
Abstract
Capsule Summary
Since the approval of dupilumab for moderate-to-severe atopic dermatitis (AD) in 2017, events of facial rash have been reported in the literature.
We conducted a pooled analysis of 14 randomized, placebo-controlled clinical trials of dupilumab for moderate-to-severe AD to report incidence of facial rash events.
Our analysis shows a small increase of facial rash events in dupilumab-treated patients, but most events were mild-to-moderate and did not require treatment discontinuation.
INTRODUCTION
Moderate-to-severe atopic dermatitis (AD) is a chronic systemic disease characterized by intense pruritus and recurrent eczematous lesions, which frequently presents early in life. 1 Head and neck dermatitis is a common phenotype of AD.2–4
Dupilumab, a fully human monoclonal antibody that targets the shared receptor component for interleukin (IL)−4 and IL-13, provided rapid, significant, and sustained improvement in the signs and symptoms of AD in pediatric and adult patients with moderate-to-severe AD in randomized, placebo-controlled clinical trials.5,6 Notably, dupilumab treatment significantly improved severity of AD signs on the head and neck (as measured by regional Eczema Area and Severity Index [EASI] component scores for erythema, infiltrations/papulation, excoriation, and lichenification) in infants, children, adolescents, and adults.2,7–9
After the initial approval of dupilumab for moderate-to-severe AD in adults in 2017, there have been case reports describing facial rash events in both adults and children.10–52 The clinical features in these reports varied, with scaling, redness, edema, plaques, burning, itching, and flushing reported on regions of the head and neck. In many cases, facial rash events resolved over time without necessitating withdrawal from dupilumab treatment, although in some cases the patients received additional therapeutic interventions (eg, antifungals, allergen avoidance, topical calcineurin inhibitors/topical corticosteroids [TCS], antihistamines). On the basis of these reports, as well as a review of the sponsor’s pharmacovigilance database, “facial rash” was designated as a post-marketing adverse drug reaction for dupilumab.
Several publications noted that these events were not observed in dupilumab clinical trials. Given the resemblance to facial AD, facial rash may not have been considered worsening of AD and thus not reported as an adverse event in clinical trials. There is also the possibility that this is a consequence of the methodology used to record adverse events for clinical trials intended for regulatory submission. The Medical Dictionary for Regulatory Activities (MedDRA) terminology was developed as a medically validated terminology for utilization throughout the regulatory process and has a specific hierarchy (Fig. 1). The High Level Terms and High Level Group Terms are analyzed primarily for registration purposes, as they facilitate data retrieval and presentation by providing clinically relevant grouping of terms. Preferred Terms (PTs) are widely used for regulatory submissions but generally do not permit identification of localized conditions such as “Redness Facial” or “Facial Rash.”53,54 Only the Lowest Level Terms (LLTs) of the MedDRA hierarchy include language specifying anatomical location of rash or erythema. To gain further insights on the incidence of facial rash events with dupilumab treatment, as reported through MedDRA, we conducted a detailed analysis focused on the LLTs of the pooled safety data from 14 randomized, placebo-controlled trials of dupilumab, including patients with AD aged 6 years and older.
