
Abstract
Background
Vascular abnormalities, including dissections and aneurysms, can be found in patients with autosomal dominant kidney disease (ADPKD). While intracranial aneurysms have been reported in 10%–25% of ADPCKD, occurrences at other locations are exceedingly rare.
Method
This is a first case report of a patient with ADPCKD who presented with a rupture of the left external carotid artery pseudoaneurysm.
Conclusion
Rupture of a carotid artery aneurysm is rare with potentially high morbidity. An endovascular and surgical approach are effective strategies for successful management that depends on etiology, location, and surgeon experience.
Keywords
Introduction
Vascular abnormalities, including dissections and aneurysms, can be found in patients with autosomal dominant polycystic kidney disease (ADPCKD). 1 While intracranial aneurysms have been reported in 10%–25% of ADPCKD, occurrences at other locations are exceedingly rare. 2 We describe the case of a patient with ADPCKD who presented with a rupture of the left external carotid artery pseudoaneurysm.
Case report
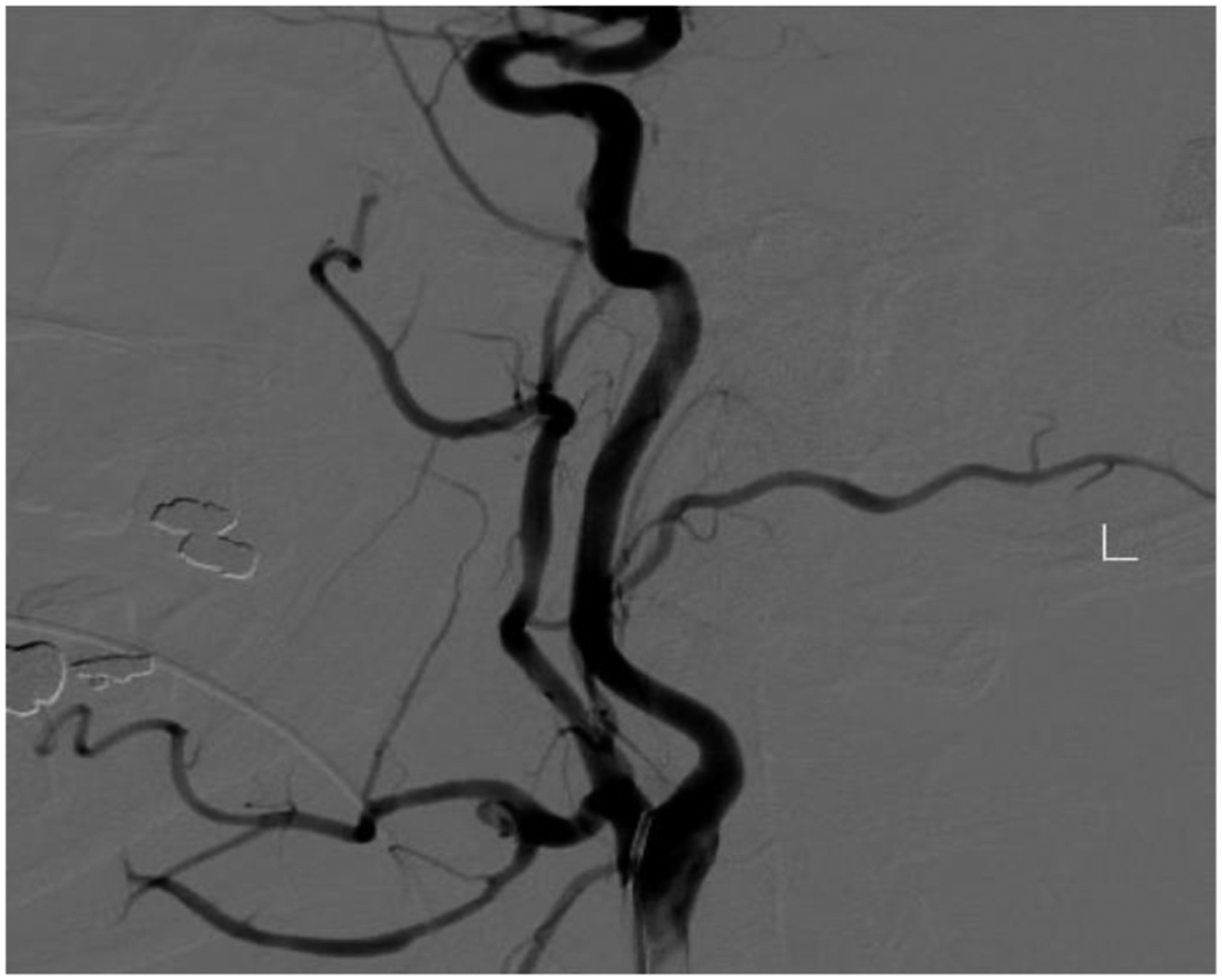
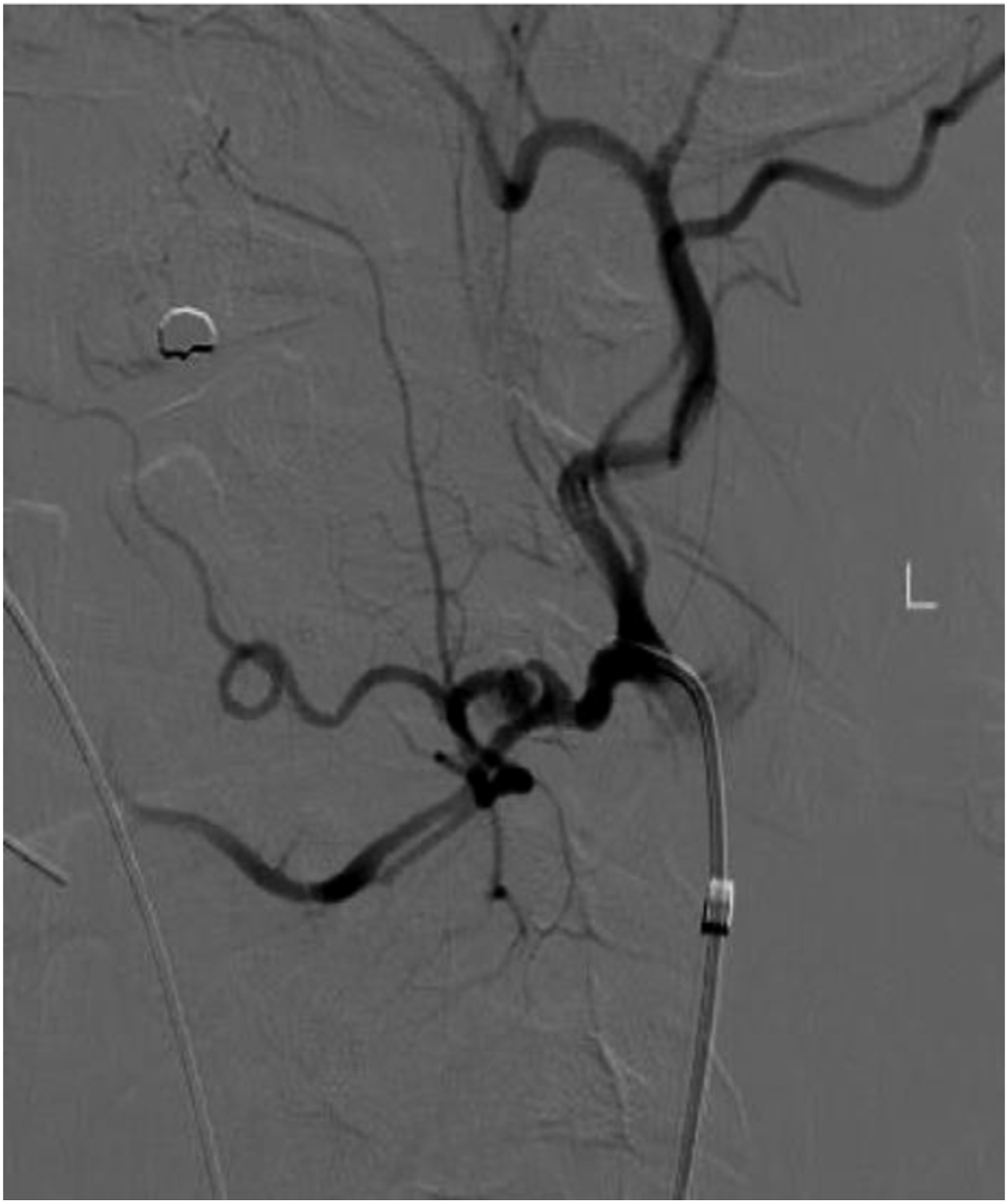
