
Abstract
Objective
To explore the risk factors for inferior vena cava filter (IVCF) thrombus in orthopedic trauma patients who underwent filter placement with ongoing anticoagulation in clinical settings.
Methods
We retrospectively analyzed clinical data from fracture patients with lower extremity acute deep vein thrombosis (DVT) implanted with an IVCF admitted to Tianjin Hospital from January 2017 to December 2019. Potential risk factors, such as gender, age, diabetes, hypertension, fracture sites, thrombus location, free-floating thrombus, filter type, Injury Severity Score (ISS), and postoperative D-dimer values, were analyzed by the Chi-square test, t-test, logistic regression, and receiver operating characteristic (ROC) curve analysis.
Results
A total of 662 patients were included in our study, and filter-related thrombosis was present in 67 (10.1%) patients. No significant differences were observed in age, gender, hypertension, diabetes, fracture site, free-floating thrombus, filter type, indwelling time, and postoperative D-dimer level. Thrombus location and ISS were significantly different (p < 0.05). Popliteal DVT (P-DVT) (odds ratio [OR]: 2.130, p = 0.018) and ISS (OR: 1.135, p = 0.000) were associated with filter thrombus. Patients with P-DVT were prone to a small filter thrombus (OR: 3.231, p = 0.037). From the ROC curve analysis, the diagnostic value of ISS was 24.5 and 26.5 for patients with filter and massive filter thrombus, respectively.
Conclusion
Thrombus location and ISS were independent risk factors for filter thrombus in patients with traumatic fractures. P-DVT had a higher potential to result in a small filter thrombus and an ISS value >26.5, which was considered a significant massive filter thrombus predictor.
Introduction
Deep vein thrombosis (DVT) is the most common and severe complication in patients with traumatic fractures, as it potentially increases mortality due to pulmonary embolism (PE). 1 Considerable research has indicated that DVT incidence in trauma patients varies from 0.76% to 5%, even though prophylactic measures such as rivaroxaban and low-molecular-weight heparin have been used for optimal prophylaxis.2–4 It is accepted that inferior vena cava filter (IVCF) implantation is an important preventative method for PE 5 and has been shown to lower the incidence of PE from 60%–70% to 0.9%–5.0%. 6 However, each coin has two sides. Some studies have reported several long-term complications after permanent filter implantation, such as DVT recurrence, inferior vena cava (IVC) thrombosis and occlusion, filter fracture, penetration and migration, chronic hypotension, and dizziness.7–9 Currently, retrievable IVCFs are preferred because they avoid long-term complications.10,11 Nonetheless, if retrievable filters are not retrieved promptly, they are prone to the same complications as permanent filters.
We hypothesized that thrombosis in an IVCF is associated with thrombosis progression and shedding in the acute DVT phase. Moreover, a thrombosed IVCF may increase the risk of PE because the thrombus extends above the filter and causes recurrent PE.
