
Abstract
Objectives
Peripheral artery disease is estimated to affect 237 million individuals worldwide. Critical limb ischaemia, also known as chronic limb threatening ischaemia is a consequence of the progression of peripheral artery disease which occurs in ∼21% of patients over a five-year period. The aim of this systematic review is to assess the use of additional below-the-ankle angioplasty in comparison to the use of above-the-ankle angioplasty alone, and the subsequent rates of amputation, wound healing, restenosis, rest pain, reintervention and complications.
Methods
This systematic review was undertaken in accordance with PRISMA guidelines following a registered protocol (CRD42019154893). Online databases were searched using a search strategy of 20 keywords. Included articles reported the outcome for inframalleolar (pedal artery, pedal arch, plantar arteries) angioplasty with additional proximal angioplasty in comparison to proximal angioplasty alone. GRADE assessment was applied to assess the quality of the evidence.
Results
After screening 1089 articles, 10 articles met the inclusion criteria. Comparative performance assessment of below-the-ankle with above-the-ankle versus above-the-ankle angioplasty alone was undertaken in 3 articles, with the remaining 7 articles reporting outcomes of below-the-ankle with above-the-ankle angioplasty with no distinct comparator group. Significant decrease in major lower limb amputation at the last follow-up in the below-the-ankle group when compared with the above-the-ankle angioplasty alone group was observed in a single study (3.45% vs. 14.9%, p < 0.05). Improved wound healing rate at follow-up in the below-the-ankle group versus above-the-ankle angioplasty alone group was also reported in a single study (59.3% vs. 38.1%, p < 0.05). Subsequent rate of amputation after below-the-ankle angioplasty has been estimated as 23.5%.
Conclusion
To date, there is a lack of studies assessing inframalleolar interventions and their use in improving limb salvage, wound healing and symptomatology. Prospective RCTs should be undertaken with adequate participant numbers to be sufficiently powered and report clinically important end-points.
Keywords
Background
Peripheral arterial disease (PAD) is estimated to affect 237 million individuals worldwide. 1 Contemporary figures report the annual prevalence of PAD amongst all hospital admissions as being as high as 10.7%. 2 PAD is a significant cause of morbidity and is known to be associated with other cardiovascular disease such as coronary artery and cerebrovascular disease.3,4 Co-existing coronary artery disease on angiography and carotid artery stenosis of >70% has been identified in 90% and 25% of PAD patients, respectively. 4 PAD represents a significant cause of death with an annual all-cause mortality of 8.2% and crude five-year all-cause mortality rate of 33.2%. 5
Critical limb ischaemia (CLI), also known as chronic limb threatening ischaemia (CLTI), is a consequence of the progression of PAD which occurs in ∼21% of patients over a five-year period. 6 CLI represents PAD in its most severe form and patients reaching CLI have increased risk of cardiovascular death, myocardial infarction or ischaemic stroke in comparison to non-critical PAD 6 . All-cause mortality for inpatients with CLI is estimated to be 8.4%. 4 Treating CLI can improve rates of limb salvage, wound healing and provide symptomatic relief. However, intervention can be complicated by restenosis, wound infection and subsequent need for amputation, 7 the latter being related to a combination of arterial, patient-related and interventional factors.
Infrapopliteal arterial disease is prevalent in diabetic populations and is challenging to treat.8,9 Development of endovascular techniques and advances in guidewire and stent design have facilitated below-the-ankle (BTA) revascularisation strategies. 10
An example of this is the pedal-plantar loop technique which permits revascularisation of both main arteries of the foot via one patent calf vessel and the plantar arch. 10
In the United Kingdom, the National Institute for Health and Care Excellence (NICE) recommends utilising endovascular angioplasty or surgical bypass interventions in the management of CLI depending on medical and technical factors. 11 There is currently insufficient evidence for recommendations regarding use of inframalleolar angioplasty and its outcome in the treatment of proximal below-knee arterial disease. The Global Vascular Guideline for management of chronic limb-threatening ischaemia mirrors the NICE guidelines stating that there is insufficient evidence to provide recommendations on the impact of inframalleolar disease on the success of proximal intervention. 12
The aim of this systematic review is to assess the use of BTA angioplasty to the pedal artery, pedal arch or pedal branches in addition to proximal revascularisation in comparison to the use of above-the-ankle (ATA) angioplasty alone, assessing the outcomes of amputation, wound healing, restenosis, rest pain and complications at last reported follow-up.
