
Abstract
Objective
Whether socioeconomic status (SES) is associated with health outcomes in patients with acute limb ischemia (ALI) is largely unknown. We aimed to determine whether SES is associated with worse presentations and outcomes for patients with ALI.
Methods
We performed a retrospective medical record review of patients who presented with ALI between April 2016 and October 2020 at a single tertiary care center. SES was quantified using individual variables (median household income, level of education, and employment) and a composite endpoint, the neighborhood deprivation index (NDI). The NDI is a standardized and reproducible index that uses census tract data (higher number indicates lower SES status). The NDI summarizes 8 domains of socioeconomic deprivation. ALI severity was categorized using the Rutherford classification. The association between SES and the severity of ALI at presentation and between SES and other health outcomes were analyzed using bivariate analysis of variance, independent t test, and multivariate logistic regression.
Results
During the study period, 278 patients were treated for ALI, of whom 211 had complete SES data available. The mean age was 64 years, 55% were men, and 57% were White. The Rutherford classification of disease severity was grade 1, 2a, 2b, and 3 for 6%, 54%, 32%, and 8% of patients, respectively. Patients with a low SES status per the NDI were more likely to have a history of peripheral arterial disease and chronic kidney disease at presentation. The ALI etiology (thrombotic vs embolic) was not associated with SES. No significant differences were seen between SES and the severity of ALI at presentation (p = 0.96) or the treatment modality (p = 0.80). No associations between SES and 30-day or 1-year mortality were observed (mean NDI, 0.15 vs 0.26, p = 0.58, and 0.20 vs 0.26, p = 0.71, respectively) or between SES and 30-day or 1-year limb loss (mean NDI, 0.06 vs 0.30, p = 0.18, and 0.1 vs 0.32, p = 0.17, respectively). Lower SES (higher NDI) was associated with increased 30-day readmission (mean NDI, 0.49 vs 0.15, p = 0.021). However, this association was not significant on multivariate analysis (odds ratio 1.4, 95% CI 0.9–2.1, p = 0.06).
Conclusions
SES was not associated with the severity of ALI at patient presentation. Although SES was associated with the presence of peripheral arterial disease and chronic kidney disease at presentation, SES was not a predictor of short-term or 1-year limb loss and mortality. Overall, ALI presentation and treatment outcomes were independent of SES.
Keywords
Introduction
The incidence of acute limb ischemia (ALI) is reported to be around 1.5 cases out of 10,000 people per year. 1 ALI is a highly morbid condition that often leads to major in-hospital adverse events such as exacerbation of congestive heart failure, myocardial infarction, deterioration in renal function, and respiratory complications. 2 Despite the practice of providing early revascularization for patients with ALI, postoperative complications in this population remain high, with 30-day amputation and mortality rates ranging between 10% and 15%.3,4
In 2019, nearly 43 million Americans lived below the poverty line, and 15% of the population lacked health insurance. 5 This problem is amplified in the city of Detroit, which was listed as the second most impoverished big city in the United States in 2020, with 31% of residents living below the poverty line. 5 Low socioeconomic status (SES) has been shown to be associated with higher prevalence of coronary artery disease, hypertension, diabetes, delayed access to health care, decreased access to specialized treatments and procedures, and increased morbidity and mortality in cardiovascular patients.6,7 Recent studies have shown that low SES is associated with increased prevalence of peripheral artery disease (PAD) with an increased risk of amputation in patients with chronic limb threatening ischemia;8,9 however, the association of SES with severity of ALI presentation and outcomes after ALI is poorly defined. The aim of this study was to examine the relationship between SES disparity and of patients who presented with ALI.
Materials and methods
Patients
Registry database medical records for all patients who underwent treatment for ALI at our tertiary referral center between 1 April 2016 and 30 October 2020 were retrospectively queried. The clinical presentation was considered acute if it occurred within 14 days after symptom onset. Physical examination and Doppler signals were used to diagnose ALI. Only patients who had ALI to their lower limbs were included in the study. Patients with missing SES or Rutherford information were excluded.