12
In addition, from our experience, the larger the filter thrombus, the smaller the clots that will fall from the filter during retrieval attempts (Figure 1). Therefore, we designed and performed this study to identify the factors of IVCF thrombus and hope to help decrease the incidence of IVC thrombosis and PE and increase the incidence of retrieved IVC filters. (A) Small filter thrombosis and less small clots after retrieval; (B) Massive filter thrombosis and more small clots after retrieval.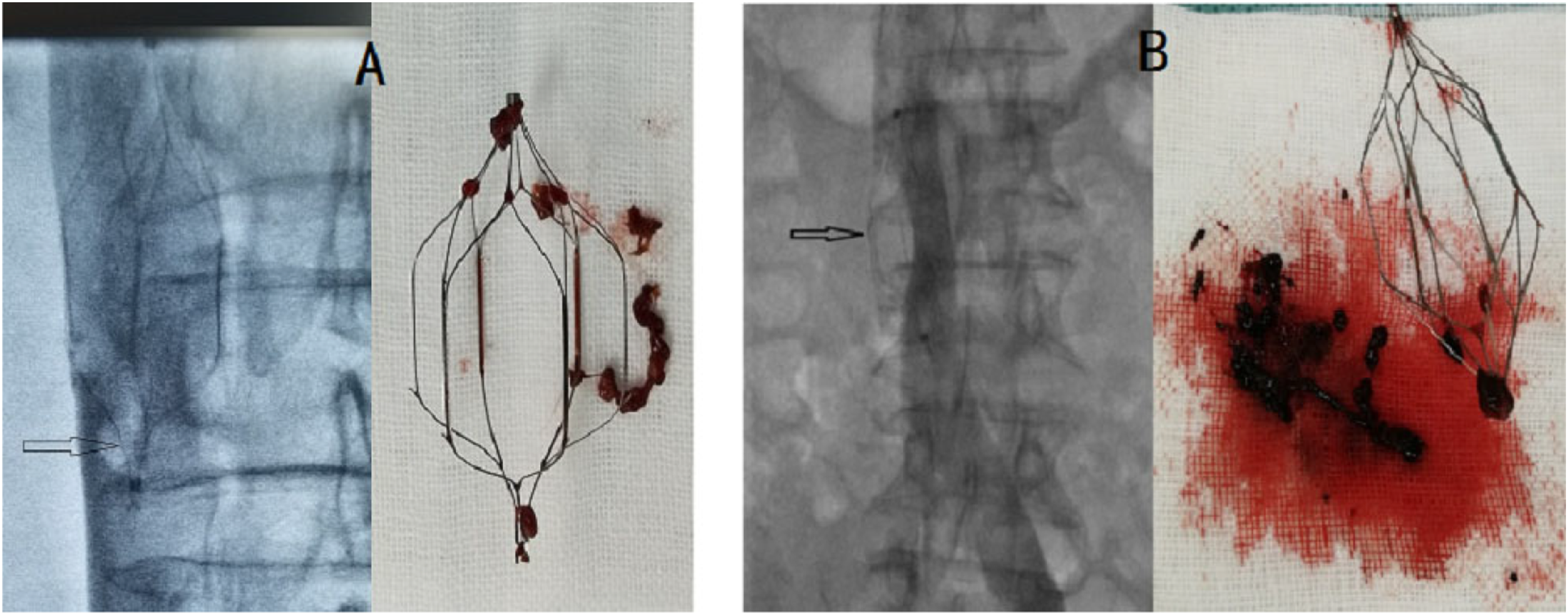
Methods
Clinical data
This retrospective study reviewed 924 orthopedic patients with acute lower extremity DVT who underwent IVCF implantation due to spine, pelvic, and lower extremity fractures between January 2017 and December 2019. The study was approved by the Ethics Committee of Tianjin Hospital (approval no. 2021-YILUNSHEN 170), and the requirement for informed consent was waived owing to the study’s retrospective nature. Study participants, including 474 males and 450 females with a mean age of 59.35 ± 14.62 years (age range, 14–80 years), were diagnosed with acute DVT by lower extremity duplex ultrasound scan, with filters implanted before orthopedic operation. After DVT was diagnosed, weight-adjusted low-molecular-weight heparin (LMWH) sodium was injected subcutaneously every 12 h (1 mg/kg). This LMWH anticoagulation treatment was performed during hospitalization but stopped temporarily at 12–24 h before and after the day of the orthopedic surgery, depending on the anesthetic mode. After leaving the hospital, the patients continued taking novel oral anticoagulants (rivaroxaban) until the anticoagulant indications disappeared. All patients underwent early ambulation or active/passive lower limb rehabilitation exercises, depending on their condition.