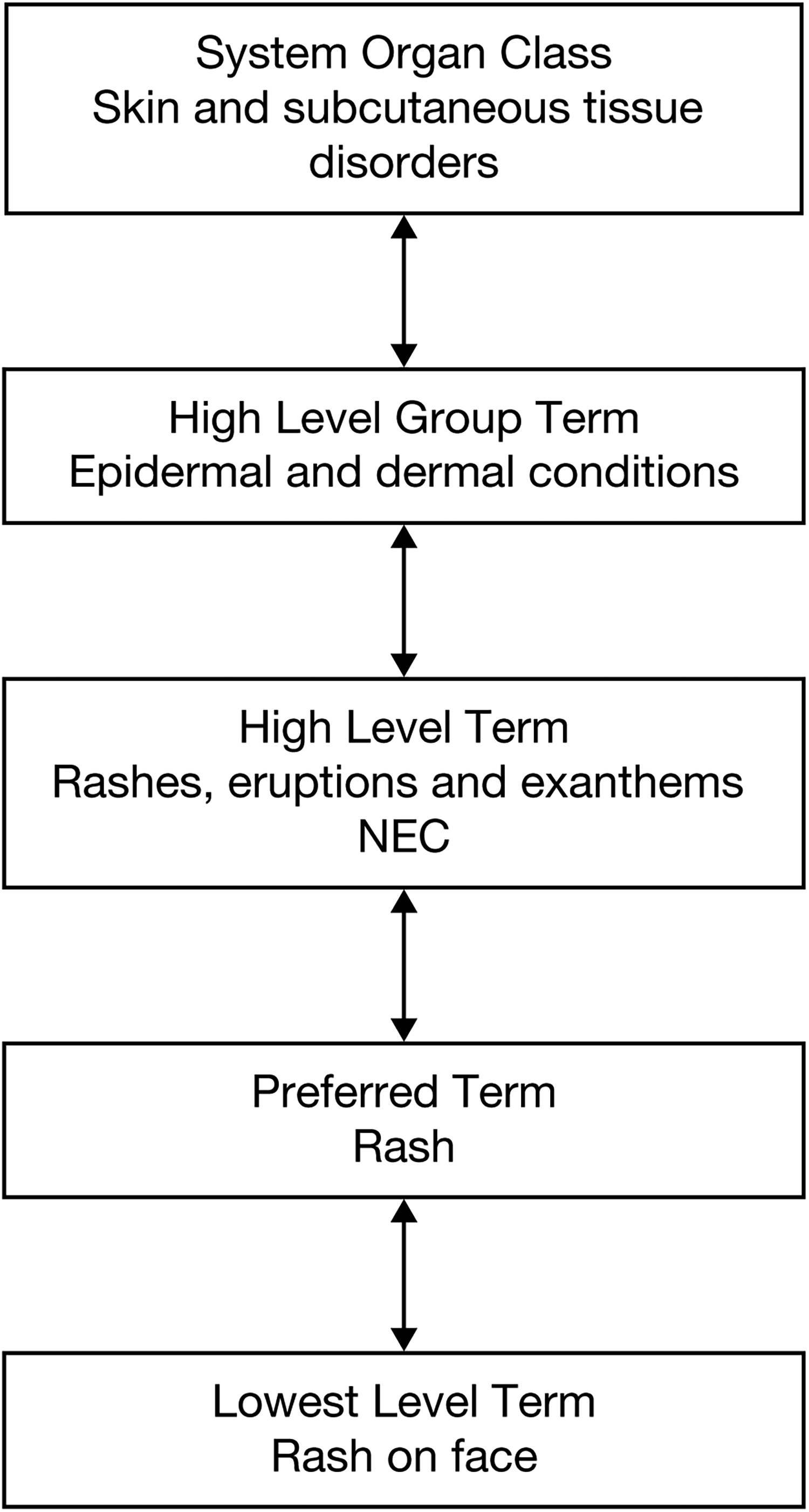
MedDRA term hierarchy for LLT Rash on Face (an example LLT used in this analysis). LLT, lowest level term; MedDRA, Medical Dictionary for Regulatory Activities; NEC, not elsewhere classified.
METHODS
Study Design, Patients, and Treatment
Data were pooled from 14 randomized, placebo-controlled trials of patients with moderate-to-severe AD (or severe AD only for patients 6–11 years). Trial details are presented in Table 1.