The present study was reviewed and approved by the Edsel Board Institutional Review Board of the Henry Ford Hospital (No. 12715) and conducted in accordance with the Health Insurance Portability and Accountability Act and the prevailing ethical principles governing research.
Variables
Sociodemographic variables included age, sex, race/ethnicity (African American, Asian, White, and Other), body mass index, and smoking. Race designations were predetermined per the medical record database. Medical history variables included type 2 diabetes, hypertension, coronary artery disease, PAD, hyperlipidemia, congestive heart failure, chronic kidney disease, anemia (defined as hemoglobin <12 g/dL in women and <13 g/dL in men), and previous vascular procedure (carotid, abdominal, or peripheral interventions). Perioperative variables included transfer from another hospital, Rutherford classification, etiology (embolic or thrombotic) and treatment modality received (open, endovascular, medical, or primary amputation).
Endpoints
The primary endpoints were mortality and limb loss at 30 days. Secondary endpoints included 30-day readmission, 1-year mortality and limb loss.
Messer neighborhood deprivation index
SES was measured using the neighborhood deprivation index (NDI). The NDI is a standardized and reproducible index based on the census tract derived from patients’ addresses at the time of surgery. The NDI summarizes 8 socioeconomic variables, including the percentage of households that have the following characteristics: head of household is male with a professional occupation; head of household has less than a high school education; household income is below the 1999 federal poverty level; head of household is a woman with