The exclusion criteria included the following: a history of vascular surgery, patients taking anticoagulants at admission, malignant neoplasm, personal or family history of venous thromboembolism (VTE), and patients with coagulation or severe cardiopulmonary dysfunction. We also excluded three patients who died due to circulatory failure after filter implantation due to severe trauma. In addition, 45 patients were lost to follow-up and 181 refused retrieval attempts. In total, 662 patients were included in the analysis (Figure 2). Flow diagram of study selection process.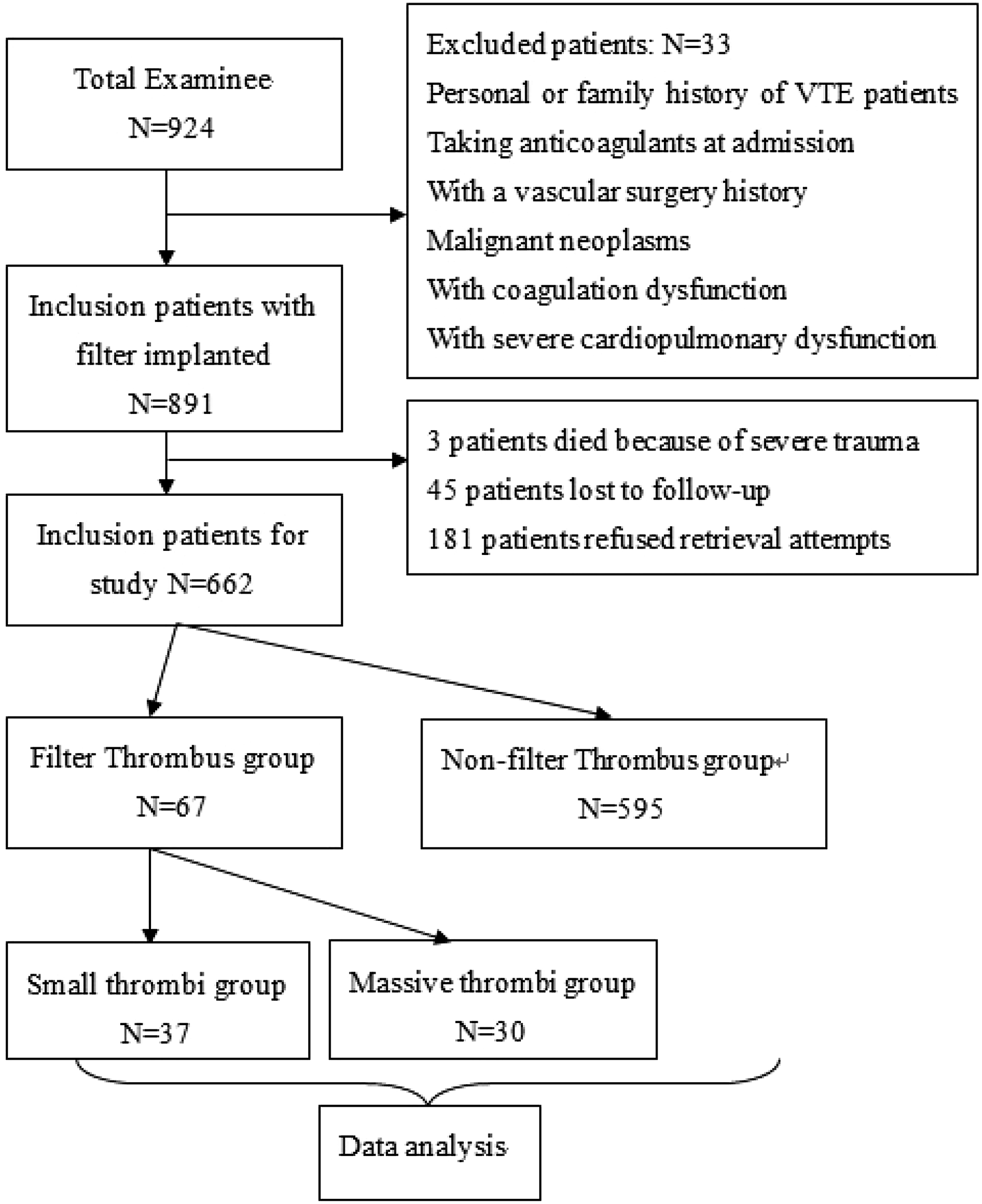
Variables and groups
We reviewed the medical records of 662 patients. Potential risk factors were noted, including gender, age, diabetes, hypertension, fracture site, thrombus location, free-floating thrombus, filter type, indwelling time, Injury Severity Score (ISS), and postoperative D-dimer level. Fracture sites were classified into six groups: (1) tibiofibula or plateau, (2) patella, (3) femur or hip, (4) pelvis, (5) spine, and (6) multiple sites (fractures at two or more sites). Thrombus location was classified into three groups: (1) above-knee DVT (AKDVT), (2) popliteal DVT (P-DVT), and (3) below-knee DVT (BKDVT). Four types of filters were used: Option Elite Filter (Argon Medical, Athens, Texas, USA), Aegisy® (Lifetech Scientific Company, Shenzhen, China; retrievable filter), OptEase® (Johnson & Johnson, Cordis Endovascular, Miami, FL, USA), and Denali® (Bard Peripheral Vascular, Tempe, Arizona). Postoperative D-dimer values were defined as the mean D-dimer level during the filter indwelling time. The participants were divided into the inferior vena cava filter thrombus (67) and non-filter thrombus (595) groups. The presence of a filter thrombus was detected using intraoperative venography (GE Innova 3100-IQ DSA, USA) after removing the IVC filter. Given some studies,13,14 we defined a small filter thrombus with clots <1 × 1 cm as the massive group. Thirty-seven patients were included in the small filter thrombus group (14, 22, and 1 in the AKDVT, P-DVT, and BKDVT groups, respectively). In comparison, 30 patients were included in the massive filter thrombus group (11, 19, and 0 in the AKDVT, P-DVT, and BKDVT groups, respectively).
Filter retrieval and filter thrombus management