Methods
This systematic review was undertaken in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 13 following a publically available registered protocol (PROSPERO: CRD42019154893).
Search strategy
The Ovid® online platform was used to search the Medline database on 11 December 2020 searching from 1946 to 2020 with no restrictions imposed. The Cochrane Library® online platform was used to search the Cochrane database on 11 December 2020 with no restrictions imposed. Relevant online platforms were used to search through randomised-controlled trial (RCT) registries; the following databases were inspected: ClinicalTrials.gov®, European Union Clinical Trials® and the International Standard Randomised Controlled Trial Number (ISRCTN) Registry®.
Searches consisted of 20 terms including keywords for endovascular interventions and below ankle vessels (see Supplement 1). For online platforms, the searches were performed based on “All Fields”. No limitations were imposed regarding date, study design or language. Additionally, the references of included articles were also screened for further eligible articles.
Eligibility criteria
Eligible studies were those performed in secondary care recruiting patients undergoing either day case or inpatient revascularisation interventions for CLTI of the lower limb. The majority of patients were admitted as an emergency after presenting with CLTI symptoms and signs. Participants underwent angioplasty to infrainguinal vessels with the addition of inframalleolar intervention in attempt to achieve in-line flow to the foot.
Included articles had following characteristics: Articles reported the outcome for the use of BTA angioplasty to the pedal artery, pedal arch or pedal branches in addition to proximal revascularisation, in comparison to the use of ATA angioplasty alone as a comparative study. Articles reported the rates of amputation, post-intervention symptomatology, wound/ulcer healing or restenosis. Articles reported the performance of BTA angioplasty in addition to proximal angioplasty without a distinct comparator arm as a non-comparative study.
Excluded articles had the following characteristics: Articles reported the use of pedal artery as an access site only to gain access to infrainguinal vessels. Articles reported non-original research, e.g. narrative review articles. Articles in which the full-text was not available in the English language. Conference abstracts that were not published as full-text publications in a peer-reviewed journal. Articles that were duplicate publications, i.e. have been previously published as full-text publications. Articles conducted using data from animals, i.e. non-human studies. Case reports.
Article screening
Retrieved articles were screened against the inclusion criteria by two reviewers (MM, HCY) independently using EndNote X9®. Mediation of articles to be included was carried out independently by a third reviewer (SO). Articles were initially screened based on the title and abstract. Eligible articles then underwent full-text review.
Data extraction
Two reviewers (MM, HCY) extracted, mediated and discussed the data using a template in Microsoft Excel 2013©. Any discrepancies in the data extraction were mediated by a third reviewer (SO).