dependent children; head of household is unemployed; household has an annual income of < $30,000; household is considered crowded; and household is on public assistance. The NDI represents 6 social domains: occupation, education, poverty housing, employment, racial composition, and residential stability. After the NDI was calculated for the patients in our cohort, a score ranging from −1.59 to 5.54 was given to each individual. The index was conventionally categorized into tertiles, with the third tertile corresponding to the most socioeconomically deprived. Several studies have used the NDI to study the effect of SES.10-12
Rutherford classification
Categorization of the cohort by Rutherford classification.

Data analysis
To increase interpretability of the models prior to the analyses, SES variables were combined and standardized. Specifically, income-related SES variables were set to present increases of $10,000, and all other SES variables were set to present increases of 10%. Continuous variables were presented as means and standard deviation, while categorical variables were described with frequency and percentages. The association between SES and the severity of ALI at presentation as well as outcomes were analyzed using independent t test, analysis of variance, and multivariate logistic regression, as appropriate. Any variable with a p value <0.1 or thought to be related to the outcome of interest was included in the multivariate analyses. SPSS version 27.0 was used for statistical analysis (IBM, Armonk, NY), and a p value <0.05 was considered statistically significant.
Results
Characteristics of the study cohort
Demographic summary of the cohort.
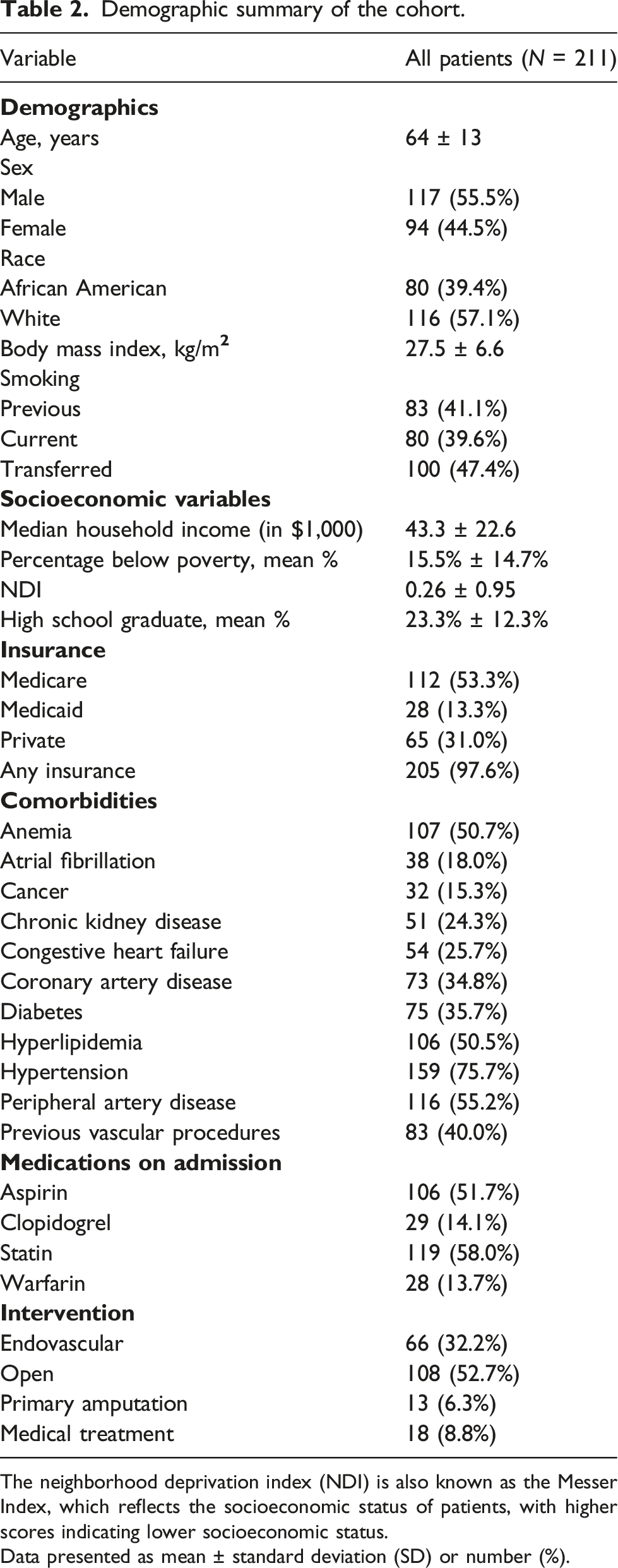