The patients with acute bone fractures that require surgery and acute proximal DVT and patients with DVT undergoing surgical repair of a fracture of the knee or areas below the knee in the ipsilateral limb were performed prophylactic IVCF placement. Patients who were scheduled for surgery received treatment of a standard anticoagulation therapy. The filters were placed according to the manufacturer’s instructions. After caval venography, retrieval of a thrombus smaller than 1 cm in the filter or none during the follow-up after the filter placement was attempted using the hook filter recovery kit. Various methods, such as the use of a double-guide wire, femoral puncture to assist in changing the position of the filter, combined use of a guide-wire loop snare, and balloon, assist in providing a better angle for snaring the filter hook. If a thrombus >1 × 2 cm occurs, some treatment modalities are available for filter thrombus management, such as manual negative pressure aspiration by 10F guiding catheter, catheter-directed thrombolysis (CDT), and negative pressure aspiration thrombectomy combined with CDT. A second retrievable filter was placed above the original filter under the condition of a clot above the filter.
Venous thromboembolic diseases were managed according to the Guideline for Diagnosis and Treatment of Deep Vein Thrombosis (3rd edition) of the Chinese Society for Vascular Surgery, 15 Chinese Association of Orthopedics, 16 American College of Chest Physicians, 17 and British Committee for Standards in Hematology for therapy of venous thromboembolic disease. 18
Statistical analysis
Data were presented as means and ranges for continuous variables and percentages for incidence rates. Chi-square tests for categorical variables and/or t-tests for continuous variables were used to assess group differences. Statistical significance was set at p < 0.05. Odds ratios (OR) were presented with 95% confidence intervals (CI 95%). Multivariable logistic regression analysis was used to identify filter thrombus-associated risk factors. Receiver operating characteristic (ROC) curve analysis was used to evaluate the diagnostic value of ISS for filter thrombi. Data were analyzed using standard statistical software (SPSS version 18.0, Chicago, IL, USA).