Studies and Treatment Arms
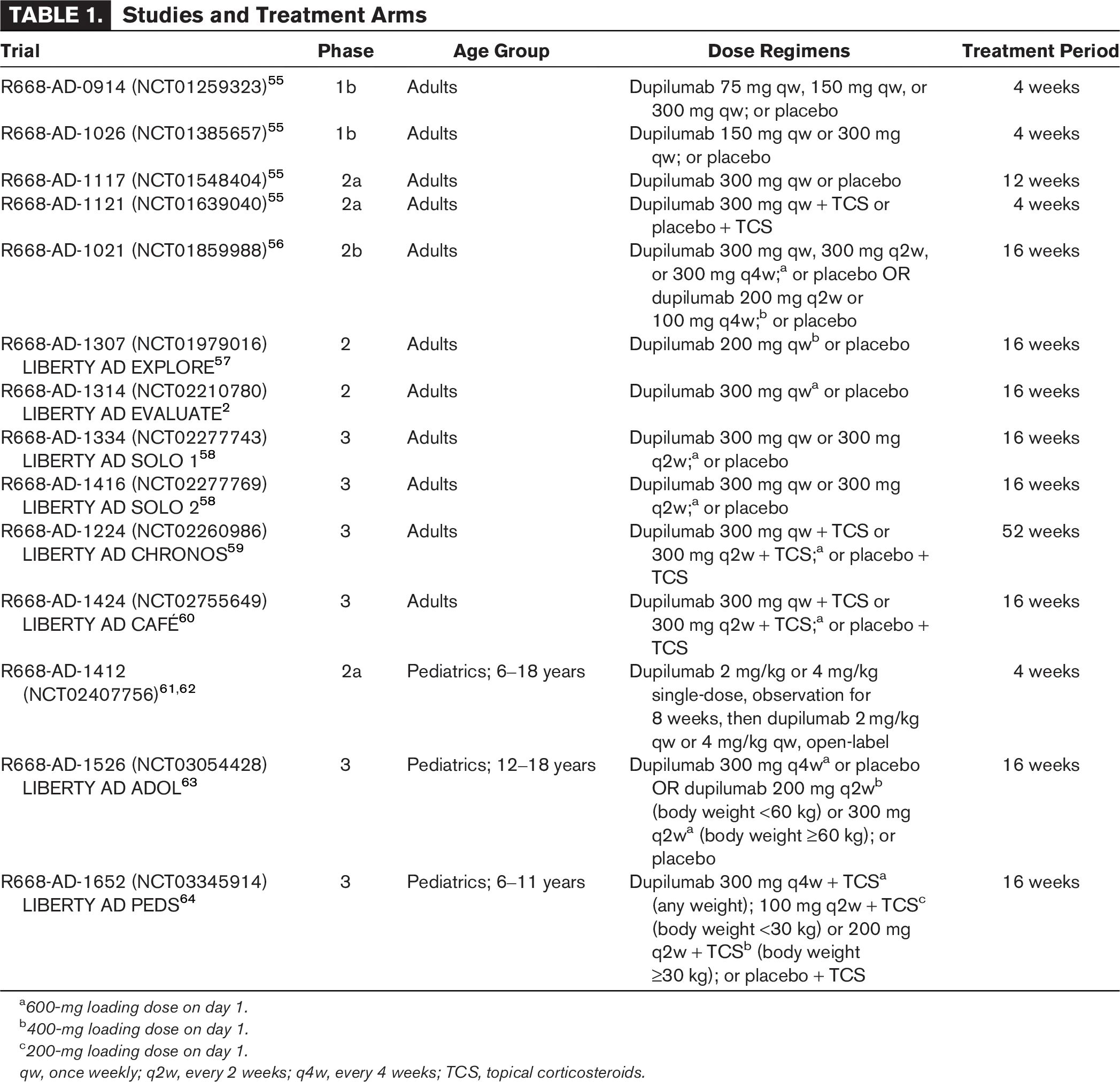
600-mg loading dose on day 1.
400-mg loading dose on day 1.
200-mg loading dose on day 1.
qw, once weekly; q2w, every 2 weeks; q4w, every 4 weeks; TCS, topical corticosteroids.
Ethics
All studies were conducted in accordance with the Declaration of Helsinki, the International Council for Harmonisation guideline, Good Clinical Practice, and local applicable regulatory requirements, including institutional review board approval. All patients provided written informed consent before any study procedures began.
Analysis
The pooled dataset was searched for facial rash treatment-emergent adverse events (TEAEs) that occurred during the study treatment period, as defined by the following MedDRA PTs and LLTs: PTs are Dermatitis contact and Rosacea, and LLTs are Dermatitic reaction of face, Dermatitic reaction of neck, Dry rash face, Dry rash neck, Eczema facial, Eruption facial, Erythema facial, Face red, Facial flushing, Facial rash, Flushed face, Flushing of face, Neck rash, Rash face, Rash on face, Red face, Red neck, Redness facial, Redness of face, Rosacea-like dermatitis, and Allergic contact dermatitis. Events of Contact dermatitis were only included in this analysis if they were reported to be affecting the face and/or neck.