The neighborhood deprivation index (NDI) is also known as the Messer Index, which reflects the socioeconomic status of patients, with higher scores indicating lower socioeconomic status.
Data presented as mean ± standard deviation (SD) or number (%).
Difference in mean NDI among baseline characteristics, comorbidities, and perioperative variables.
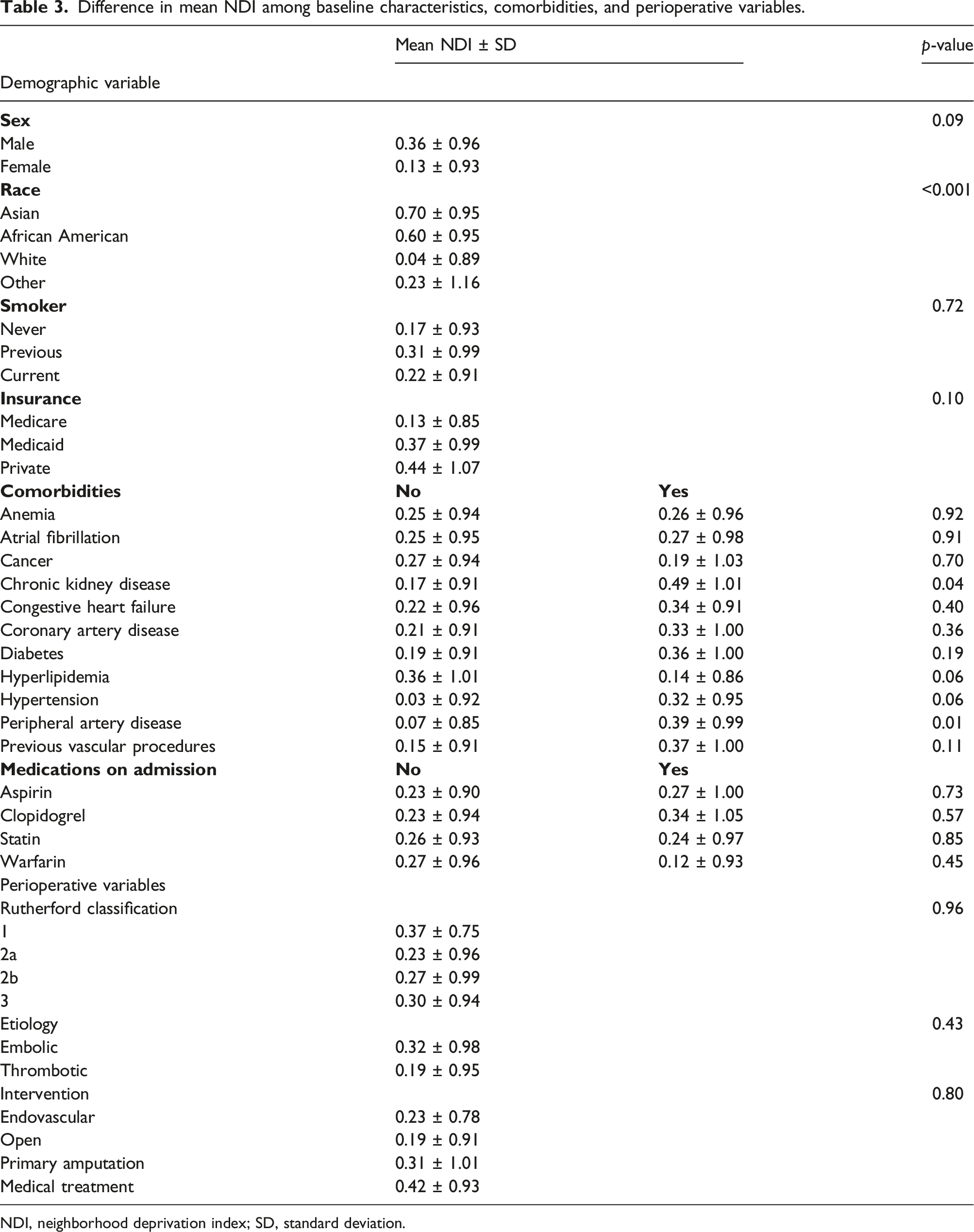
NDI, neighborhood deprivation index; SD, standard deviation.
SES and covariates
The mean NDI did not correlate with sex or smoking status (p = 0.09 and p = 0.72, respectively) (Table 3). No significant difference was seen when comparing the mean NDI and insurance type (p = 0.10). White patients were more likely to have a lower SES, which corresponds to a higher NDI score, than Asian and African American patients (p < 0.001). Patients with lower SES were more likely to have a history of chronic kidney disease (p = 0.04) and PAD (p = 0.01) on presentation. No significant differences were seen in comparisons of mean NDI with other comorbidities, admission medications, severity of ALI on presentation (p = 0.96), ALI etiology (p = 0.43), or the treatment modality received (p = 0.80). No significant difference was seen when comparing distance from the hospital and ALI severity on presentation (p = 0.79).
SES and outcomes
Difference in mean NDI among outcomes of interest.
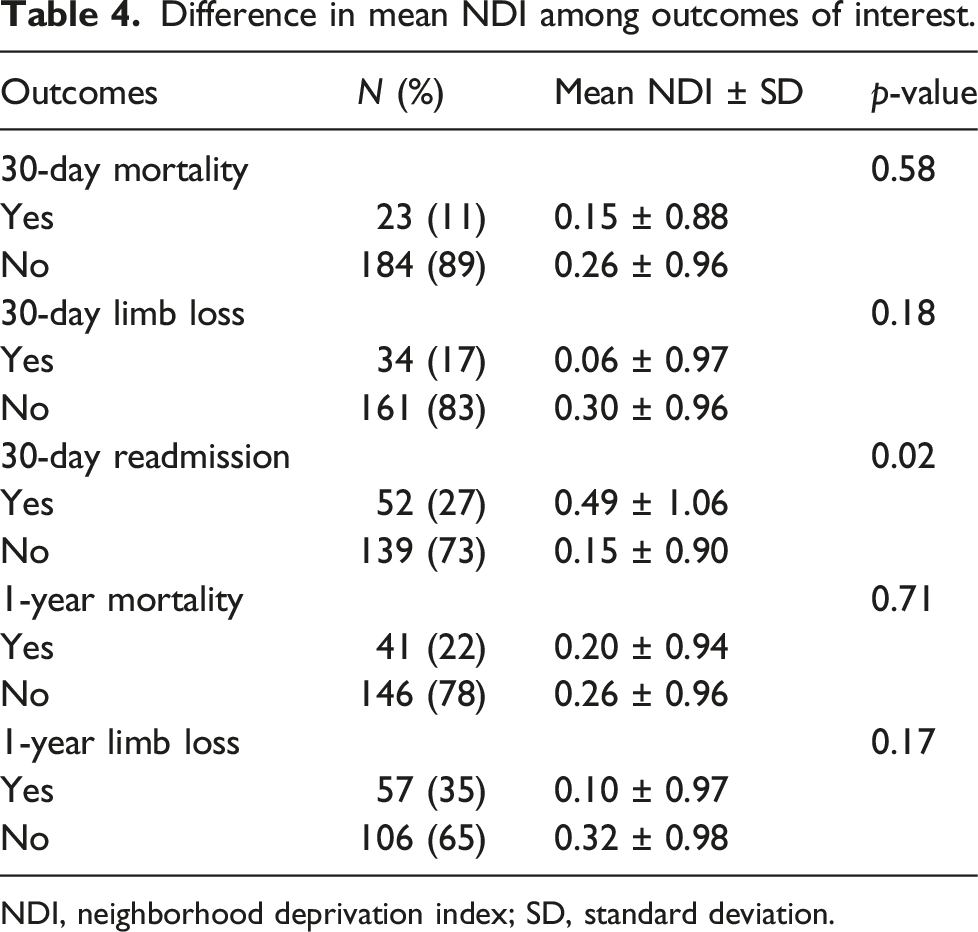
NDI, neighborhood deprivation index; SD, standard deviation.
Discussion
This study analyzed the association of SES with the severity of ALI and health outcomes of patients who presented with ALI in a general population-based sample in the United States. We found that SES was not associated with the short-term or 1-year amputation rate or mortality of