
Abstract
Introduction
Low-density lipoprotein cholesterol (LDL) is a known contributing factor to atherosclerotic cardiovascular disease (ASCVD) and a primary therapeutic target for medical management of ASCVD. Non-high-density lipoprotein cholesterol (non-HDL) has recently been identified as a secondary therapeutic target but is not yet widely used in vascular surgery patients. We sought to assess if vascular surgery patients were undertreated per non-HDL therapeutic guidelines.
Methods
This was an observational study that used a single-center database to identify a cohort of adult patients who received care from a vascular surgery provider from 01/2001 to 07/2021. ICD-9/10-CM codes were used to identify patients with a medical history of hyperlipidemia (HLD), coronary artery disease (CAD), cerebrovascular occlusive disease (CVOD), peripheral artery disease (PAD), hypertension (HTN), or diabetes mellitus (DM). Patient smoking status and medications were also identified. Lab values were obtained from the first and last patient encounter within our system. Primary outcomes were serum concentrations of LDL and non-HDL, with therapeutic thresholds defined as 70 mg/dL and 100 mg/dL, respectively.
Results
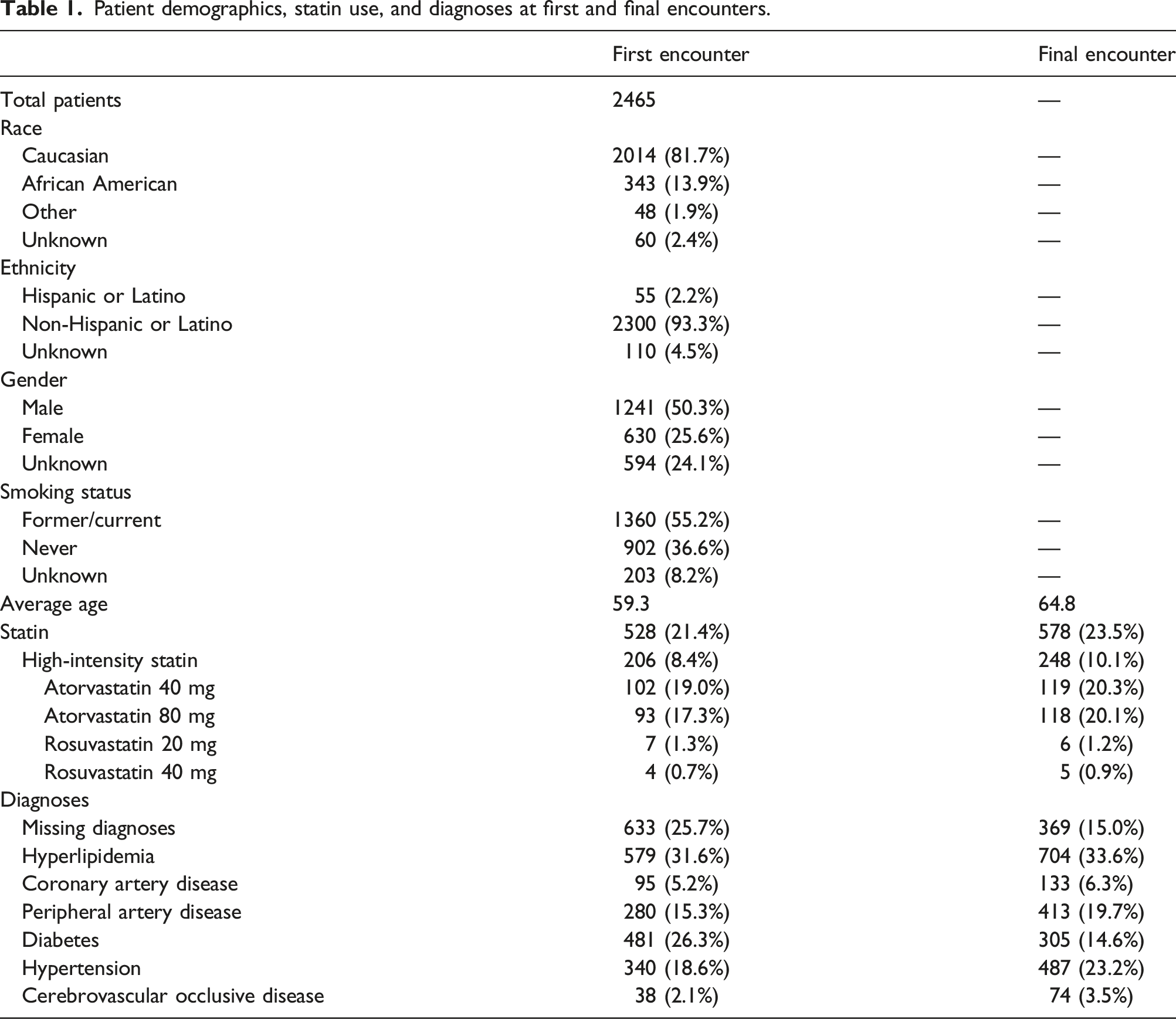
The cohort included 2465 patients. At first encounter, average age was 59.3 years old, 21.4% were on statins, 8.4% were on a high-intensity statin, 25.7% were diagnosed with HLD, 5.2% with CAD, 15.3% with PAD, 26.3% with DM, 18.6% with HTN, and 2.1% with CVOD. At final encounter, mean age was 64.8 years, 23.5% were on statins with 10.1% on high-intensity statin. Diagnoses frequency did not change at final encounter. At first encounter, nearly two-thirds of patients were not at an LDL <70 mg/dL (62.3%) or non-HDL <100 mg/dL (66.0%) with improvement at final encounter to 45.2 and 40.5% of patients not at these LDL or non-HDL treatment thresholds, respectively. Patients on statins exhibited similar trends with 51.1 and 50.1% of patients not at LDL or non-HDL treatment thresholds at first encounter and 39.9 and 35.4% not at LDL or non-HDL treatment thresholds at last encounter. Importantly, 6.9% of patients were at LDL but not non-HDL treatment thresholds.