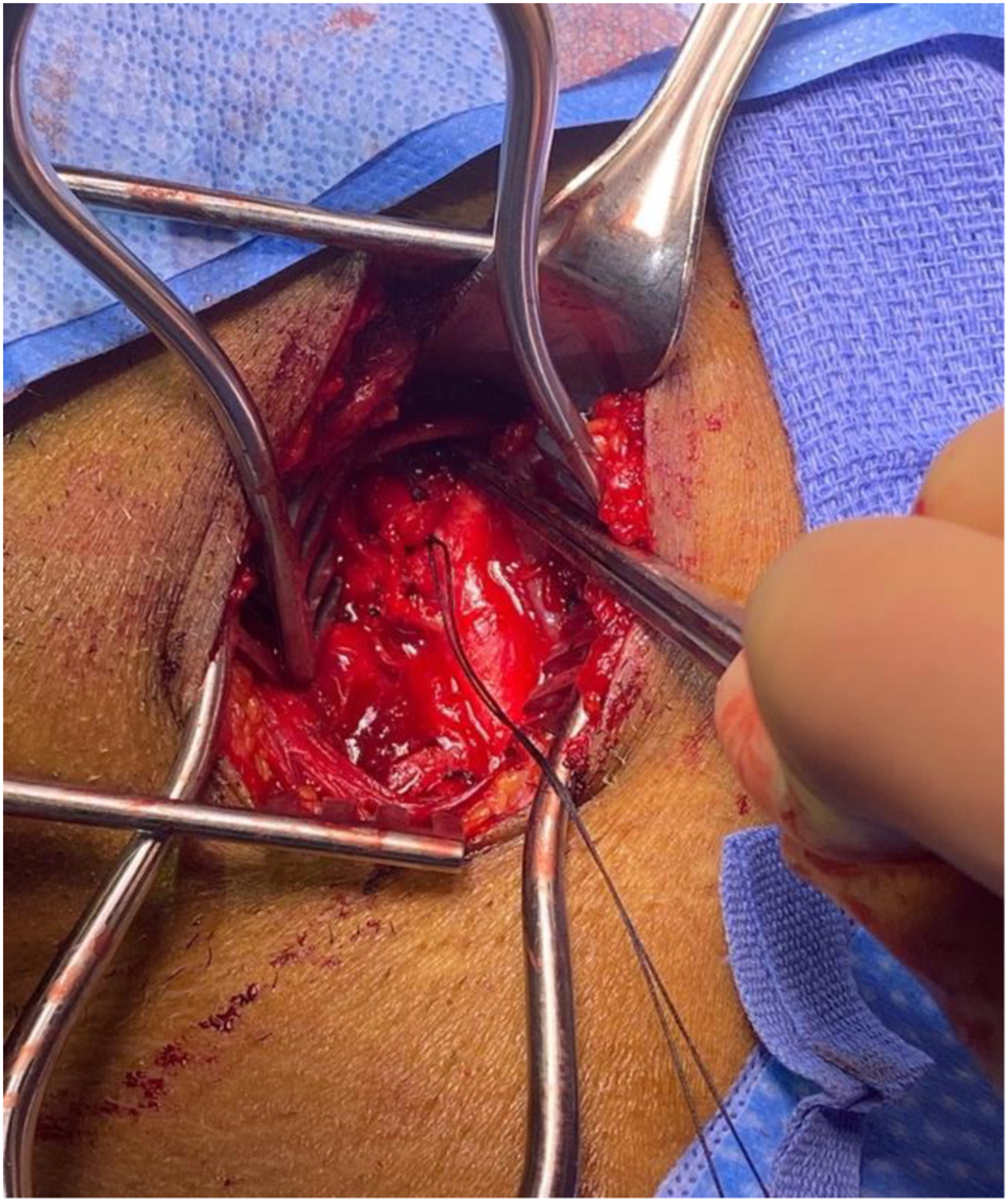
A 44-years-old male with a history of ADPCKD post remote kidney transplant presented to the emergency department with a spontaneous onset of left-sided neck pain and swelling. There was no history of trauma. A computed tomography angiogram revealed a pseudoaneurysm of the external carotid artery between the origin of the lingual and facial artery, with a large hematoma resulting in deviation of the trachea to the right. (Figure 1) The patient was promptly intubated in the emergency department for airway protection. A carotid angiogram was performed through right femoral artery access (Figure 2), and the pseudoaneurysm was embolized using three 5-mm Tornado coils (Cook. Inc) (Figures 3 to 5). Then he was brought to the operating room for neck exploration and hematoma evacuation. The cervical carotid artery was exposed through an incision along the left anterior border of the sternocleidomastoid. The lack of active bleeding confirmed the successful embolization. To prevent a potentially lethal future hemorrhage, we ligated the proximal external carotid artery flush at the bifurcation (Figure 6). The patient was