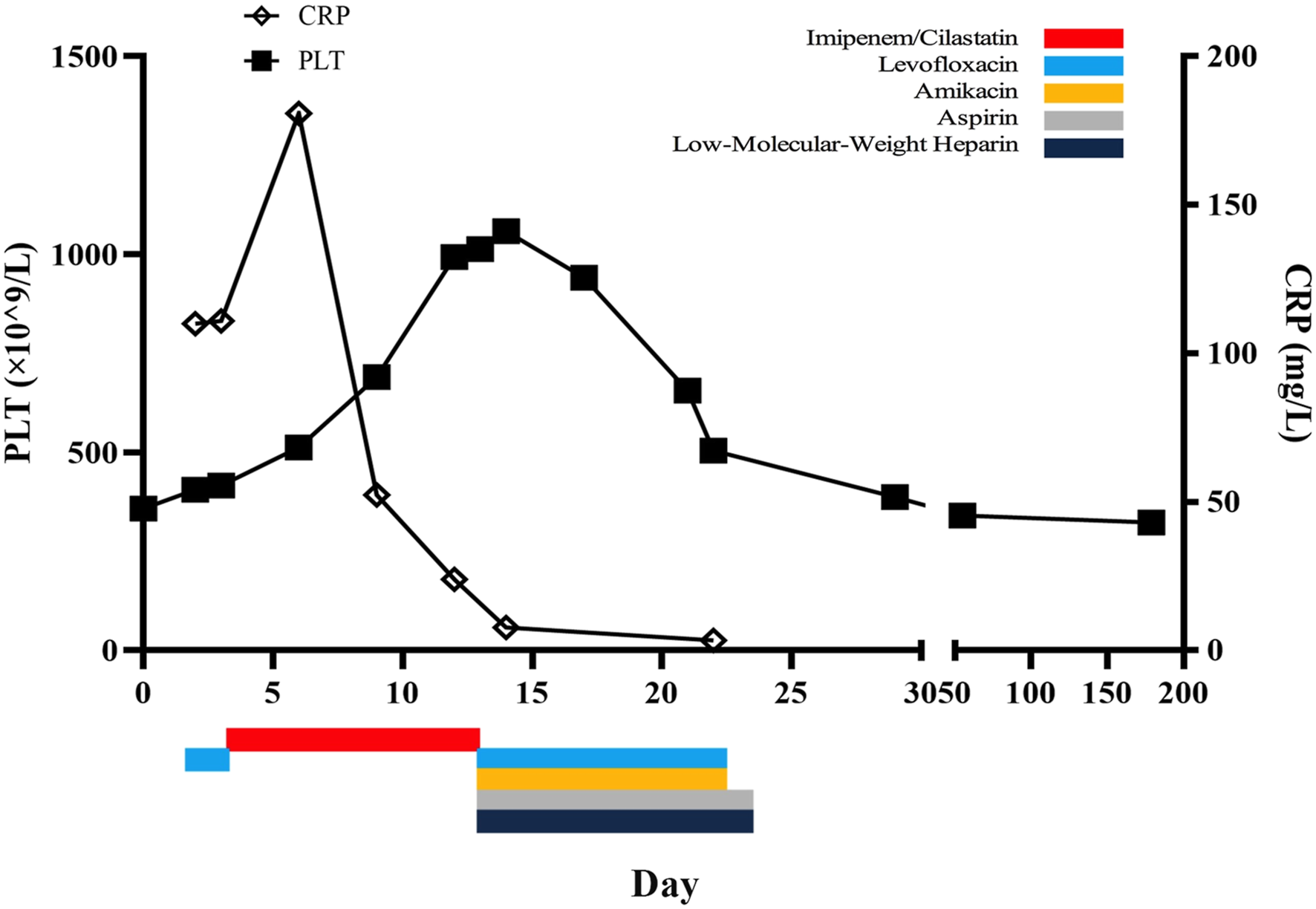
Timeline showing the patient’s platelet counts and timing of specific drug administration. Dose of each drug: imipenem-cilastatin, 0.5 g every 8 h, intravenous infusion; levofloxacin, 0.5 g every 24 h, intravenous infusion; amikacin, 0.4 g every 24 h, intravenous infusion; aspirin, 100 mg every day, oral; low-molecular-weight heparin, and 4100 IU every day, subcutaneous injection.