Discussion
Among vascular surgery patients, over half did not meet non-HDL targets. These results suggest that we may be vastly under-performing adequate medical optimization with only about one-fourth of patients on a statin at their final encounter and approximately one-tenth of patients being treated with a high-intensity statin. With recent evidence supporting non-HDL as a valuable measurement for atherosclerotic risk, there is potential to optimize medical management beyond current high-intensity statin therapy. Further investigation is needed regarding the risk of adverse events between patients treated with these varied therapeutic targets.
Introduction
Atherosclerotic cardiovascular disease (ASCVD) is defined as acute coronary syndrome, myocardial infarction, angina, stroke or transient ischemic attack (TIA) due to cerebrovascular occlusive disease (CVOD), and/or peripheral artery disease (PAD) and is the leading cause of death in the United States.1–3 Atherogenesis is driven by several factors, especially by atherogenic lipoproteins which play fundamental roles in the initiation and evolution of atherosclerosis and ASCVD. 2 Preventive measures via lifestyle modifications and risk factor modification with antiplatelet agents and statin therapy are critical for primary and secondary prevention of ASCVD. 4 Low-density lipoprotein (LDL) cholesterol has historically been the primary medical target for primary and secondary prevention of ASCVD with a target value of less than 100 mg/dL.4–8 However, current guidelines recommend considering ASCVD risk enhancers that include lipid and biomarkers such as elevated triglycerides rather than targeting specific LDL values alone.5,9,10 Moreover, a growing body of literature has highlighted the importance of measuring and modifying other components of the lipid profile that may provide more accurate risk assessment, chiefly non-high-density lipoprotein (non-HDL) cholesterol and apolipoprotein B (Apo B).11–14
Non-HDL defines the cholesterol content of all atherogenic lipoproteins and can be measured by subtracting the HDL from the total cholesterol (TC). 15 Non-HDL is a better marker for risk of coronary artery disease and is more closely associated with coronary atheroma progression than LDL.12,15,16 Furthermore, non-HDL has been shown to be a reliable predictor of adverse cardiovascular outcomes amongst patients on lipid-lowering therapy and to be as good or better than LDL in predicting ASCVD risk.17,18 Non-HDL has been shown to be independently associated with both CVOD and PAD.19–22 In fact, non-HDL has been added as secondary treatment target in patients with elevated triglycerides with a treatment threshold value of non-HDL 30 mg/dL above the LDL treatment threshold (i.e., non-HDL threshold of 100 mg/dL when the guideline-defined LDL threshold is 70 mg/dL).4,22–25
Despite its association with PAD and CVOD, non-HDL is still not routinely used as a treatment target nor risk predictor in vascular surgery patients, who are in general high risk for ASCVD. High-intensity statins remain the mainstay of treatment for vascular surgery patients with PAD and/or CVOD with current treatment thresholds remaining unclear.4,24–26 It is unclear how many vascular surgery patients have elevated non-HDL and thus may not be medically optimized and/or undertreated with statin therapy. Thus, we studied this high-risk population of vascular surgery patients to examine frequency of elevated non-HDL levels in addition to those who are not at proposed LDL and/or non-HDL treatment thresholds. In addition, we aimed to investigate whether patients with elevated non-HDL levels had higher proportions of PAD and/or CVOD.
Methods
This study was an observational cohort study of adults treated by a vascular surgery provider at the University of Michigan (U-M) from January 2001 to July 2021. Patients were selected from DataDirect, a single-center dataset using diagnosis codes from the International Classification of Disease 9th and 10th edition (ICD9/ICD10). DataDirect is a self-serve tool that enables access to clinical data such as diagnoses, encounters, procedures, medications, and labs from more than four million surgical patients from across the U-M Health System. The Institutional Review Board at University of Michigan approved this study and determined that informed consent was waived since it was a secondary analysis of a de-identified database.