Quality assessment
The online platform GradePro was used to undertake Grading of Recommendations Assessment, Development and Evaluation (GRADE) assessment for the comparison of the aforementioned outcomes.
Data synthesis
To assess heterogeneity, outcome data were imported into RevMan 5®. Given the substantial heterogeneity in study design, study size, variations in procedure and differing outcomes reported, and there were only three trials reporting direct comparison between BTA angioplasty with ATA angioplasty alone, a qualitative analysis was performed.
Results
Literature search
Searches of online databases yielded a total of 1089 unique articles (see Figure 1 PRISMA flow-chart). Screening based on title and abstract resulted in the exclusion of 1057 articles. Subsequent full-text review of 32 articles led to the exclusion of 22 studies for the following reasons: no outcome data reported for BTA angioplasty: 6, no BTA angioplasty performed: 4, conference abstract: 3, case report: 8, and data were subsequently reported in more contemporary full-text publication: 1. Narrative synthesis was performed on 10 articles.14–23
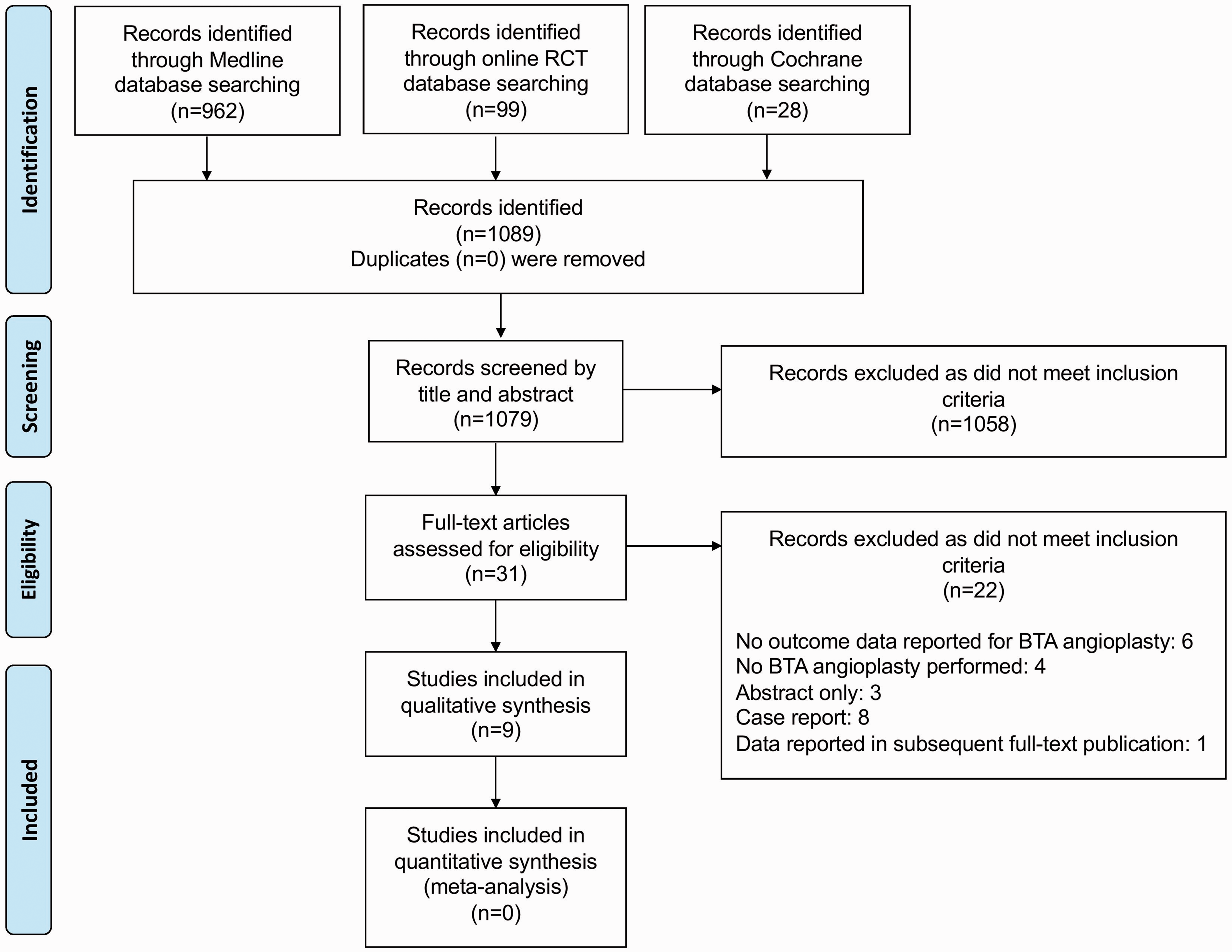
PRISMA flow-chart illustrating article selection.
Study characteristics (see Tables 1 and 2)
Prospective, non-randomised, non-controlled study design was undertaken in four articles.17,18,22,23 Retrospective cohort analysis was performed in six articles.14–16,19–21 Direct comparison of the performance of BTA angioplasty with ATA angioplasty alone was reported in three articles; all had retrospective study designs.14–16 The remaining seven articles reported the performance of BTA alongside additional ATA angioplasty with no comparator arm.17–23
Articles were all published in the last 10 years, with a range from 2009 to 2019. Studies were undertaken in China, 17 Greece, 19 Italy,18,22 Japan, 16 Korea, 14 Turkey, 15 UK, 21 and USA.20,23 Participant number ranged from 20 to 257 with a total of 643 patients undergoing BTA angioplasty and 240 participants acting as controls undergoing ATA angioplasty alone. Mean age of participants ranged from 58 to 73.5 years.
The majority of participants were male with mean percentage of male participants ranging from 64.3% to 78.4%. All 10 articles included patients with CLI of the lower limb. A single article included only diabetic patients with CLI. 15 A single study included patients with only type-2 or type-3 pedal arch (i.e. pedal arch disease). 14 A proportion of participants in a single article did not meet criteria for CLI – the cohort included patients with Rutherford classification I–VI disease. 17
Quality of evidence
GRADE assessment for the performance of limb salvage/amputation prevention in the BTA angioplasty arm in comparison to the ATA angioplasty alone arm revealed a very low certainty in the evidence (see Supplement 2). GRADE assessment was not performed for the rates of wound healing, restenosis and rest pain outcomes due to insufficient data reported in the included studies. There is no certainty in these outcomes. There was no indication to perform funnel plots to assess for risk of publication bias.