Outcomes Assessed in This Analysis
Outcomes assessed in this analysis included the overall incidence of facial rash: TEAEs, TEAEs considered by the investigator to be related to study drug, treatment-emergent serious adverse events (TE-SAEs), events leading to permanent discontinuation of study drug, and TEAEs by PTs and LLTs. The severity, duration, time to onset, and outcome (ie, whether the TEAE recovered/resolved during the treatment period) are also described. All statistics are descriptive.
RESULTS
Patients
A total of 3964 patients (1349 placebo and 2615 dupilumab, corresponding to 706.6 and 1306.3 patient-years [PY] of exposure) were included in the pooled dataset. Baseline demographics and disease characteristics were similar across the placebo and dupilumab groups in the overall population and in the subset of patients with facial rash events (Table 2).
Baseline Demographics and Disease Characteristics
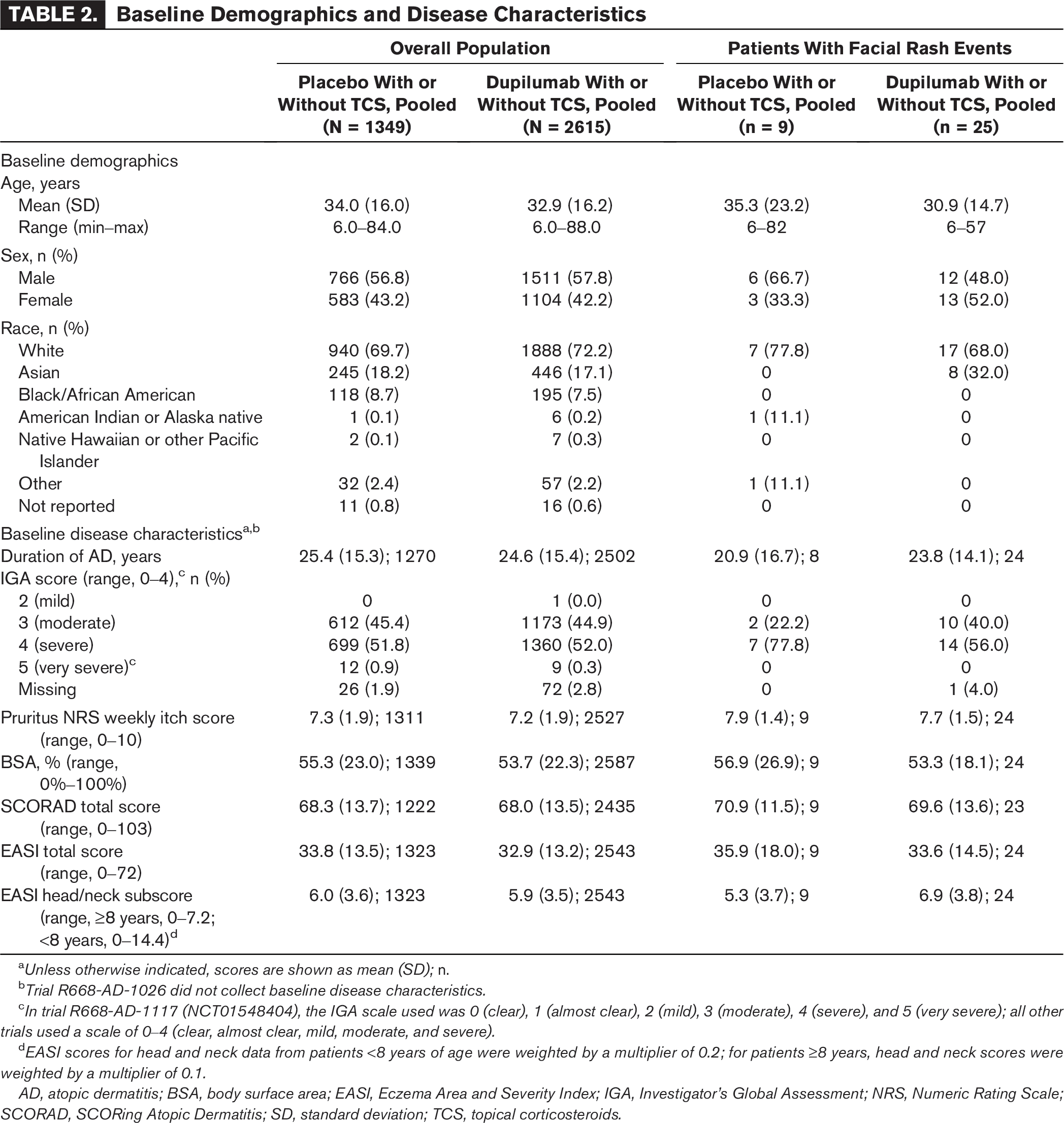
Unless otherwise indicated, scores are shown as mean (SD); n.