Study population
The study population consisted of adult surgery patients and/or recipients of anesthesia who received care at the U-M in an inpatient and/or outpatient setting from a vascular surgery provider from 01/2001 to 07/2021. DataDirect catalogs information from all surgery patients and/or recipients of anesthesia. Patients were not included or excluded based on surgical procedures or providers but rather included on inpatient and/or outpatient encounters with vascular surgery providers. Patients were included if they had laboratory values and/or medication information in the database. Patient encounters were included if they were associated with lipid focused lab values: Triglycerides (TG), HDL, LDL, non-HDL, or TC. First encounter was defined as the first inpatient or outpatient encounter with a vascular surgery provider that was associated with lipid focused labs, and last encounter was defined as the last inpatient or outpatient encounter by a vascular surgery provider associated with lipid labs. Patients without more than one encounter associated with lipid-focused labs were excluded (Figure 1). ICD9/ICD10 codes were used to identify diagnosis of hyperlipidemia (HLD), CAD, CVOD, PAD, hypertension (HTN), and/or diabetes mellitus (DM) (Supplemental Table 1). General demographic information, statin usage, and lipid-focused lab values were collected. LDL is calculated at the U-M using the Friedewald equation.
27
We also calculated LDL using the Sampson
28
and the Martin-Hopkins equations.
29
Non-HDL was calculated using total cholesterol minus HDL cholesterol. Adult surgical patients seen by a vascular surgery provider at the University of Michigan between 2001 and 2021 were identified. Patients were included if they had patient encounters that were associated with medications, diagnoses, and lipid-focused laboratory values (TG, HDL, LDL, non-HDL, and/or TC). Patients were included if they have lipid-focused lab values at more than one patient encounter.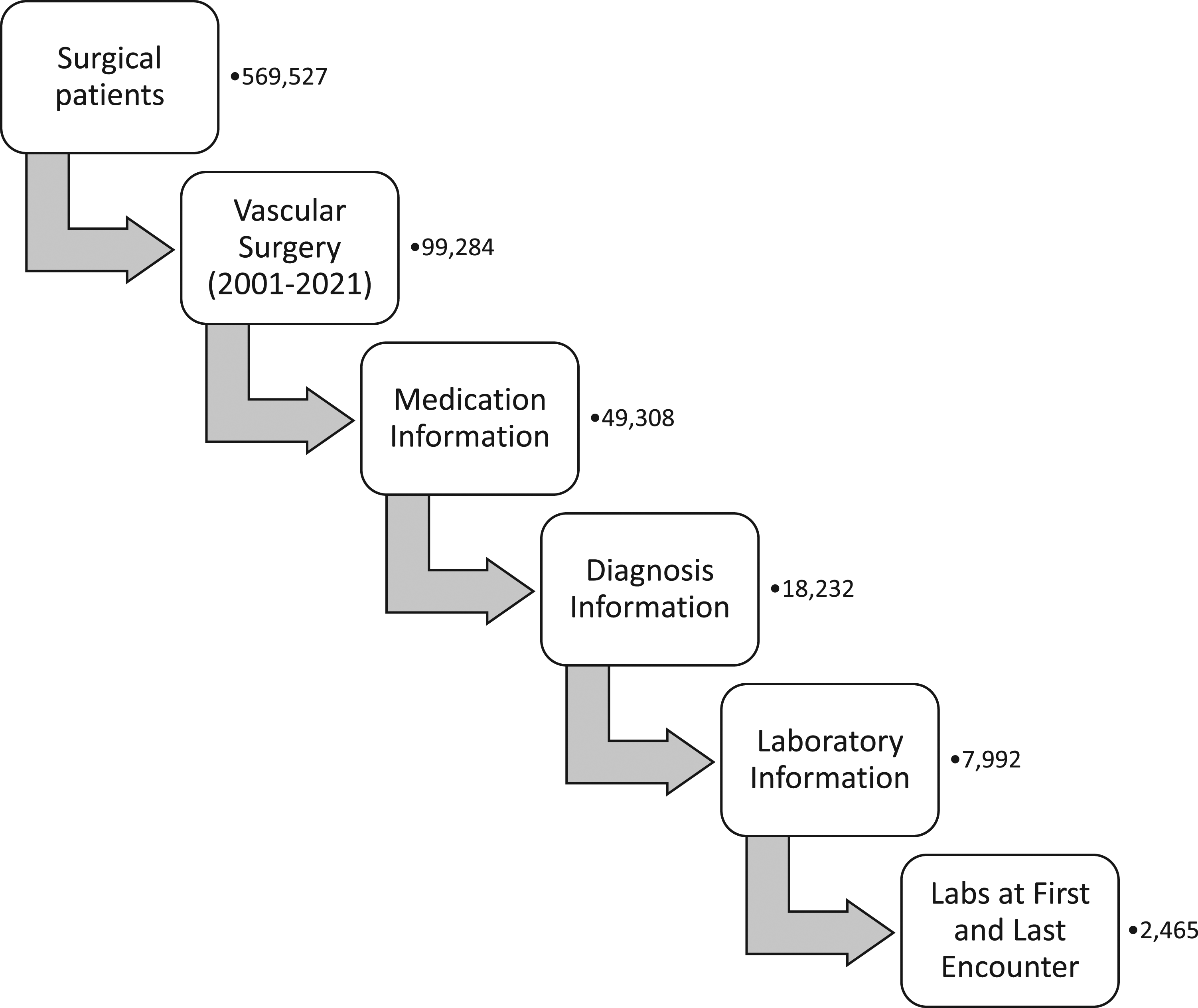
Data analysis
Diagnoses and lab values were assessed at the patients’ first encounter and last encounter and at any encounter within the database. The first encounter was defined as the earliest patient encounter that was associated with laboratory measurements of triglycerides, HDL, LDL, non-HDL, and/or TC while the last encounter was defined as the latest patient encounter associated with the above laboratory measurements. We first assessed average age, statin use, and encounter diagnoses between first and last patient encounters. Statin use was defined as documentation of any medication within the statin class during an encounter. Encounter diagnoses were defined using the aforementioned IDC9/ICD10 codes. We then compared the aforementioned lipid-focused lab values and diagnoses between first and last encounter. Primary outcomes were serum concentrations of LDL (calculated via the Friedewald equation) and non-HDL, with therapeutic thresholds of 70 mg/dL and 100 mg/dL, respectively. Additionally, patients were divided into cohorts based on their LDL (calculated via the Friedewald, Sampson, and Martin-Hopkins equations) and non-HDL lab values and therapeutic thresholds (LDL < or ≥70 mg/dL, non-HDL < or ≥100 mg/dL, LDL <70 mg/dL and non-HDL <100 mg/dL, and LDL <70 mg/dL but non-HDL >100 mg/dL). We then compared encounter diagnoses at last patient encounter for patients who were within these therapeutic thresholds.