transferred to the intensive care unit, intubated, and stable. On a postoperative day one, the patient was extubated and discharged home on postoperative day three. The patient was seen postoperatively and was doing well. CTA neck. Carotid angiogram. Selective ECA catheterization. ECA branch embolization. Post embolization. ECA ligation.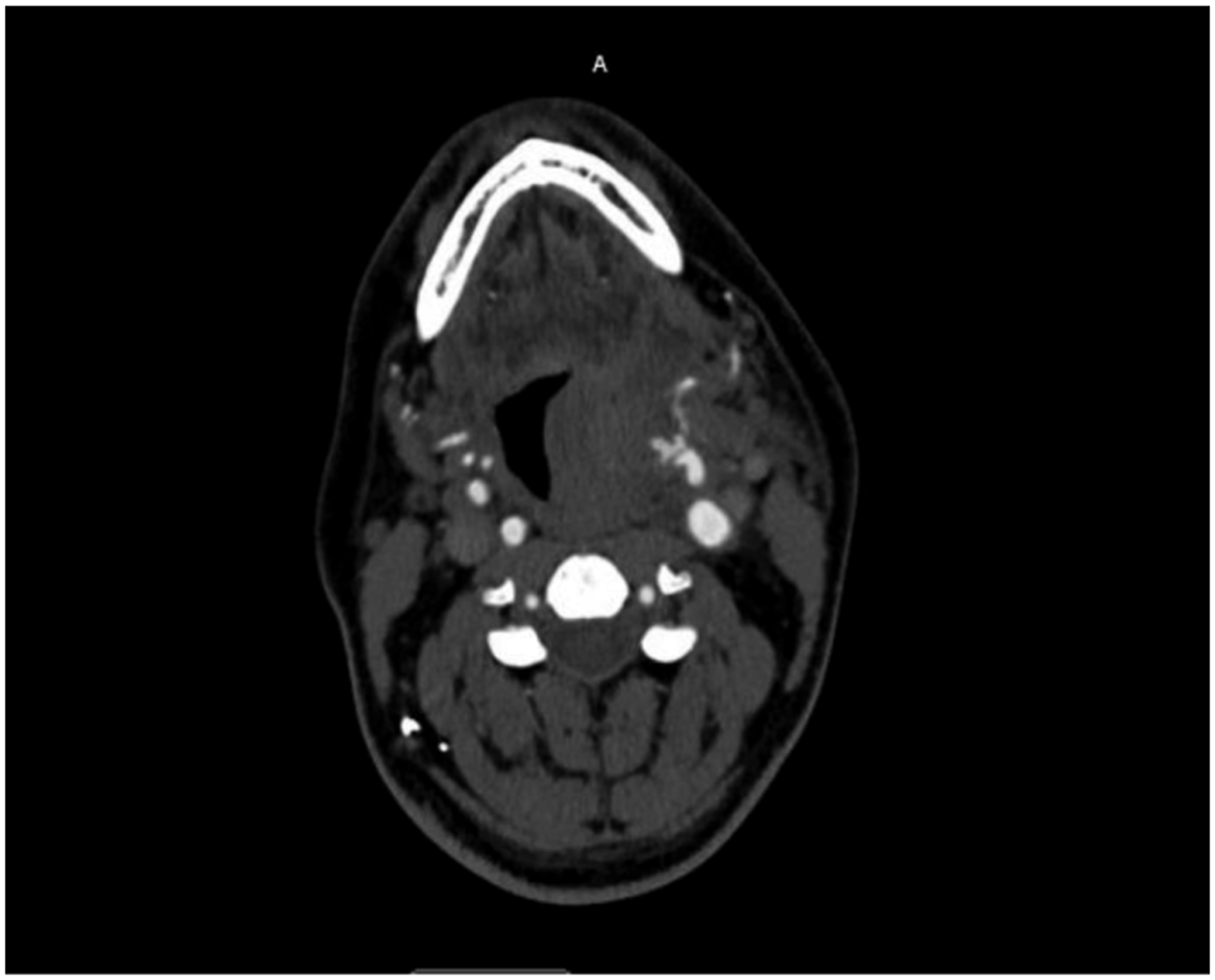


Discussion
Carotid artery aneurysms are rare, most commonly resulting from atherosclerosis, trauma, infection, dissection, or connective tissue disorders.3,4 Rupture of the carotid artery aneurysms is extremely rare; Martins de Souza et al. reviewed and analyzed the report of 74 patients who suffered a ruptured extracranial carotid artery aneurysm (true aneurysm or pseudoaneurysm)and concluded that infection was the most common cause of the rupture. 5 Also, patients who have undergone extensive head and neck surgery or cervical radiation therapy are at increased risk of a carotid blowout. 6 There were few reports of spontaneous carotid ruptures not associated with trauma, aneurysm, or carotid blowout syndrome.7–10 Pseudoaneurysms of the carotid artery are very rare in clinical practice, with an incidence of 0.07%. The most common etiology of carotid pseudoaneurysms is trauma, whether from penetrating or blunt neck trauma. 