
Abstract
The aim of this case series was to document our early experience using combination therapy with UltraScore™ Focused Force percutaneous transluminal angioplasty balloon (BD Interventional, New Jersey, US) and Selution Sustained Limus Release (SLR)™ (M.A. MedAlliance SA, Nyon, Switzerland) sirolimus-coated balloon catheter for anti-restenotic drug elution, in the setting of multifocal high-grade stenosis for chronic limb threatening ischaemia. Our anecdotal experience was that preparing the lesion with scoring balloon and then using sirolimus drug-eluting balloon may have synergistic effect when used in tandem, especially in the setting of calcified arterial lesions, where the scoring wires may achieve deeper clefts within the atheromatous plaque to allow better drug absorption into the arterial wall. We report two cases with high-grade multifocal stenosis affecting the superficial femoral and anterior tibial arteries, respectively. Combination therapy using the scoring balloon to first prepare the lesion followed by sirolimus elution achieved technical and procedural success in both cases and a 100% 30-day primary patency. There were no complications related to flow-limiting dissections, vessel perforation or acute recoil. However, whether this combination therapy leads to better primary vessel patency with longer freedom from target lesion revascularization in the medium term remains to be determined.
Keywords
Introduction
Chronic limb threatening ischaemia (CLTI) represents the most advanced stage of peripheral artery disease (PAD), which if left untreated, can progress to ulceration, gangrene, sepsis, major lower extremity amputation (LEA) and premature death.1,2 Despite initial high rates of technical success (> 90%), infrainguinal percutaneous transluminal angioplasty (PTA) is plagued by high restenosis rates because of elastic recoil 3 and barotrauma caused by intra-arterial ballooning, leading to the development of neointimal hyperplasia (NIH). 4 Acute vessel damage is frequently seen in non-compliant calcified atherosclerotic vessels, common in those with end-stage renal failure and diabetes and may range from simple plaque rupture, flow-limiting dissection, or local perforations requiring stent placement.
Improving vessel compliance with focused force plaque fracture seems to be a promising strategy to avoid significant vessel damage. Scoring balloons were developed by exploiting the concept of precise rupture of the atheroma using microblades. The UltraScore™ balloon has only been available since 2019 and there has been no literature on its clinical experience in the peripheral vasculature to date.
Devices coated with paclitaxel and with rapamycin analogues, such as sirolimus, have been used successfully to limit restenosis by inhibiting the biologic pathway that leads to NIH. 5 Rapamycin analogues are generally perceived as superior to paclitaxel because of lower restenosis rates and higher safety margin in the coronary bed. 6 Moreover, recent attention has been drawn to a possible increase in late mortality and lower amputation-free survival (AFS) 7 in patients receiving paclitaxel-coated devices for peripheral arterial disease.
Inherent in Asian arteries is the small vessel calibre with poor luminal gain after standard conventional balloon angioplasty (CBA). The atherosclerotic lesions are often long, complex and calcified with significant early recoil. Although drug-coated balloon (DCB) angioplasty technology may have the potential to mitigate the NIH response, their benefit in addressing the problem of acute recoil is doubtful. To lower the restenosis risk due to early recoil, literature suggests that vessel preparation with prolonged angioplasty using the UltraScore balloon may allow more controlled dissection of calcified lesions and create clefts within the atheromatous plaque to allow better drug absorption into the adventitia and may help achieve sustained luminal gain for successful wound healing. 8 By fracturing the plaque twice, combination therapy with scoring balloon followed by sirolimus-coated balloon angioplasty theoretically leads to more marked proliferative response to the acute trauma caused by balloon angioplasty. However, inhibition of mammalian target of rapamycin (mTOR) by the sirolimus-FKBP12 complex in endothelial cells gives rise to coordinated and controlled cell proliferation by integrating signals from the PI3K/AKT pathway mediated by mTOR. This ultimately leads to less restenosis within the NIH process.
The aim of this case series was to document our early experience using the UltraScore Focused Force PTA balloon in combination with Selution SLR™ (M.A. MedAlliance SA, Nyon, Switzerland) balloon catheter, in the setting of CLTI.