Interventions (see Tables 1 and 2)
All articles reported the use of proximal infrainguinal or infrapopliteal angioplasty with additional angioplasty to the pedal artery, pedal arch or plantar arteries with the exception of two participants where only BTA angioplasty was utilised as the disease was confined to the foot. 19 Angioplasty technique was transluminal with exception of two articles in which either transluminal or subintimal strategies were used.14,18 Deployment of below-ankle stents was reported in two articles when balloon angioplasty was insufficient.19,20
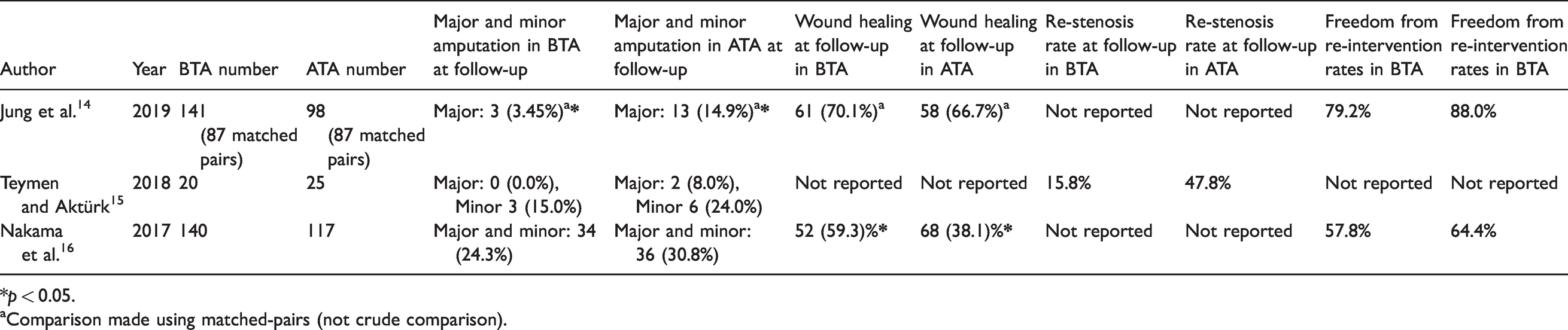
Limb salvage (see Tables 3 and 4)
All included articles reported on the incidence of amputation during follow-up. Limb salvage rates were compared for BTA angioplasty versus ATA angioplasty alone in three articles.14–16 A single article reported a significant decrease in major lower limb amputation in the BTA arm in comparison to the ATA angioplasty alone arm (3.45% vs. 14.9%, p < 0.05) at a median of 644 days. 14 Teymen and Aktürk15 reported a decrease in major and minor lower limb amputation in the BTA angioplasty arm in comparison to the ATA angioplasty alone arm (0.0% vs. 8.0%, and 15.0% vs. 24.0%, respectively) at 12-month follow-up; however, this failed to reach statistical significance. 15 The remaining comparative study combined minor and major amputation as a single outcome. 16 Similar rates of minor and major amputation in both the BTA arm and the ATA arm at 12-month follow-up (24.3% vs. 30.8%, p > 0.05) were reported 16 /
Incidence from the remaining non-comparative studies reported the following rates of minor amputation: 33%, 23 53.3%, 20 46.5%, 22 26.2%, 21 15.8% 18 and 4.5%. 17 Rates of major amputation were 4%, 23 16.7%, 20 16.6%, 21 4.5%, 17 2.63% 22 and 0%. 18 Across the articles reporting amputation rates, a total of 622 patients received BTA angioplasty and 163 subsequently underwent amputations at any level, giving a pooled incidence of 26.2%.
Wound healing (see Tables 3 and 4)
Outcomes for wound healing were reported in four articles.14,16,17,20 A single study reported a significant increase in the rate of wound healing at 12 month follow-up in the BTA angioplasty arm in comparison to the ATA angioplasty alone arm (59.3% vs. 38.1%, p < 0.05). 16 Time to wound healing was also significantly shorter in the BTA angioplasty arm (211 days vs. 365 days, p = 0.008). Interestingly, despite reporting a significant difference in limb salvage, Jung et al. reported similar rates of wound healing across both arms. 14
One article reported that 83% of participants achieved the composite outcome of improvement in rest pain or wound healing at follow-up. 24 Distinction between these two outcomes was not reported.