Laboratory findings for a patient who developed thrombocytosis during imipenem–cilastatin treatment.
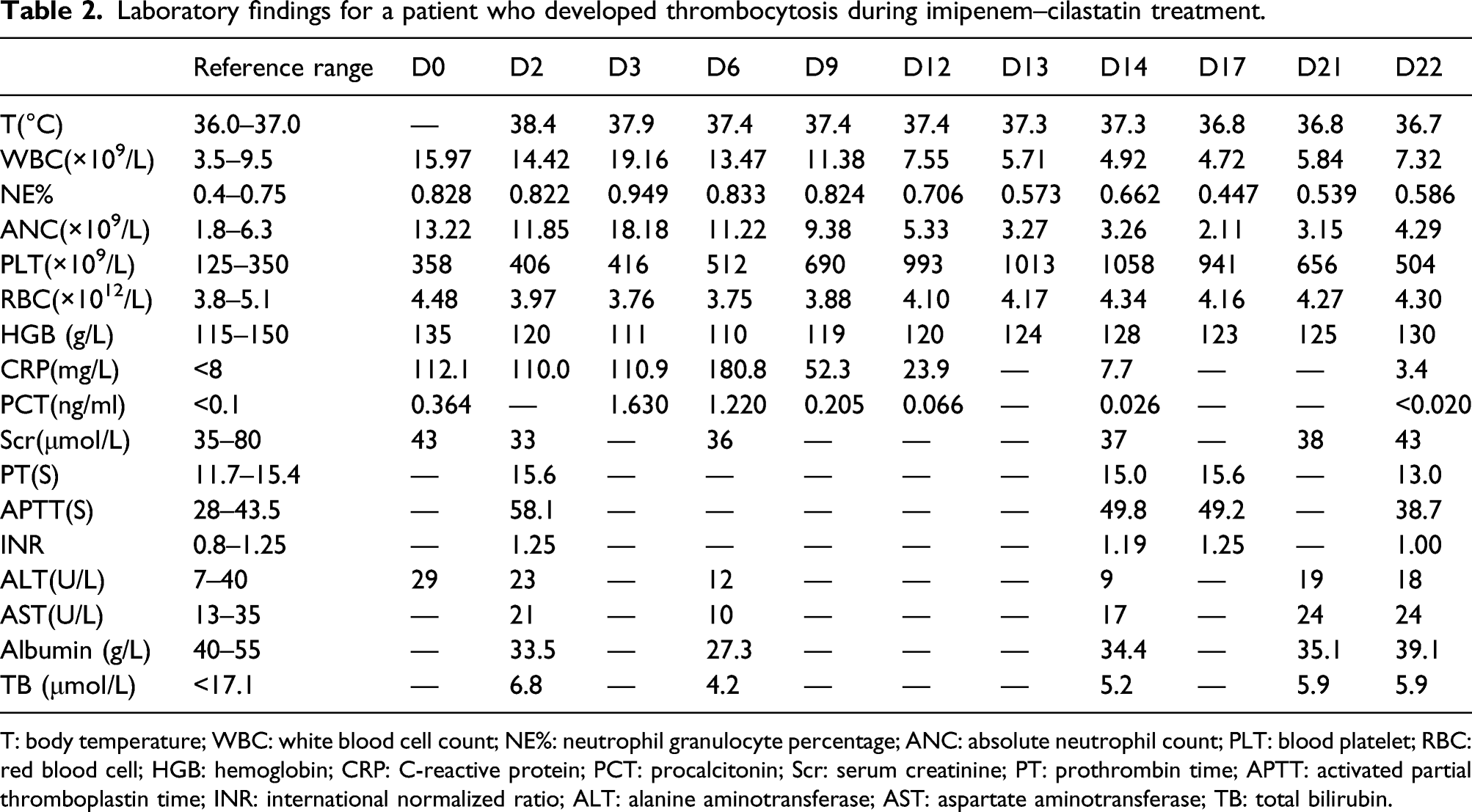
T: body temperature; WBC: white blood cell count; NE%: neutrophil granulocyte percentage; ANC: absolute neutrophil count; PLT: blood platelet; RBC: red blood cell; HGB: hemoglobin; CRP: C-reactive protein; PCT: procalcitonin; Scr: serum creatinine; PT: prothrombin time; APTT: activated partial thromboplastin time; INR: international normalized ratio; ALT: alanine aminotransferase; AST: aspartate aminotransferase; TB: total bilirubin.