Statistical analysis was done with Stata (StataCorp, College Station, TX). Paired student’s T test was used to compare average lab values and numerical data between groups. Chi squared analysis was used to compare average diagnoses and categorical data between patient cohorts.
Results
Patient demographics, statin use, and diagnoses at first and final encounters.
Patients treated with and without statins.
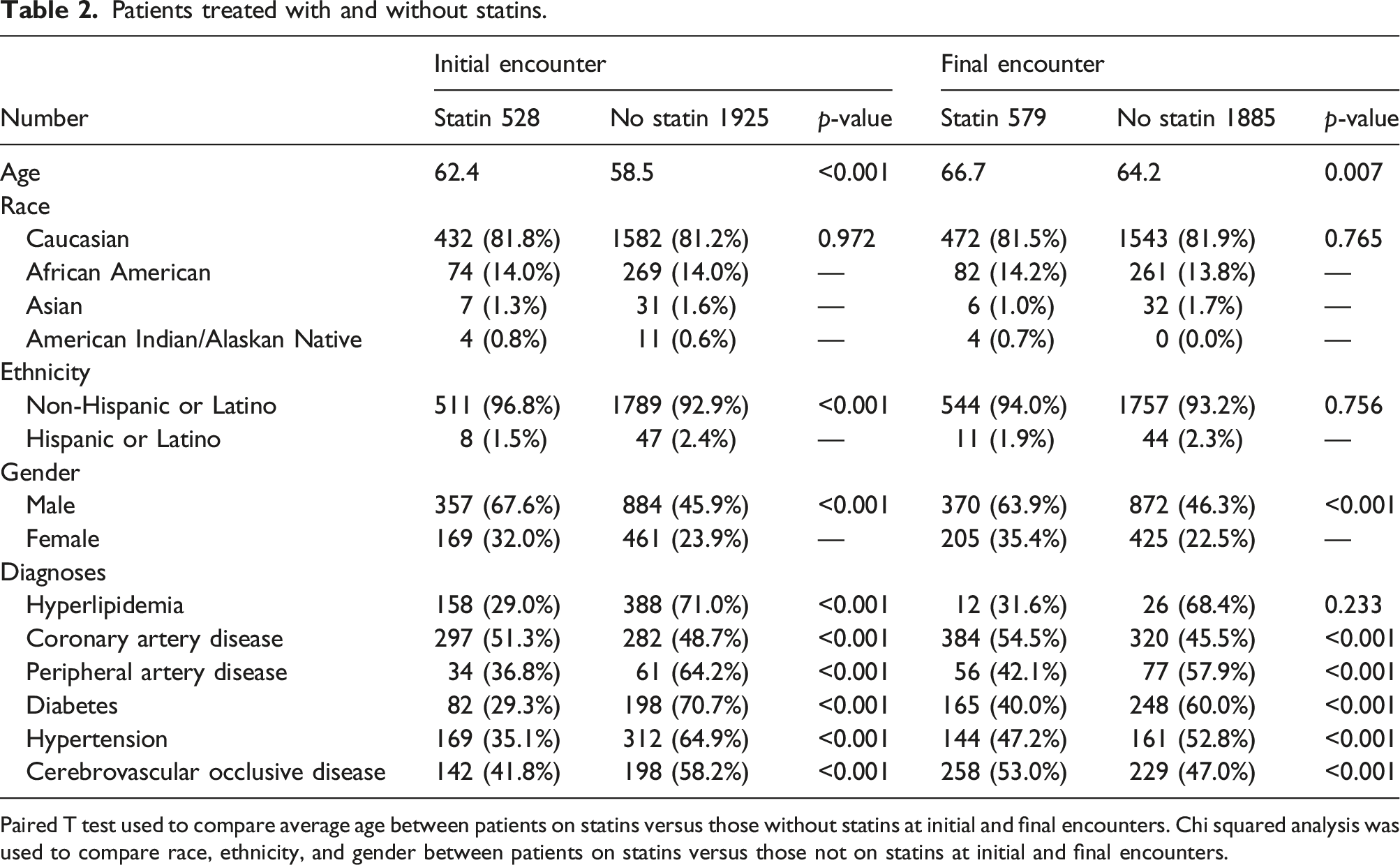
Paired T test used to compare average age between patients on statins versus those without statins at initial and final encounters. Chi squared analysis was used to compare race, ethnicity, and gender between patients on statins versus those not on statins at initial and final encounters.