Improvement in rest pain (see Tables 3 and 4)
A binary outcome for rest pain was reported in a single article. 21 There were no comparative pain outcomes reported for rest pain for BTA angioplasty versus ATA angioplasty alone. Abdelhamid et al. reported that just two patients had rest pain at follow-up but did not state the number of patients experiencing rest pain pre-intervention. 21 Kawarada et al. reported a composite outcome of improvement of rest pain and wound healing. 20 Wei et al. used improvement in rest pain as an outcome but did not report symptomatology at follow-up. 17
Quality of life
A single article reported Stark questionnaire Quality of Life (QoL) scores at one, three and six months post-procedure. 23 They saw an overall increase in QoL scores (−1.3 pre-study to 0.7 at six months follow-up) and significant increases in activity (‘fairly’ to ‘well’, p = 0.014) and mood parameters (0 to +1, p = 0.033). 23
Restenosis (see Tables 3 and 4)
Restenosis rates were reported in three articles.15,17,19 A single article reported lower restenosis rates in the BTA angioplasty arm in comparison to the ATA angioplasty alone arm which approached significance at one year (15.8% vs. 47.8%, p = 0.059). 15 Katsanos et al. and Wei et al. reported incidence of restenosis at follow-up to be 64.1% at 19.6 months and 54.5% at 24 months, respectively. 19
Reintervention
A total of six articles reported reintervention rates after BTA angioplasty.14,16,19–22 There was no significant difference in reintervention rates between the BTA angioplasty and ATA alone angioplasty groups in the comparative articles.
Pooled analysis of articles reporting reintervention rates (n = 580) demonstrated that 114 underwent reintervention post-BTA angioplasty, representing an overall freedom from re-intervention of 80.3% at follow-up.
Complications (see Tables 3 and 4)
In comparative studies, complication rates did not differ significantly between the BTA angioplasty in comparison to ATA angioplasty alone arms.
Failure of procedure was the most common complication of BTA angioplasty and was reported in seven articles. Failure of procedure occurred in 55 of the 440 patients from the articles reporting the complication; a corresponding pooled risk of 12.5%. Specific reasons for failure of procedure were not reported. Other reported complications included: acute arterial occlusion, subacute arterial occlusion, rupture of artery, balloon rupture, haematoma at insertion site, vasospasm and bleeding, with a total of 106 complications occurring in the 580 patients who underwent BTA angioplasty. The incidence of these complications was highly variable between studies.
Duration of follow-up
Mean follow-up duration ranged from 6 months to 19.6 months. Follow-up duration was 12 months in 3 articles15,16,18 and 24 months in 4 articles.17,19–21 Palena et al. had a follow-up duration of 6.7 months and was the only article to report no subsequent major lower limb amputations. 18
Discussion
We present what we believe to be the first systematic review assessing the performance of below-the-ankle percutaneous angioplasty in addition to infrainguinal or infrapopliteal angioplasty. From this, it can be concluded there is presently little formally published evidence to support the use of inframalleolar angioplasty. A single significant finding for limb salvage was identified.
Patency of the pedal arch after infrainguinal angioplasty has been previously found to be prognostic of outcome. Higashimori et al. undertook a retrospective analysis of 312 patients undergoing below-knee angioplasty for critical limb ischaemia; within this there were 137 patients who were identified as having one-vessel run-off. 25 Amputation-free survival was significantly higher in patients that had a patent pedal arch, defined as arterial flow through one of dorsalis pedis or common plantar through to the main contralateral pedal artery via the connection via the deep penetrating artery, in comparison to those that did not (88.2% vs. 65.6%, p = 0.01).
A single study reported a significant improvement in wound healing rate and time to healing with additional BTA angioplasty. 16 This is supported by evidence in the literature that post-intervention pedal arch classification is independently associated with wound healing. 24 However, individuals with severe pedal arch disease are more likely to have diabetes or more extensive PAD. 26
It is possible that pedal arch patency is entirely a prognostic indicator rather than a meaningful therapeutic goal, and hence by undergoing revascularisation the outcome is unchanged. This is the conclusion reached by Cheun et al. in their study examining outcomes for 109 diabetic patients undergoing isolated inframalleolar intervention.26,27 Although technical success was 81% with acceptable short-term results, five-year freedom from major adverse limb events was 27% ± 9%. 27
Due to the retrospective study designs, we are unable to infer how many patients did not undergo BTA angioplasty because it was decided that this approach would have failed (either in crossing the lesion or failure of treatment); the cohorts therefore may be subject to confounding by indication, i.e. high-risk pedal interventions did not occur. This makes the complication rates reported in this paper less representative of unselected pedal interventions.