The patient received blood tests at 5 days, 1 month, and 6 months after discharge, and platelet counts were all within the normal range. We therefore concluded that thrombocytosis was probably induced by imipenem–cilastatin treatment. Written informed consent was obtained from the patient for her anonymized information to be published in this article.
Discussion
We have reported a rare case of thrombocytosis probably induced by imipenem–cilastatin treatment. Thrombocytosis can be diagnosed on clinical evidence; however, the type of thrombocytosis and the cause of secondary thrombocytosis are always difficult to determine. 8 Patients with thrombocytosis always had multiple factors contributing to their condition. In the current case, platelet count was independent of infection progression and recovery. Pharmacological treatment was simple and so this adverse effect could be attributed to imipenem–cilastatin according to the Naranjo scale. Imipenem–cilastatin combination therapy is frequently used in patients with severe infections, and imipenem–cilastatin-induced thrombocytosis may be masked by other confounding factors. We suggest that imipenem–cilastatin should be considered as a possible cause in patients with thrombocytosis.
Current literature regarding drug-induced thrombocytosis covers a wide variety of drugs and no pattern is evident as of yet. 9 Some antibiotics have been implicated in the development of thrombocytosis,11,12 and this was a rare case in which it was concluded that thrombocytosis was probably induced by imipenem-cilastatin. Thrombopoietin, interleukin-6, and interleukin-11 are considered key elements in the regulation of platelets and in the development of thrombocytosis. 13 However, the effect of imipenem–cilastatin on these factors has not been reported and the exact mechanism of drug-induced thrombocytosis should be investigated in future studies.
It has been reported that patients with secondary thrombocytosis did not need specific anti-platelet or platelet-lowering therapy. 8 Identifying the cause of secondary thrombocytosis and then treating the underlying disease is more important. In this case, thrombocytosis was probably attributed to imipenem–cilastatin treatment and then these drugs were discontinued. The patient had a high platelet count and was evaluated to be at risk of a thromboembolism; therefore, aspirin and low-molecular-weight heparin were also administered. The platelet count decreased progressively over several days and ultimately returned to the normal range. Imipenem–cilastatin-induced thrombocytosis did not cause any long-term effects in this case.
Conclusion
This was a probable rare case of thrombocytosis induced by imipenem–cilastatin treatment and suggests that clinicians need to be vigilant regarding the impact of imipenem–cilastatin on platelet count. Replacement with other antibiotic classes and evaluation of the risk of thromboembolism events should be performed when thrombocytosis is induced in patients by imipenem–cilastatin.
Footnotes
Author contributions
Huadong Chen is the primary author and was responsible for data acquisition, analysis, interpretation and manuscript preparation. Xing’e Xu, Piaopiao Li, and Zhenglin Xu participated in data interpretation and manuscript editing. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Science and Technology Bureau of Jinhua, Zhejiang (2019-4–110).
Ethic approval
Ethical approval to report this case was obtained from Ethics committee of Dongyang People’s Hospital (approval number DONGRENYI2021-YX-044).
Informed consent
Written informed consent was obtained from the patient for her anonymized information to be published in this article.
Data availability statement
Data are contained within the article.