Patient lab values at initial and final encounters.
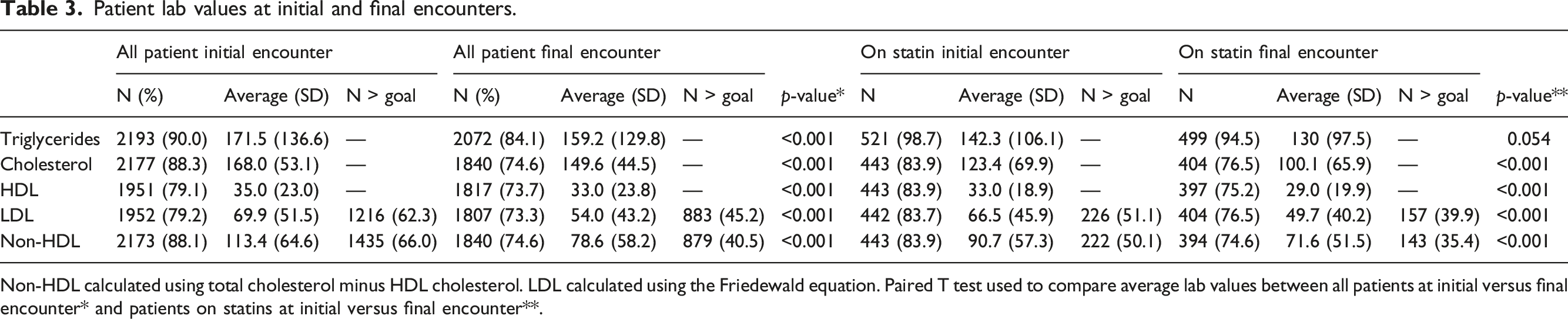
Non-HDL calculated using total cholesterol minus HDL cholesterol. LDL calculated using the Friedewald equation. Paired T test used to compare average lab values between all patients at initial versus final encounter* and patients on statins at initial versus final encounter**.
Diagnosis codes for patients based on non-HDL and LDL values.
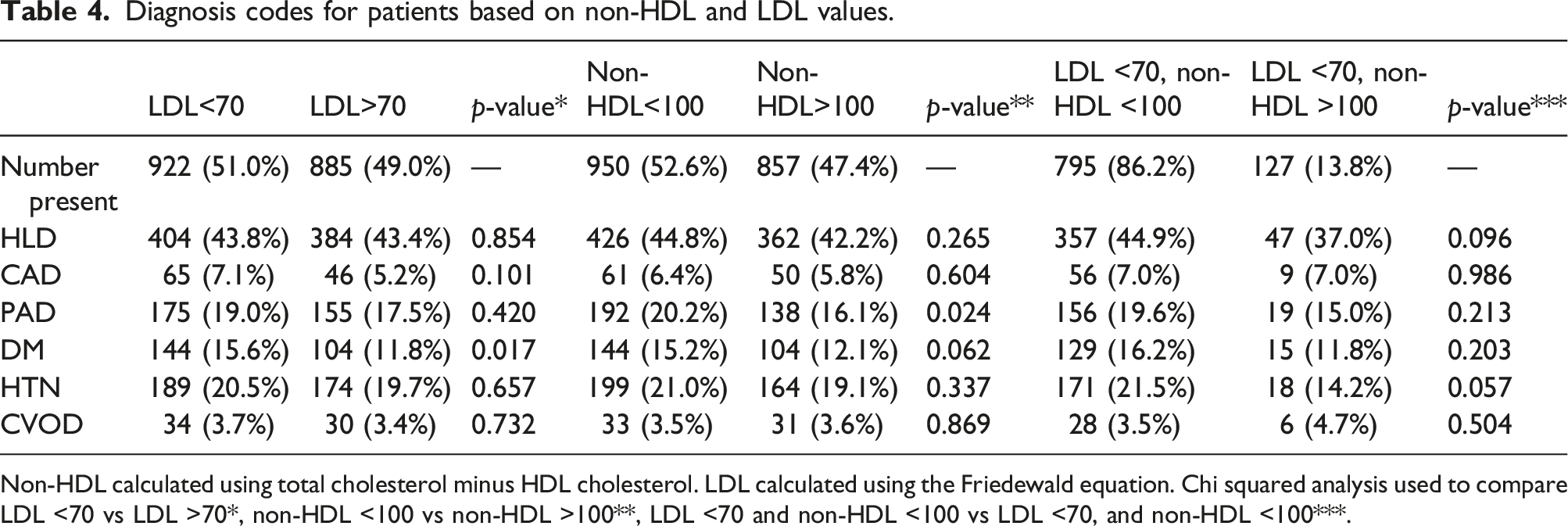
Non-HDL calculated using total cholesterol minus HDL cholesterol. LDL calculated using the Friedewald equation. Chi squared analysis used to compare LDL <70 vs LDL >70*, non-HDL <100 vs non-HDL >100**, LDL <70 and non-HDL <100 vs LDL <70, and non-HDL <100***.