Results
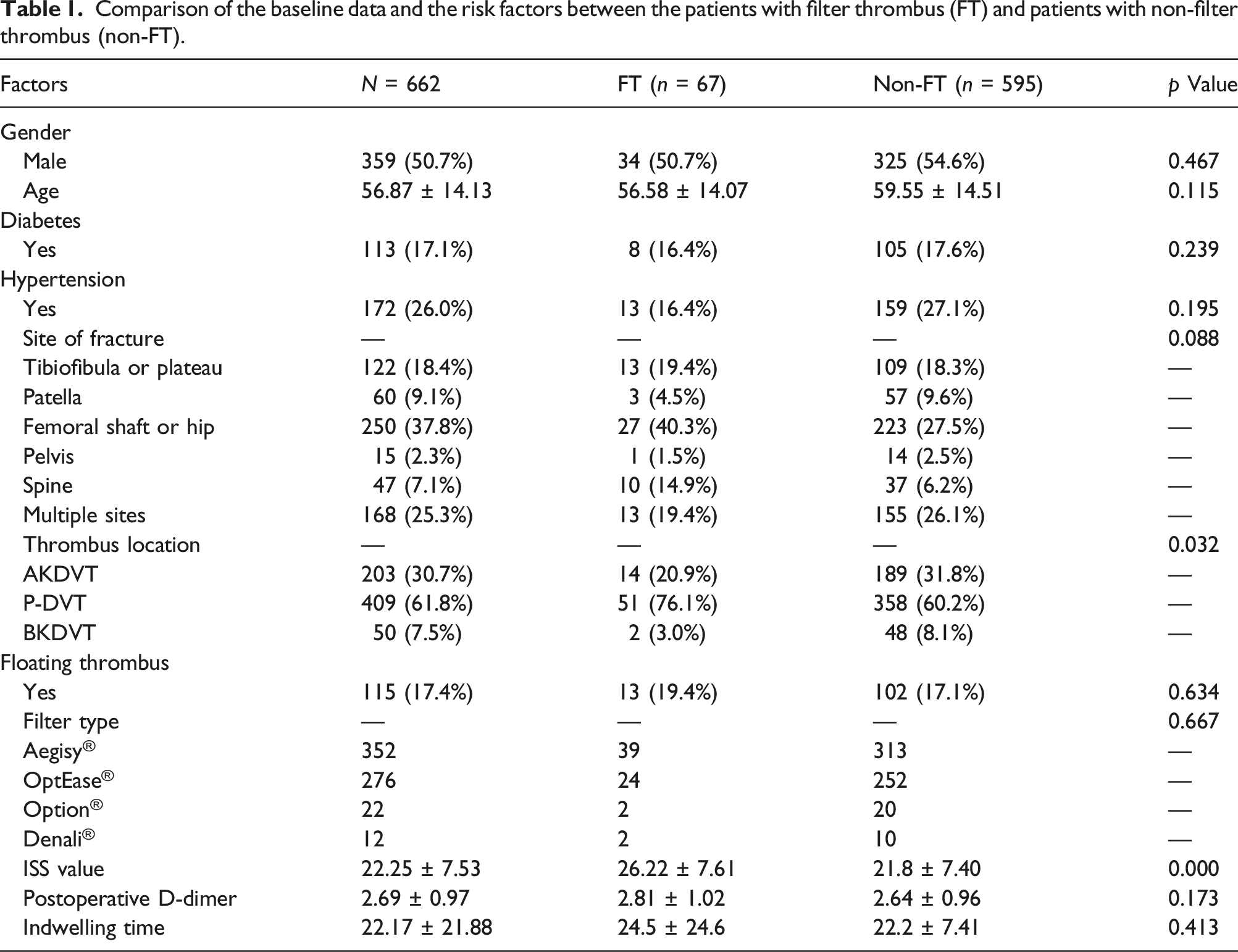
Comparison of the baseline data and the risk factors between the patients with filter thrombus (FT) and patients with non-filter thrombus (non-FT).
Multivariate logistic regression analysis.