11 Carotid Pseudoaneurysms can occur following carotid endarterectomy or as a late sequel of carotid artery dissection. 11
This is the first report of a carotid pseudoaneurysm in a patient with ADPCKD. Dissections and aneurysms of almost every large artery have been reported in patients with ADPCKD, including the aorta, coronaries, cervico-cephalic, vertebral, and cranial arteries. 2 The mechanism of aneurysm formation remains unclear. Still, it may be related to partial inactivation or deletion of the PKD 1 or PKD 2 genes responsible for ADPCKD with alterations in intracellular calcium signaling, modifier genes, and changes in TGF-β signaling. 2
Management of carotid aneurysms includes open reconstruction, ligation, or endovascular embolization. 5 The location and etiology of carotid artery aneurysms dictate the most appropriate approach. Aneurysms located in zone I (including the thoracic inlet to the cricothyroid cartilage) or zone III (Above the mandible angle) should be approached endovascularly to avoid extensive exposure in the form of a sternotomy, mandibulotomy, or other unusual techniques. 5 Zone II lesions may be approached endovascularly or using conventional surgical procedures. 5
We elected to proceed with a hybrid approach given the location of the pseudoaneurysm to avoid a distal dissection possibly complicated by a nerve injury in the setting of a large hematoma. After controlling the bleeding source with coils, we explored the neck for hematoma evacuation and airway decompression. There was no active bleeding, but the external carotid appeared fragile with a sub-adventitial hematoma. Given the unknown nature of the pathology, we decided to proceed with ligation of the external carotid with a silk stick tie flush at bifurcation to prevent further bleeding. Ligation was ensured by doppler.
Conclusion
Rupture of a carotid artery aneurysm is rare with potentially high morbidity. An endovascular and surgical approach are effective strategies for successful management that depend on etiology, location, and experience of the surgeon.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent
The patient’s permission was obtained for the case report.