Comparison of patient diagnoses between different LDL cholesterol calculations.
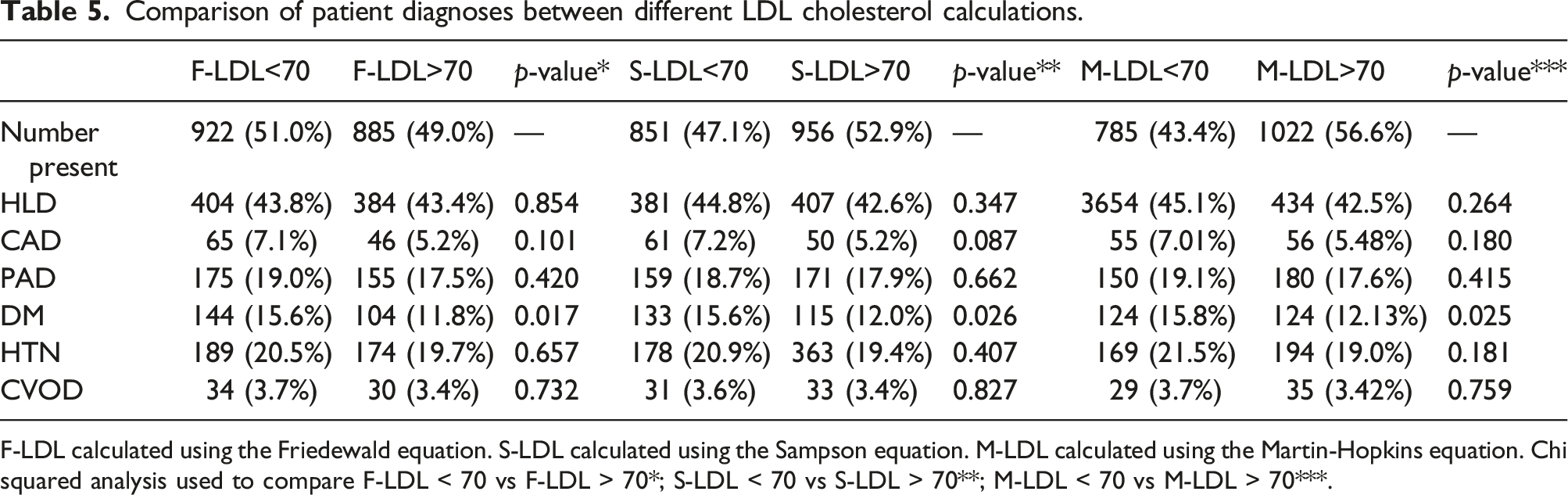
F-LDL calculated using the Friedewald equation. S-LDL calculated using the Sampson equation. M-LDL calculated using the Martin-Hopkins equation. Chi squared analysis used to compare F-LDL < 70 vs F-LDL > 70*; S-LDL < 70 vs S-LDL > 70**; M-LDL < 70 vs M-LDL > 70***.
Comparison of patient diagnoses between different LDL cholesterol calculations and non-HDL values.