Participant numbers in the included articles were low. There were no sample size calculations reported in any of the three comparative articles. Given the lack of significant results and small total participant number, it is likely that these comparative trials were underpowered.
An interventional study is clearly required in this area. The results from this systematic review can help to inform sample size calculations and effect sizes for limb salvage and wound healing outcomes for such future studies.
Limitations
Included articles were heterogeneous with differing study designs including prospective, non-randomised and retrospective cohort studies. Reported performance outcomes differed across the included articles with rate of limb salvage being the only consistent outcome. Other outcomes were inconsistently reported.
The number of included articles and total participant numbers were low, limiting the validity of any outcomes reported, e.g. rate of limb salvage. Due to lack of sufficient articles and significant heterogeneity, a meta-analysis was not performed. The quality of evidence for reported outcomes was deemed as low. This limits the applicability of the comparison between inframalleolar angioplasty as an adjunct to infrainguinal or infrapopliteal angioplasty.
Conclusion
Existing evidence in the literature suggests that patency of the pedal arch is a prognostic indicator; however, it is unclear if this is confounding by indication rather than a therapeutic goal. There is a lack of studies assessing inframalleolar interventions and their use in improving limb salvage, wound healing and symptomatology. The existing evidence is heterogeneous consisting of differing study size, study design and utilisation of different endovascular approaches.
Study characteristics for comparative studies.
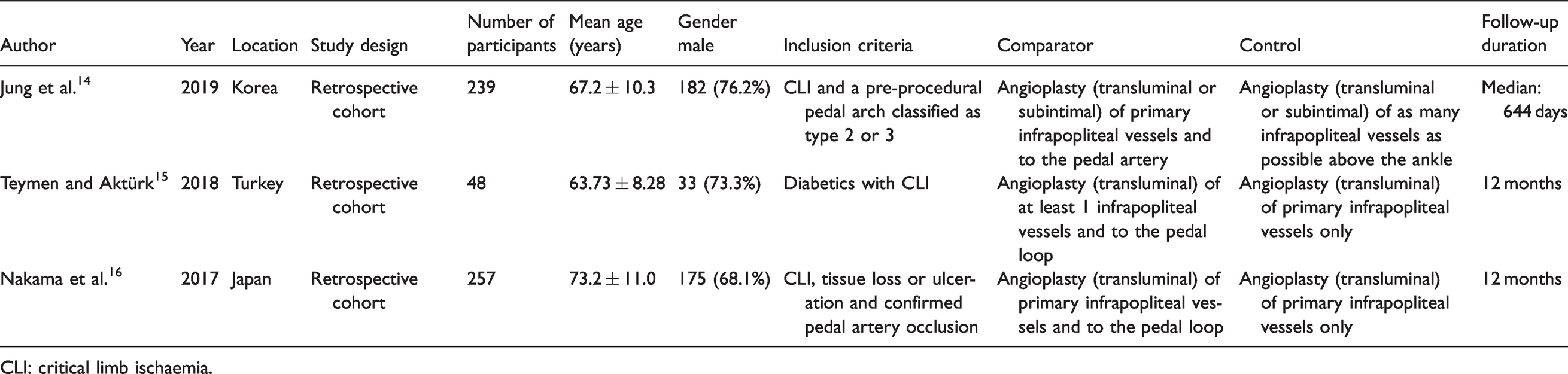
CLI: critical limb ischaemia.
Study characteristics for studies with single arm (non-comparative).