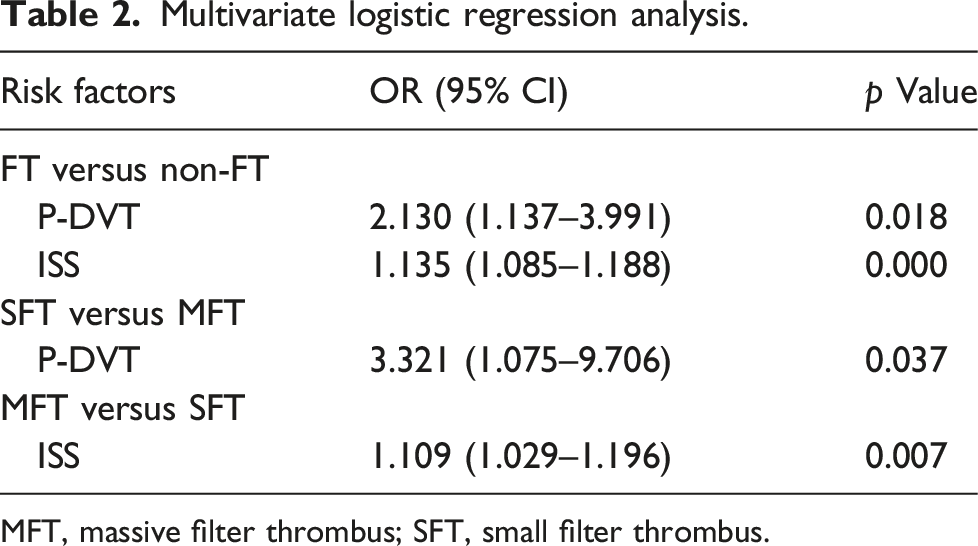
MFT, massive filter thrombus; SFT, small filter thrombus.
Receiver operating characteristic cure analyses of ISS.

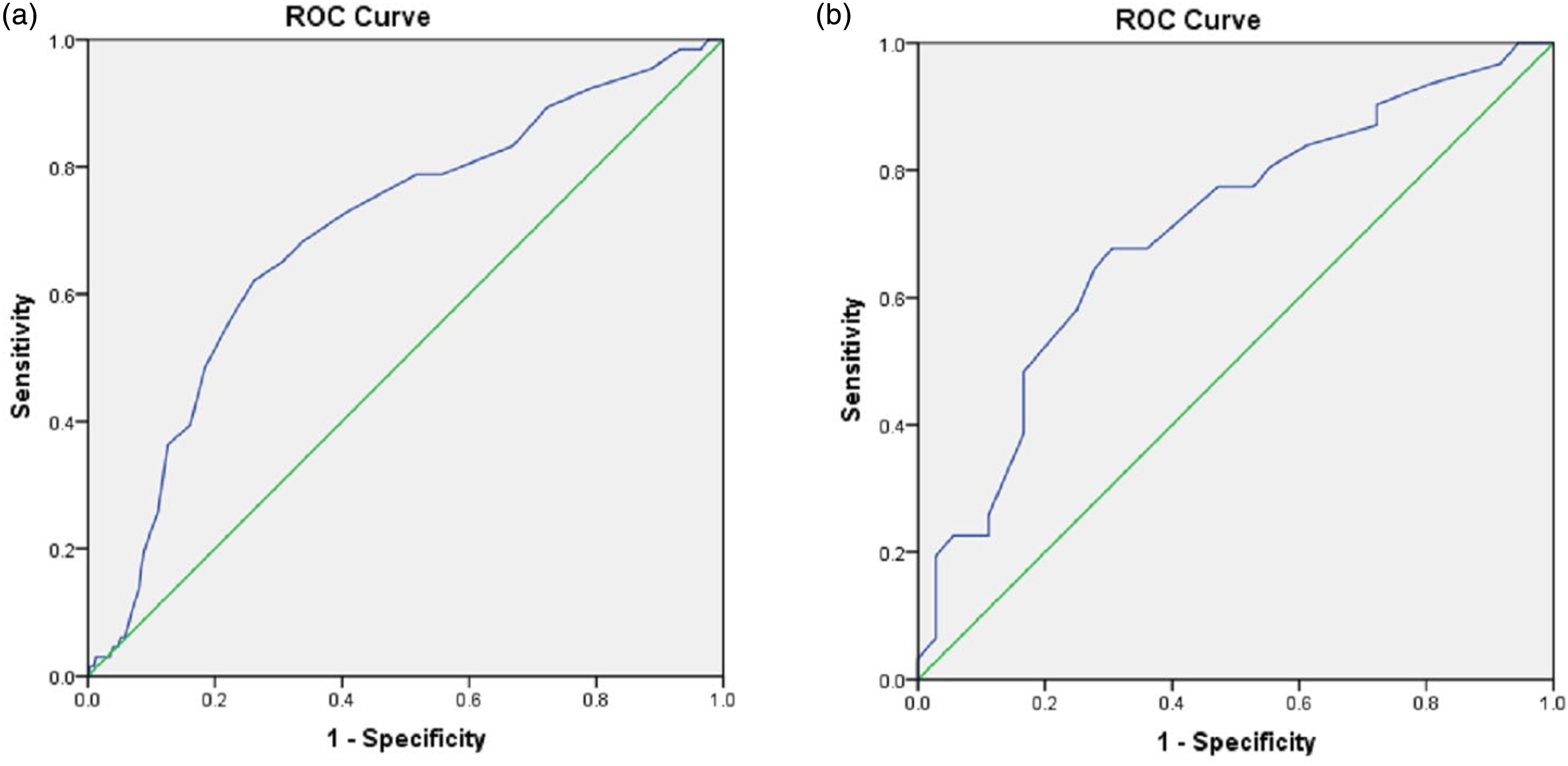
(a) the ROC curve analysis of ISS for filter thrombosis; (b) the the ROC curve analysis of ISS for massive filter thrombosis.