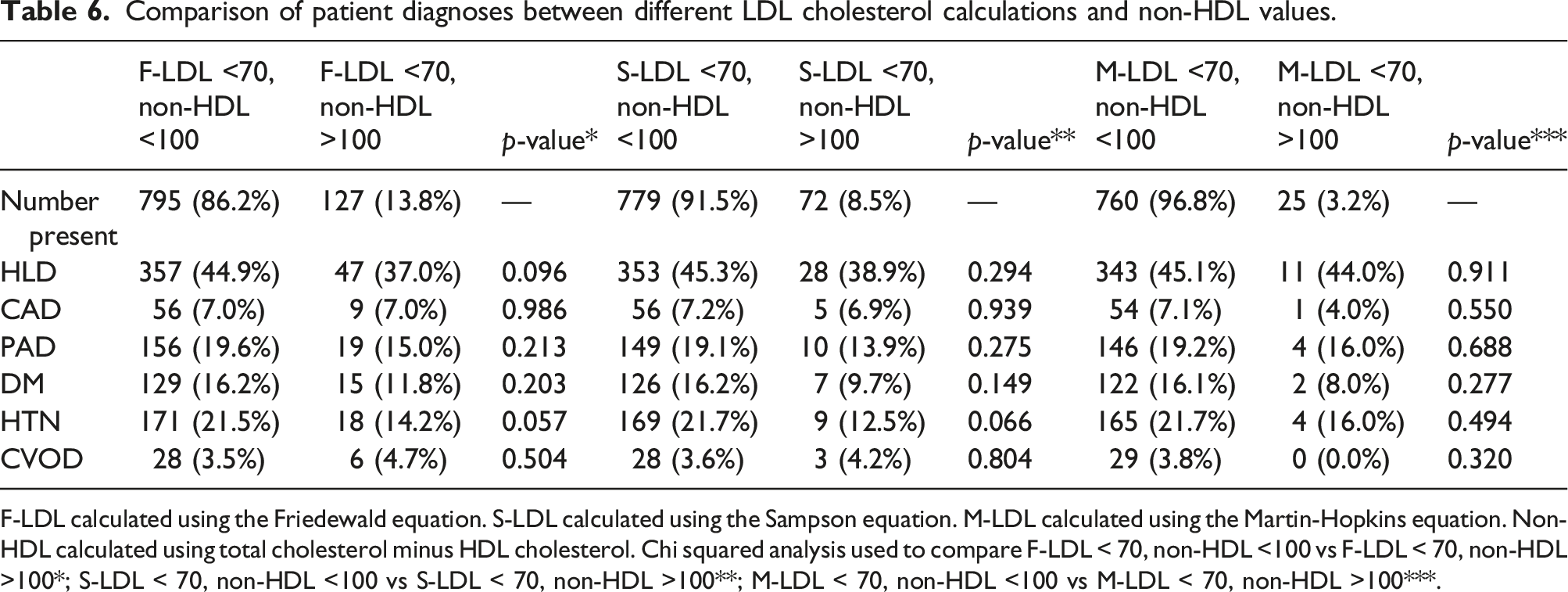
F-LDL calculated using the Friedewald equation. S-LDL calculated using the Sampson equation. M-LDL calculated using the Martin-Hopkins equation. Non-HDL calculated using total cholesterol minus HDL cholesterol. Chi squared analysis used to compare F-LDL < 70, non-HDL <100 vs F-LDL < 70, non-HDL >100*; S-LDL < 70, non-HDL <100 vs S-LDL < 70, non-HDL >100**; M-LDL < 70, non-HDL <100 vs M-LDL < 70, non-HDL >100***.
Discussion
In the present study, we demonstrate that among vascular surgery patients, approximately two-thirds were not at a treatment target of LDL <70 md/dL or non-HDL of <100 mg/dL at their first encounter. Patients remained undertreated with approximately half of patients not at or below LDL or non-HDL thresholds at their final encounter. Current guidelines for PAD and CVOD recommend patients to be on statin therapy with lipid-lowering targets as a secondary treatment threshold. Our results demonstrate that we may be vastly under-performing proper medical optimization with only about one-fourth of patients on a statin at their final encounter and approximately one-tenth of patients being treated with a high-intensity statin. The present study highlights the fact that vascular surgery patients, who are often at high risk for ASCVD, may be significantly undertreated and are not currently being optimized at current guideline thresholds.
Non-HDL has been proposed as a more reliable measurement than LDL because it accounts for all atherogenic lipoproteins, whereas LDL is indirectly estimated as a function of TG, HDL, and TC, most often via the Friedewald equation. 27 Measurement of TG have been plagued by a high degree of variability even in the fasting state. 30 Non-HDL can be measured on a non-fasting patient and easily calculated from a lipid profile without the use of TG and thus is less subject to error induced by high TG in a non-fasting state. 11 Furthermore, non-HDL is a better predictor of adverse cardiovascular outcomes amongst patients on lipid-lowering therapy than LDL.14,15 Thus, non-HDL remains a promising adjunct for ASCVD risk stratification and appears to be more reliable and accurate than LDL. In our study, using different LDL equations (Friedewald, Sampson, and Martin-Hopkins) lead to differences in the percentage of patients who were at LDL <70 mg/dL and non-HDL <100 mg/dL, with the Martin-Hopkins equation demonstrating the highest congruence of patients at both LDL and non-HDL goals (96.8%). These results support that non-HDL may be a more reliable measure and demonstrate that the use of the Friedewald equation performs the worst. Given the differences seen between LDL equations, there is potential to optimize medical management beyond current high-intensity statin therapy using non-HDL as a treatment marker. However, further investigation is needed to determine the association of non-HDL cholesterol with disease burden and post-operative outcomes.
When comparing patients who were above and below LDL of 70 mg/dL and those above and below non-HDL of 100 mg/dL, there was no difference in patient diagnoses of CAD, HTN, or CVOD at their final encounter. Interestingly, patients with LDL >70 mg/dL had lower amount of DM diagnoses and patients with non-HDL >100 mg/dL had a lower amount of HLD and PAD diagnoses. These findings were irrespective of LDL calculation (Friedewald, Sampson, and Martin-Hopkins). However, these findings were conducted with a univariate analysis and thus are limited given that we did not account for other factors that could contribute to diagnoses such as CAD, HTN, DM, PAD, and CVOD. The former could possibly be explained by metabolic derangements leading to higher TG, thus erroneously calculating lower LDL by the Friedewald equation. However, our sensitivity analysis did not confirm this to be the case. Although these results seemingly support that lipid-based treatment thresholds do not improve outcomes, our dataset is limited and not appropriate to answer this question. On the contrary, we feel it informs on the high-risk nature of patients being referred to vascular surgery.