Trial R668-AD-1026 did not collect baseline disease characteristics.
In trial R668-AD-1117 (NCT01548404), the IGA scale used was 0 (clear), 1 (almost clear), 2 (mild), 3 (moderate), 4 (severe), and 5 (very severe); all other trials used a scale of 0–4 (clear, almost clear, mild, moderate, and severe).
EASI scores for head and neck data from patients <8 years of age were weighted by a multiplier of 0.2; for patients ≥8 years, head and neck scores were weighted by a multiplier of 0.1.
AD, atopic dermatitis; BSA, body surface area; EASI, Eczema Area and Severity Index; IGA, Investigator’s Global Assessment; NRS, Numeric Rating Scale; SCORAD, SCORing Atopic Dermatitis; SD, standard deviation; TCS, topical corticosteroids.
Facial Rash Events
A total of 9 facial rash events were reported in 9 (0.7%, 1.3 number of events [nE]/100PY) patients in the placebo group and 28 in 25 (1.0%, 2.1 nE/100PY) patients in the dupilumab group; among these, 2 (0.1%, 0.3 nE/100PY) placebo-treated and 5 (0.2%, 0.5 nE/100PY) dupilumab-treated patients experienced events deemed by the investigator to be related to the study drug (Table 3). No patient experienced a facial rash TE-SAE or a facial rash TEAE leading to permanent drug discontinuation.
Events of Facial Rash
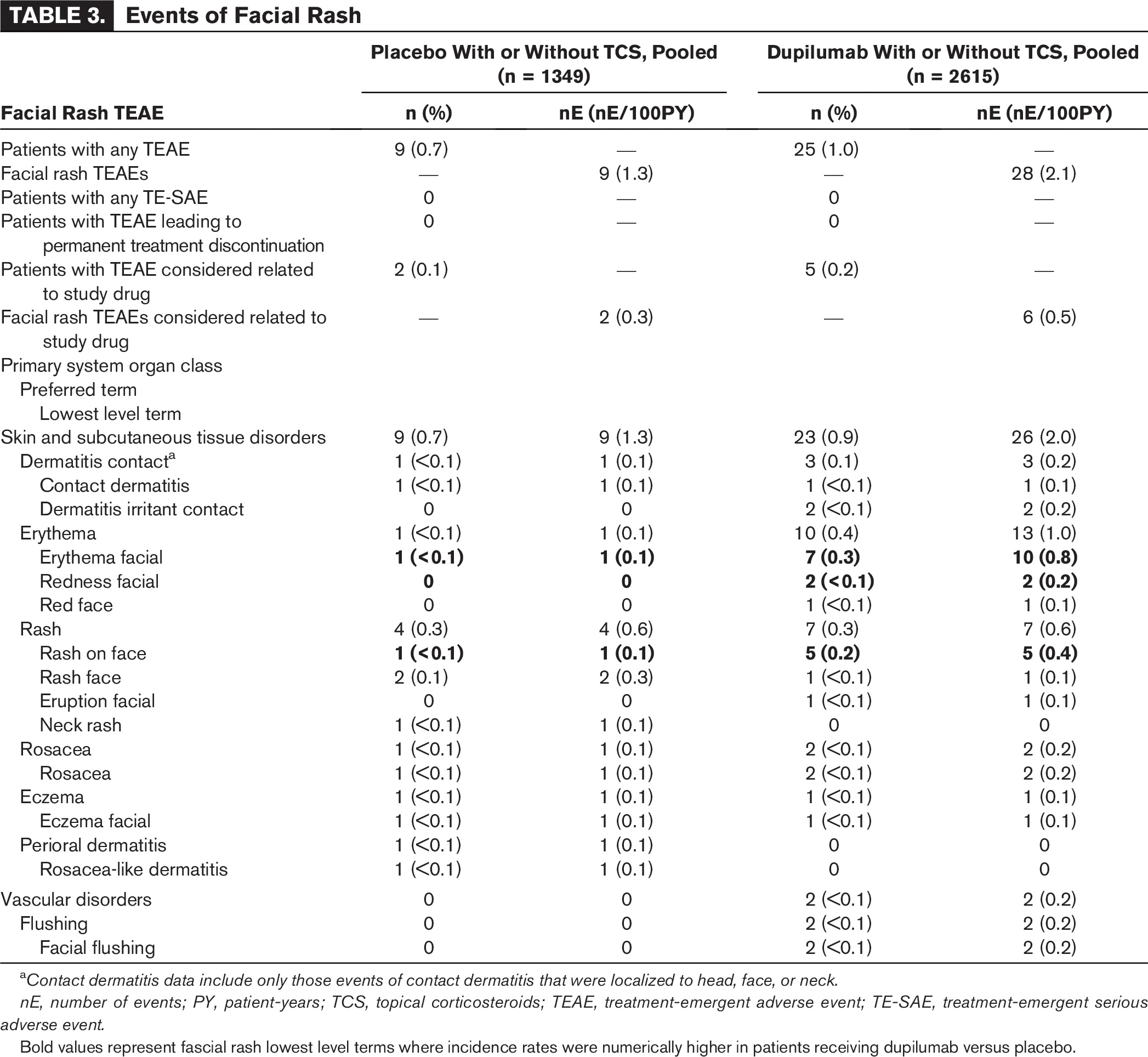
Contact dermatitis data include only those events of contact dermatitis that were localized to head, face, or neck.
nE, number of events; PY, patient-years; TCS, topical corticosteroids; TEAE, treatment-emergent adverse event; TE-SAE, treatment-emergent serious adverse event.