P-DVT was an independent risk factor for filter thrombus with or without calf vein thrombosis. As described above, the filter thrombus group was divided into two depending on thrombus size. Chi-square analysis for ISS indicated significant differences in thrombus size among patients with different thrombus sites (p = 0.041, χ2 = 6.37). Similarly, t-test analysis showed that the ISS was significantly correlated with thrombus size (24.5 ± 6.79 for the small filter thrombus group vs. 29.9 ± 7.77 for the massive filter thrombus group) (T = 3.035, p = 0.003). Multivariable logistic regression analysis showed that P-DVT had a higher potential to lead to a small filter thrombus when compared with AKDVT (OR: 3.231; 95% CI: 1.075–9.706, p = 0.037) (Table 2). ISS was considered a significant predictor for massive filter thrombus (OR: 1.109; 95% CI: 1.029–1.196, p = 0.007). The ROC curve analysis showed that the optimal cutoff value of ISS was 26.5 for diagnosing massive filter thrombus. The AUC of ISS was 0.707 (95% CI: 0.518–0.832, p = 0.004), with a sensitivity of 0.677 and specificity of 0.639 (Table 3 and Figure 3(b)).
Discussion
According to Virchow’s triad, DVT can occur quickly in orthopedic trauma patients due to hypercoagulability, immobilization, and endothelial injury.19,20 The incidence of filter thrombus ranges from 18.6% to 30%, depending on the filter category, study population, anticoagulation therapy, indwelling time, and follow-up time.21–23 In our study, we observed a filter thrombus incidence of 10.1% in all patients receiving anticoagulation therapy, which may have accounted for this. In contrast, some studies24,25 have shown that patients with IVCF on anticoagulation have equivalent rates of thrombotic events compared to patients without anticoagulation. Therefore, whether anticoagulants could significantly decrease the incidence of filter thrombi remains elusive.
Thrombosis progression, IVCF design, filters with short indwelling time, and contraindications for anticoagulation are considered risk factors for thrombosis in a filter.21,26–28 However, little research has been conducted on risk factors such as fracture site, ISS, thrombus location, D-dimer levels, and floating thrombus. In our study, we observed that the spine fracture group had the highest IVCF thrombus rate (21.2%); conversely, the multivariate logistic analysis indicated that the fracture site was not an independent risk factor. The OptEase filter with a shorter dwell time is notorious for filter-related complications, including caval thrombosis. A few reports on OptEase filters showed a rate of up to 9%–25% of thrombi within the filter,22,29 higher than the series with longer dwell times. The lower incidence of trapped clots after a longer dwell time was explained by the dissolution of the clot over time, particularly in patients receiving anticoagulants. 11 Our data showed an occurrence rate of 10% (63/628) for filters with longer dwell times and 11.7% (4/34) for filters with shorter dwell times, suggesting that the type of filter is not a risk factor for filter thrombosis. Therefore, further studies are required to investigate the effect of filter type on filter thrombosis.