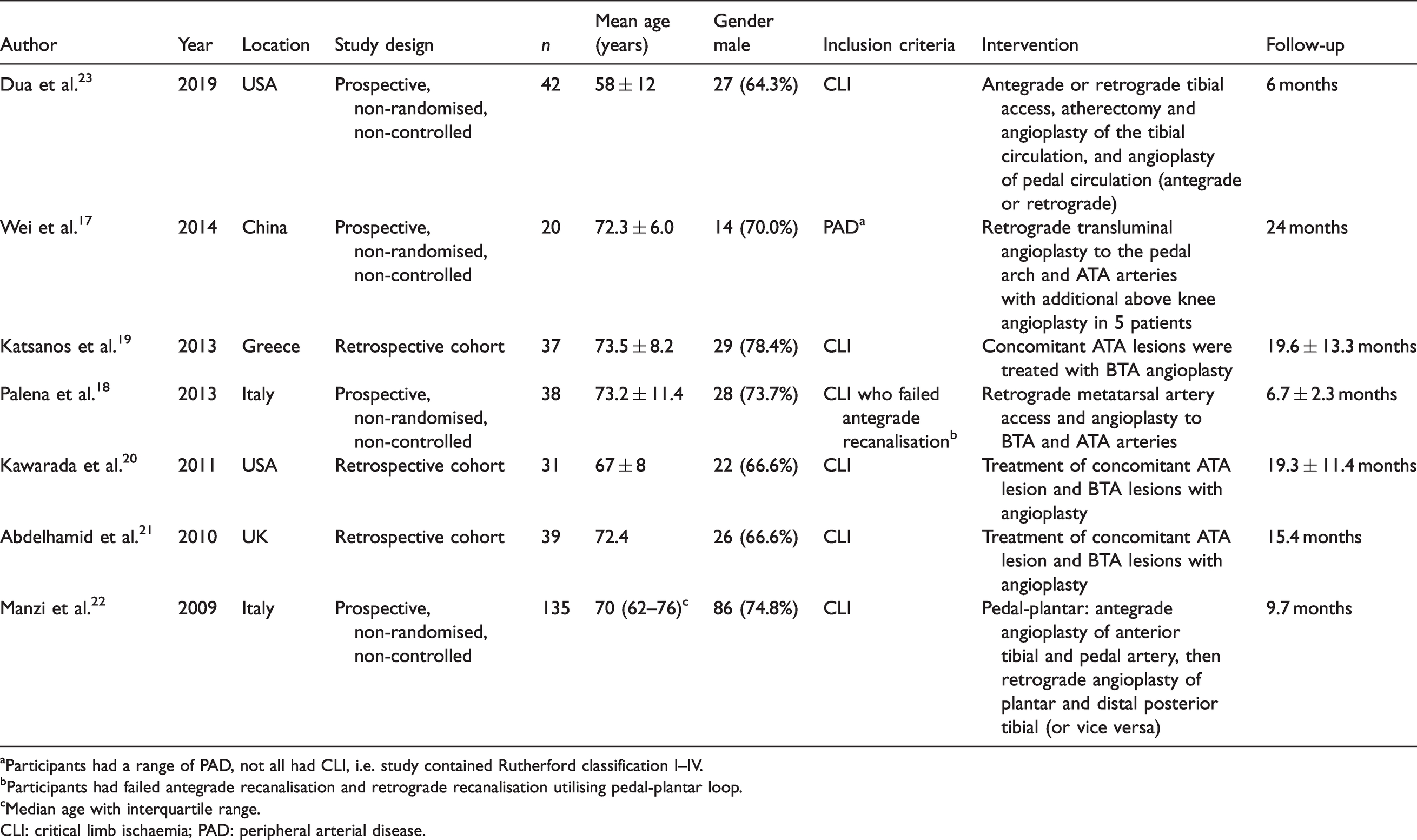
aParticipants had a range of PAD, not all had CLI, i.e. study contained Rutherford classification I–IV.
bParticipants had failed antegrade recanalisation and retrograde recanalisation utilising pedal-plantar loop.
cMedian age with interquartile range.
CLI: critical limb ischaemia; PAD: peripheral arterial disease.
Study outcomes for comparative studies.
*p < 0.05.
aComparison made using matched-pairs (not crude comparison).
Study outcomes for studies with single arm (non-comparative).