Bold values represent fascial rash lowest level terms where incidence rates were numerically higher in patients receiving dupilumab versus placebo.
At the MedDRA LLT level, incidences of facial rash LLTs were generally similar across treatment groups; however, rates of Erythema facial (7 [0.3%, 0.8 nE/100PY] vs 1 [<0.1%, 0.1 nE/100PY]), Redness facial (2 [<0.1%, 0.2 nE/100PY] vs 0), and Rash on face (5 [0.2%, 0.4 nE/100PY] vs 1 [<0.1%, 0.1 nE/100PY]) were numerically higher in dupilumab-treated patients than in placebo-treated patients.
Regarding the characteristics of these facial rash events, the time to onset was similar for the placebo and the dupilumab groups (mean [SD]: 125.0 [124.8] days for placebo vs 130.9 [121.1] days for dupilumab), as was their duration (mean [SD]: duration in days: 13.4 [13.8] for placebo and 12.5 [15.9] for dupilumab) (Table 4). The shortest time to onset was 30 days in the placebo group and 2 days in the dupilumab group, and the longest was 366 and 351 days, respectively. The shortest duration of the facial rash event for both groups was 1 day, and the longest was 34 days for placebo and 44 days for dupilumab. Most events were of mild or moderate intensity. Severe events were reported in 2 of 25 (8.0%, 0.2 nE/100PY) dupilumab-treated patients and none in placebo-treated patients (Table 4). In most cases, facial rash events recovered/resolved or were recovering/resolving by the end of the treatment period; 7 of 9 (78%) placebo-treated and 18 of 25 (72%) dupilumab-treated patients reported that facial rash events recovered/resolved, and 1 of 25 (4%) dupilumab-treated patients reported an event that was recovering/resolving (Table 4).