patients who had presented with ALI. Although univariate analysis showed that patients with lower SES tended to be readmitted to the hospital at 30 days more often, this association was not significant after accounting for potential confounders. In addition, SES disparity was not associated with severity of ALI on presentation.
Many previous studies have observed an association of lower SES with worse outcomes in cardiovascular patients.6,7,14-17 Few studies have focused on SES and outcomes in PAD patients.8,9,18-20 Ultee et al. 18 retrospectively evaluated 324 patients with PAD and showed that low income was associated with worse postoperative survival (hazard ratio 1.05, 95% CI 1.0–1.1 per 5,650-US dollar increase). Hawkins et al. 19 studied 2,578 patients undergoing infrainguinal bypass for PAD between 2011 and 2017 and showed that patients with low SES were found to have increased short-term as well as 1-year rates of major adverse limb events (13% vs 10%; p = 0.03, and 21% vs 17%, p = 0.01, respectively). These findings were in accordance with another study by Arya et al., 20 who looked at 155,647 PAD patients admitted to the Veterans Affairs from 2003 to 2014 and showed that low SES was independently predictive of increased risk of amputation (hazard ratio 1.12, 95% CI 1.06–1.17). When looking at patients with advanced PAD, Henry et al. 9 showed that patients with lower SES were more likely to have limb amputation for their chronic limb threatening ischemia. Our study is the first to evaluate the ALI subset of PAD and showed that SES did not affect short-term or 1-year mortality or limb salvage outcomes in ALI patients, which might indicate that ALI patients would seek timely care regardless of their SES status.