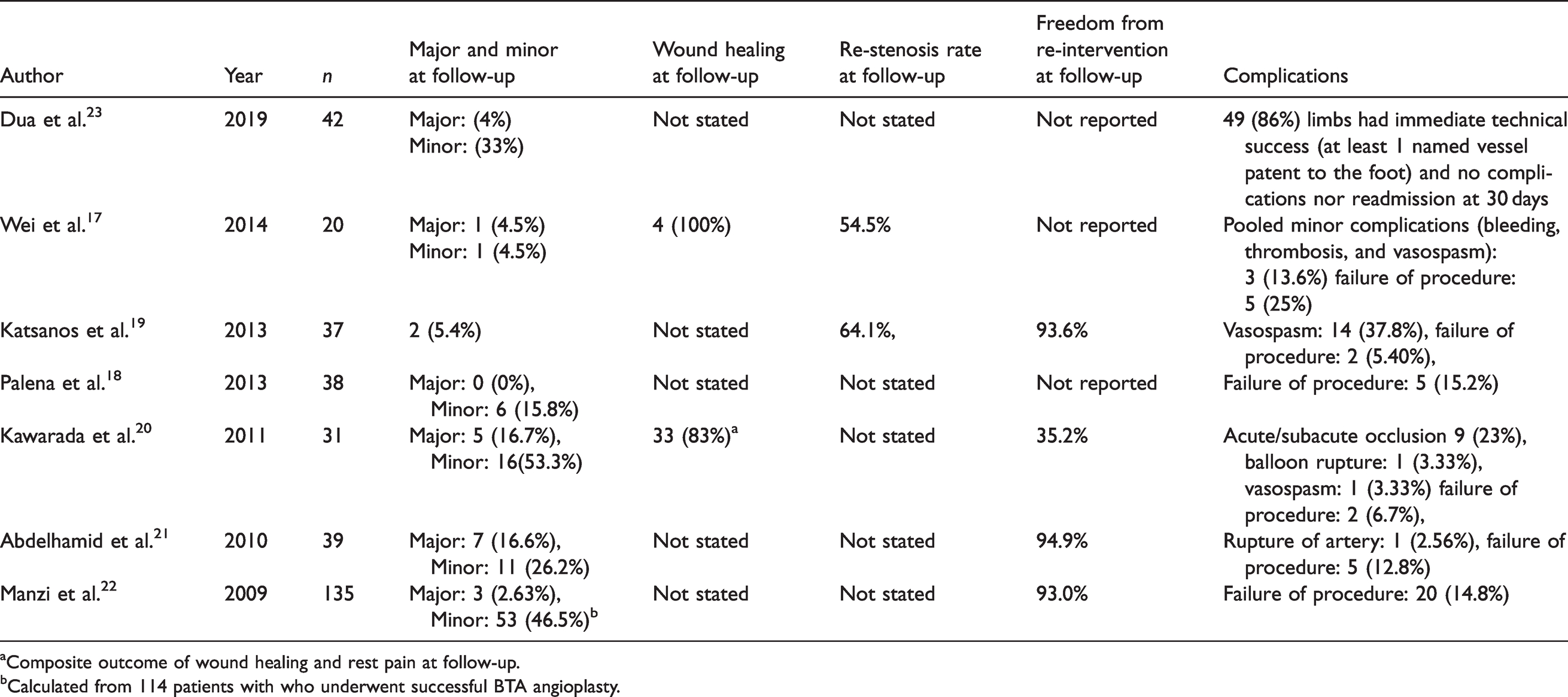
aComposite outcome of wound healing and rest pain at follow-up.
bCalculated from 114 patients with who underwent successful BTA angioplasty.
Supplemental Material
sj-pdf-1-vas-10.1177_17085381211004246 - Supplemental material for Systematic review of inframalleolar endovascular interventions and rates of limb salvage, wound healing, restenosis, rest pain, reintervention and complications
Supplemental material, sj-pdf-1-vas-10.1177_17085381211004246 for Systematic review of inframalleolar endovascular interventions and rates of limb salvage, wound healing, restenosis, rest pain, reintervention and complications by M Machin, HC Younan, AM Guéroult, S Onida, J Shalhoub and AH Davies in Vascular
Supplemental Material
sj-pdf-2-vas-10.1177_17085381211004246 - Supplemental material for Systematic review of inframalleolar endovascular interventions and rates of limb salvage, wound healing, restenosis, rest pain, reintervention and complications
Supplemental material, sj-pdf-2-vas-10.1177_17085381211004246 for Systematic review of inframalleolar endovascular interventions and rates of limb salvage, wound healing, restenosis, rest pain, reintervention and complications by M Machin, HC Younan, AM Guéroult, S Onida, J Shalhoub and AH Davies in Vascular
Footnotes
Authors’ contributions
Study design: AHD, JS, MM.
Data collection: MM, HCY, AMG, SO.
Data analysis: MM, HCY, AMG, SO.
Writing: MM, HCY, AMG, SO, JS, AHD.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Infrastructure support for this work was provided by the NIHR Imperial Biomedical Research Centre.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.