The risk factors for associated VTE have also increased with the increased ISS in trauma patients. Hereford et al. reported that for patients with head, neck, chest, and limb trauma, the probability of VTE significantly increased if the ISS was > 12. 30 Chu et al. also reported that the risk of VTE in severe trauma patients with an ISS >15 was six times higher than in patients with mild trauma with an ISS of ≤15. 31 One reason for this phenomenon is that these groups of patients often do not receive immediate DVT prophylaxis until their injuries are stabilized, owing to the risks of excessive blood loss. 30 Moreover, blood transfusion is a significant risk factor for VTE. 32 Inflammation plays an essential role in DVT. Higher ISS, a marker of more severe inflammation, is also related to VTE development. 33 According to our data, ISS significantly differed between the filter thrombus and non-filter thrombus groups and between the small and massive filter thrombus groups. After ROC analysis, when ISS was >26.5, patients were prone to a massive filter thrombus. However, another study found that ISS did not have a predictive value for the possible presence of thrombus within the filter in patients with a mean ISS of 33.1. 22 Therefore, further studies are required to investigate the influence of the ISS.
Proximal DVT (the highest thrombus extent in the popliteal vein or proximally) is associated with an increased risk of symptomatic PE. In a prospective study of 1149 patients 34 and a prospective, multicenter study of 387 patients 35 diagnosed with acute symptomatic DVT, patients with iliofemoral DVT had poor clinical outcomes, such as higher recurrent VTE and higher severity of postthrombotic syndrome. There is no consensus regarding the relationship between proximal DVT and filter thrombosis. We demonstrated that the incidence of filter thrombus in the P-DVT combined with calf DVT group was higher than that in the AKDVT group. In addition, P-DVT is an independent risk factor correlated with small filter thrombi. We hypothesized that this might be related to knee mobility or possible passive activity during the surgery.
Our data showed that IVCF implantation is required for traumatic fracture patients with P-DVT and/or ISS >24.5 before orthopedic surgery. However, without a contraindication for anticoagulation or recurrent PE, the systematic use of IVCFs in the general population with VTE is not recommended, as indicated in the clinical practice guidelines of the American College of Radiology, 36 American College of Chest Physicians, 17 and European Society of Cardiology. 37 Indeed, the necessity of filter implantation for traumatic fracture patients with P-DVT and/or ISS >24.5 should be carefully evaluated, especially for patients with ISS >26.5.
Our study concluded that higher ISS and P-DVT combined with or without calf DVT are potential risk factors for IVCF thrombosis in patients with traumatic fractures. We suggest that orthopedic and vascular physicians should pay more attention to the patients with ISS >24.5 and/or P-DVT combined with or without calf DVT. In addition, for patients with P-DVT combined with or without calf DVT, the physicians should reduce the passive knee flexion and extension as much as possible. Lastly, some methods should be used to control the inflammation of severe traumatic patients (ISS >24.5), such as medicine therapy, early operation, and nutrition support therapy. This study had some limitations. First, other potential risk factors for filter thrombus, including lower limb immobility, contraindication for anticoagulation, personal or family history of VTE, body mass index, perioperative blood pressure and glucose levels, and wound infection, were not discussed. Second, blood loss and transfusion in the patients were not recorded in detail. Lastly, we had a small sample size, which may have led to reporting bias.
Conclusions
Patients with trauma should be monitored for filter thrombosis after filter placement. We observed that the thrombus location and ISS were potential risk factors for filter thrombus in patients with traumatic fractures. P-DVT had a higher potential for leading to filter thrombus, and an ISS value >24.5 was considered a significant predictor for a small filter thrombus, ISS >26.5 for a massive filter thrombus. In addition, more attention should be paid to P-DVT, which may shed more easily during perioperative periods compared with iliofemoral vein thrombosis. However, severe thrombi may not occur after IVCF implantation. Patients with ISS values >24.5 should be closely observed to prevent thrombus aggravation. Finally, a color Doppler ultrasound examination of the IVC should be conducted regularly to identify early filter thrombosis.
Footnotes
Acknowledgements
We acknowledge the patients who participated in this study and the staff at our trauma center.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.