In our study, patients who were on statins demonstrated a significant decrease in their non-HDL and LDL when comparing initial and final encounters. Moreover, patients treated with statins had more patients at LDL and non-HDL treatment thresholds. Although this dataset included patients seen by vascular surgery providers, a majority of medical management is oftentimes multi-disciplinary with many patients being managed by cardiology, vascular medicine, and primary care. Regular dose titration to LDL of <70 mg/dL is not routinely done by vascular surgeons; our results support that statin therapy is an effective means of lipid lowering and risk reduction via secondary treatment thresholds. However, our findings highlight that there is significant room for improvement in the medical optimization of vascular surgery patients. Moreover, our results highlight potential under-prescribing of statins to patients with peripheral vascular and cerebrovascular disease given the higher rates of statin usage in patients with CAD when compared to PAD and CVOD. Given the astoundingly low percentage of patients on statins, improved methods of identifying patients not optimally managed medically are warranted. A multi-modal approach including vascular surgeons, cardiovascular medicine, and primary care providers is needed to ensure adequate lipid-lowering treatment of vascular surgery patients. Vascular surgery providers must place increasing emphasis on ensuring their patients are treated appropriately with statin therapy through improved communication with primary care providers and increased prescribing of statin therapy when indicated.
Interestingly, there was decrease in HDL between first and final encounters for all patients and those on statins, which could be explained via a few mechanisms which were not captured in our database. Given that inactivity has been demonstrated to be suggested to be a cause of lower HDL, vascular surgery patients with progressive disease and those undergoing surgical interventions may have become less active over time thus contributing to a decrease in HDL.31,32 Additionally, numerous cardiovascular medications, antipsychotics, anticonvulsants, hormones, and certain immunosuppressives have been demonstrated to have a negative impact on lipid profiles. 33 Some medications demonstrate a class effect while others are dose dependent and drug specific. 33 Nonetheless, these were not accounted for in our dataset.
This study was a single-center retrospective study and thus has limitations that must be kept in mind. Although the U-M has a large patient catchment area, the pre-dominant vascular surgery patients are non-Hispanic white males which was reflected in our cohort. Vascular disease affects all races and genders, and thus, our results may not be completely generalizable to the entire population. Furthermore, our study depicts only medication trends from a single center rather than nationwide. Given that LDL and cholesterol treatment guidelines have changed over time with previous recommendations of LDL values <100 mg/dL, patients who were seen and managed earlier in the cohort may have been at their treatment goal based on recommendations at that time. 8 Our study relied on ICD9/ICD10 codes which may vary between institutions nationally and hospital coders at a single institution and do not include quantifiable or robust information about disease burden. Retrospective studies are subject to limitations associated with data from the electronic health record including missing data, such as laboratory values performed at other institutions. If a diagnosis and/or medication was not associated with an encounter, then it would not have been captured in our study and thus could impact our results. Additionally, the diagnoses evaluated in this study are not equivalent to each other and are not indications alone for statin usage, but rather strong risk factors for poor outcomes and a major component of risk estimation equations. Diagnoses evaluated in this study are chronic and thus would likely not change between patient encounters. Furthermore, our study did not assess for other lipid-modifying treatment modalities such as lifestyle modifications, PCSK9 inhibitors, bile acid sequestrants, or fibrates. Given that our dataset consisted of outpatient and inpatient encounters, we cannot ensure that all lipid panels were obtained in the fasting state which could have affected that accuracy of our results. Future studies are needed to elucidate the association of non-HDL levels on disease burden and patient outcomes.
Conclusion
In our study, only one-fourth of statin-eligible vascular surgery patients were treated with statin therapy. Furthermore, approximately half of patients seen by vascular surgery were not at secondary treatment threshold with elevated LDL and non-HDL at their initial and final encounters. These results highlight that vascular surgery patients may be undertreated and not medically optimized. There is significant room for improvement in medical therapy for vascular surgery patients. A multi-disciplinary approach from vascular surgery, cardiovascular, and general medical providers is needed to increase statin usage in patients with PAD and/or CVOD. Further research is needed to identify provider and patient barriers for statin usage and optimal medical therapy. Non-HDL is a promising adjunct for ASCVD risk stratification and serves as a secondary treatment target for further medical optimization. However, future studies are needed to explore the association of non-HDL cholesterol with atherosclerotic disease burden and post-operative outcomes among vascular surgery patients.
Supplemental Material
Supplemental Material - Non-High density lipoprotein cholesterol and treatment targets in vascular surgery patients
Supplemental Material for Non-High density lipoprotein cholesterol and treatment targets in vascular surgery patients by Drew J Braet, Kian Pourak, Vibav Mouli, Itai Palmon, Dan Dinh, Nicholas H Osborne, Chandu Vemuri and Eric J Brandt in Vascular
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.