Duration, Time to Onset, Severity, and Resolution of Facial Rash TEAEs
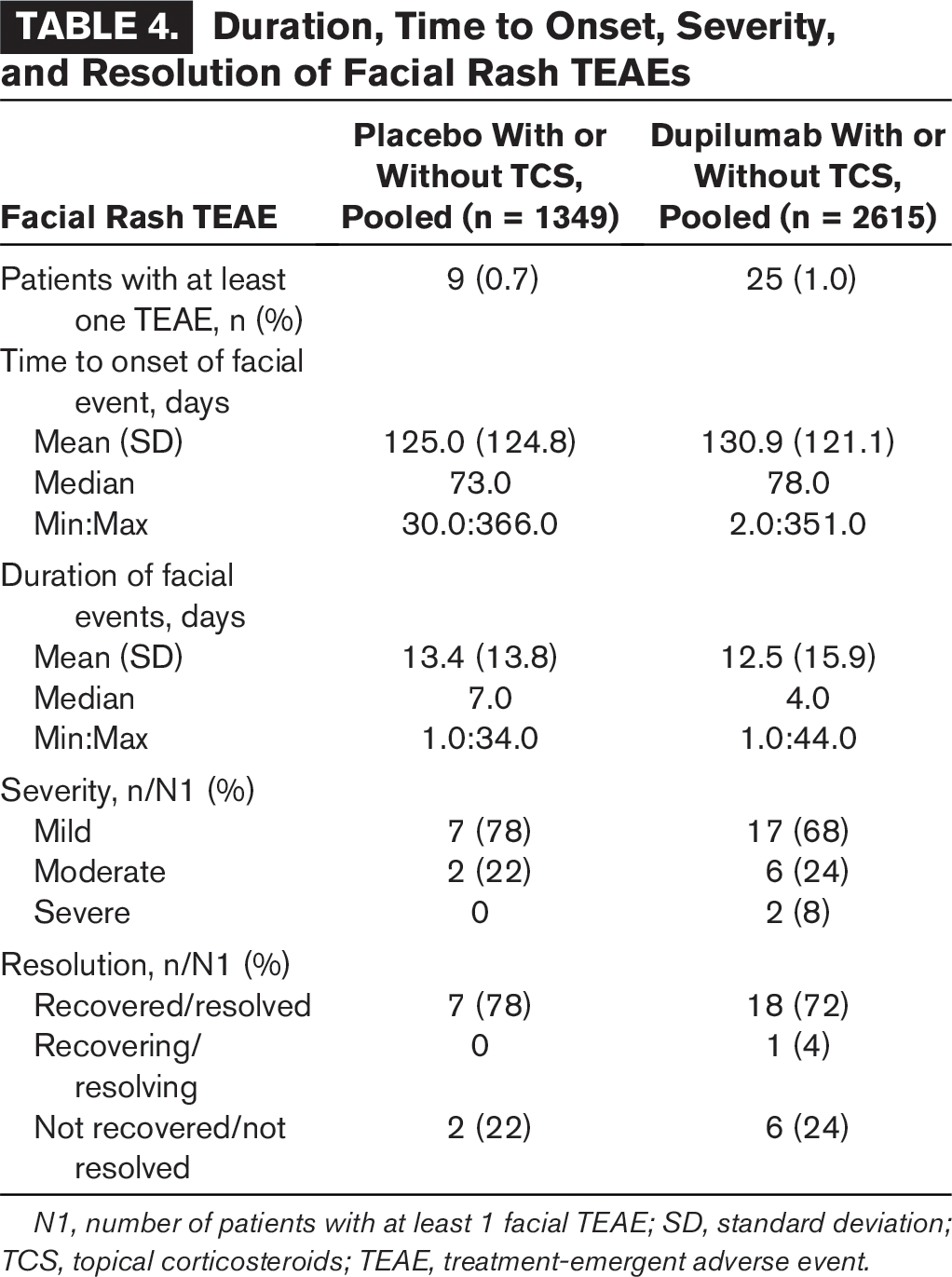
N1, number of patients with at least 1 facial TEAE; SD, standard deviation; TCS, topical corticosteroids; TEAE, treatment-emergent adverse event.