One of the most popular explanations for the worse postoperative outcomes observed in low SES cardiovascular patients is the so-called “social gradient,” which posits that the incidence of a disease and subsequent outcomes are worse amongst the most deprived people. 21 This has pushed authorities to implement more targeted care in managing known cardiovascular risk factors in the least affluent populations. In our study, patients with lower SES were more likely to have had a history of PAD and chronic kidney disease, and there was a trend of having higher prevalence of hypertension on presentation. This could be due to a multitude of reasons as described in the literature, 22 including lack of access to healthcare, intrinsic health issues, or lack of education. Most of our patients had access to healthcare since almost all had health insurance, and they had a median of 4 office care visits per year per person. In addition, in our cohort, African American patients were more likely to have higher NDI (lower SES) than White patients. African American patients have a 2- to 3-fold higher prevalence of PAD than White patients, 23 and they are more like to have comorbid hypertension and chronic kidney disease.24,25 Moreover, patients with higher NDI in our study were less likely to be high school graduates (p < 0.001), which might reflect poorer health literacy. This might indicate that the higher prevalence of cardiovascular comorbidities in the least affluent patients in our cohort was most likely due to racial disparities, intrinsic health issues, or lack of education.
Lower SES has been shown to correlate with higher prevalence of PAD. 26 In addition, poverty has been shown to be a marker for more advanced PAD on presentation. 27 In our cohort, SES did not correlate with the Rutherford classification of ALI on presentation. Also, no correlation was seen when studying whether the distance from the hospital affected ALI severity on presentation. Moreover, it has been shown that patients with low SES, as defined by a high NDI, are more likely to use the Emergency Department as a primary destination for urgent health care instead of using a primary care physician’s office. 28 However, the emergency department is usually the preferable location to seek medical care in the setting of ALI. This suggests that ALI in any form may be a trigger for patients to seek medical care, regardless of SES or location.
Several definitions for SES have been used in the literature.10,12,29,30 No single variable can be all inclusive for quantifying SES owing to the numerous parameters that can be used to describe it. Rather, SES encompasses multiple societal factors, including wealth, occupation, income, and educational status. 31 In our analysis, we used a composite score that encompassed several variables to quantify SES, including educational level, median household income, percentage of people below the poverty level, family income, and the NDI. 32 This composite score minimizes the limitations of using a single variable to quantify SES. Originally, NDI was used to explore the association between low birth weight and SES. 33 NDI has also been used in studies that have shown that low SES is associated with up to 37% decreased probability of individuals participating in health checks. 34 Patients with high NDI also have been shown to have a lower likelihood of achieving long-term cessation of cocaine injection and opiate use. 12 Finally, patients with high NDI have been shown to be more likely to have a higher prevalence of adverse health behaviors such as physical inactivity, smoking, and unhealthy diet. 11 In our study, we observed that SES was not associated with the severity of disease on presentation or outcomes in ALI patients.
Within the current context of healthcare reform, our study draws important findings, since it is the first to explore whether SES is associated with the outcomes in patients with ALI, a highly morbid disease. With the rapidly changing forms of healthcare delivery systems aimed at preventing cardiovascular disease, our results suggest that regardless of the disease severity or SES status, patients with ALI would likely seek medical care for their disease and subsequently receive similar treatment modalities. This implies that healthcare resources should be directed toward other cardiovascular and PAD areas.
Limitations
The retrospective nature of this study allows determination of association and not causation, and an inherent selection bias existed since we are a referral center. Our cohort did not include the most deprived patients per the NDI, which might limit the generalizability of our results to the general population. Nonetheless, the average median household income was well below the national average. Our sample size might have introduced a type II error, and our follow-up time might not have been long-enough to detect significant differences should one exist. Personal interviews were not conducted with patients, which might have better corroborated their home locations and SES. Finally, algorithms based on patients’ census tract information were used to estimate SES variables, and hence, were not collected individually, which might have distorted some associations.
Conclusions
This study showed that although SES was associated with the presence of PAD and chronic kidney disease in patients presenting with ALI, it was not associated with the severity of ALI and was not predictive of short-term or 1-year limb loss and mortality in these patients. In this study, ALI presentation and health outcomes were independent of SES.
Our study is the first to link SES with the outcomes specifically in patients with ALI who were treated at a tertiary medical center. While our results need to be replicated, the findings are important to consider when making decisions about healthcare resource allocation within the context of current healthcare reforms and changes in delivery systems.
Footnotes
Author note
This study was presented as an oral presentation at the 45th Midwestern Vascular Surgical Society Meeting, Chicago, IL, September 9–11, 2021.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Betty Jane and Alfred J. Fisher Vascular Surgery Research Fund.