DISCUSSION
In this pooled analysis of 1349 placebo-treated patients and 2615 dupilumab-treated patients from 14 randomized, placebo-controlled clinical trials in adults and children ≥6 years of age with moderate-to-severe AD, the overall incidence of facial rash events was low but slightly higher in the dupilumab group compared with the placebo group. At the MedDRA LLT level, more dupilumab-treated patients reported “Erythema facial” and “Rash on face.” Most facial rash events were mild to moderate in severity and nonserious, and most recovered/resolved during the study period. None resulted in treatment discontinuation or study withdrawal.
In real-world patient cohorts, facial rash events have been described in approximately 10% of patients of diverse age groups treated with dupilumab,15,19,26,37,65,66 although a lower incidence has also been reported.35,45 Facial rash events may also masquerade as AD and thus be under-reported, although previous analyses based on EASI data on dupilumab clinical trials in adults, adolescents, and children with moderate-to-severe AD demonstrated that dupilumab resulted in a significant improvement of AD signs in the head and neck, similar to the levels of improvement observed in other body regions.2,7,8 Efficacy was similar in head-to-head trials of dupilumab versus abrocitinib or upadacitinib,67,68 but some reports indicate that face and neck AD may improve but still persist on dupilumab. 69 While there may be under-reporting, another possible explanation for the lower incidence reported here may be the duration of treatment. Most trials in this pooled analysis were 16 weeks or less in duration; only one trial (CHRONOS) was 52 weeks in duration. The time to onset of facial rash events reported ranges from hours after dupilumab injection15,20,23,29 to up to 8 months after treatment initiation.21,35 In case series, the mean time to onset varied between 9.3, 13 22.25, 18 29.5, 26 and 36.9 35 weeks, suggesting eventually some cases would not be captured within the 16-week study period. The time to onset while on dupilumab in this analysis ranged from 2 to 351 days, and the event duration from 1 to 44 days.
In a real-world, multicenter, prospective, cohort study of 162 patients with severe AD from the US and South Korea, most patients (84.6%) had facial erythema prior to dupilumab treatment. 31 Overall, 88.3% of patients with previous facial erythema observed improvement with dupilumab treatment, 6.6% of patients had no change of facial erythema with dupilumab treatment, and 5.1% of patients experienced worsening of facial erythema with dupilumab treatment. 31 This is consistent with our analysis, in which most facial rash events resolved over time. In addition, regardless of resolution, no facial rash event led to permanent treatment discontinuation, a fact also observed in many published reports, although in some cases additional concomitant treatments were used.10–15,18–21,24,26–29,32,33,35,37,39,44,47,49,50,70,71 In some cases, the events resolved after switching to other treatments for AD.37,51,52
Although the etiology of facial rash events in dupilumab-treated patients is unclear, several hypotheses have been proposed, including TCS withdrawal syndrome, seborrheic dermatitis—like reactions, allergic contact dermatitis, Malassezia hypersensitivity, photosensitivity, allergic angioedema, rosacea, lupus erythematosus, Staphylococcus aureus infection, alcohol-induced facial flushing, and Demodex-related/rosacea-like or a combination of these mechanisms.10–25,27–32,37,39–42,44,47,50,51,72,73 Of note, TCS withdrawal has been associated with the development of facial rash in patients with AD, including those treated with dupilumab.25,31,74,75 The absence of biopsies and patch testing in most reported cases does not permit firm conclusions regarding pathophysiology of these events.
Strengths of this analysis include the large sample size and the fact that TEAEs were evaluated at the MedDRA LLT level. Limitations include the post hoc nature of the analyses and the short-term nature of most studies included which may limit the extrapolation of these findings for long-term dupilumab users.
CONCLUSIONS
Facial rash is a recognized adverse drug reaction for dupilumab. This analysis of pooled, randomized, placebo-controlled clinical trial data indicates that events were infrequently reported as adverse events, were mostly mild to moderate in severity, and were responsive to treatment without the need to discontinue dupilumab.