Case reports

(a) Baseline angiography showed TransAtlantic Inter-Society Consensus II C SFA lesion. The TransAtlantic Inter-Society Consensus II C lesion of the SFA was prepared with 5.0 × 200 mm2 UltraScore focused force scoring balloon at (b) 2, (c) 4, and (d) 10 atm at 30 s interval. (e, f) Subsequent angioplasty using DCB Selution SLR 5.0 × 100 and 5.0 × 150 mm2 was done at nominal pressure for 2 min each. (g) Completion angiography after scoring balloon and DCB angioplasty resulted in less than 30% residual stenosis and a lasting angiographic result after 3 months.
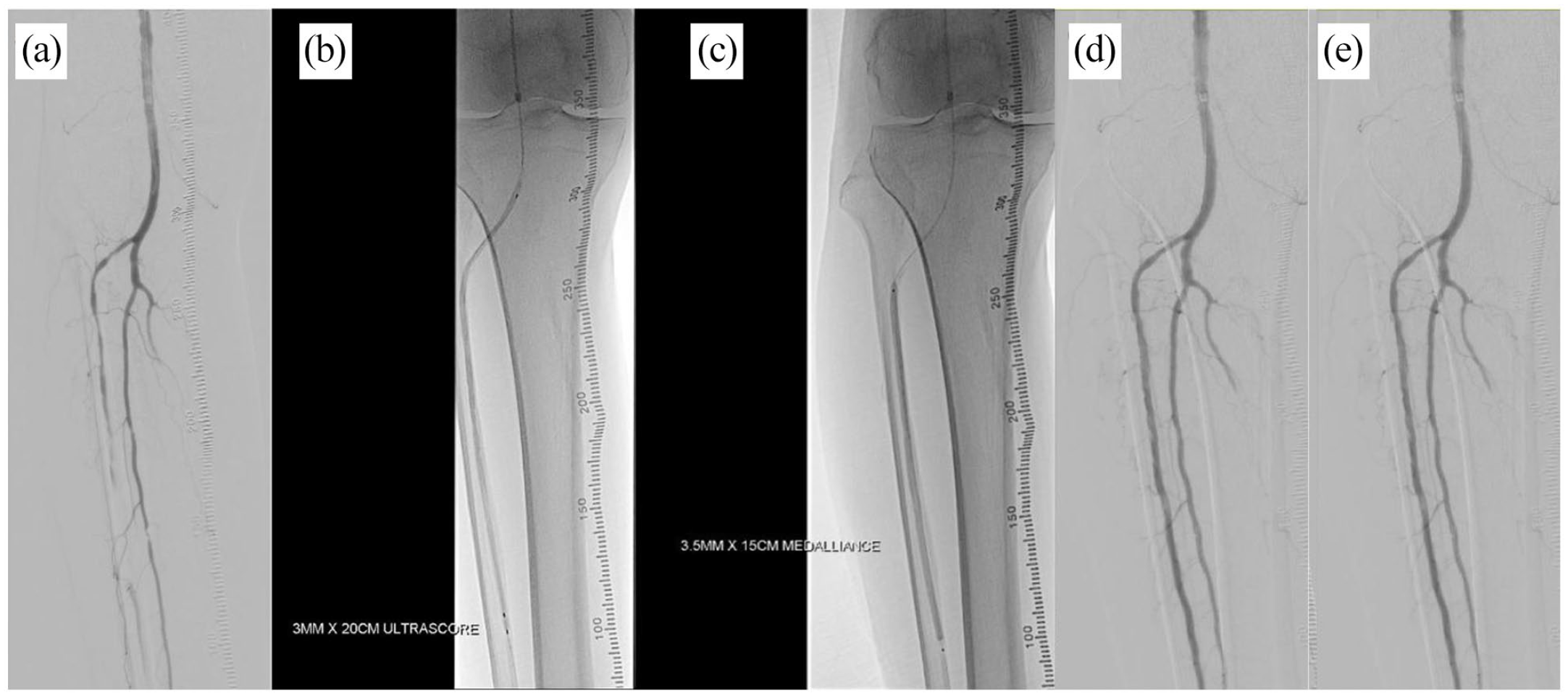
(a) Baseline angiography showed TransAtlantic Inter-Society Consensus II C anterior tibial and peroneal artery lesion. ATA lesion preparation with (b) UltraScore focused force PTA balloon 3 × 200 mm2 with inflation slowly to 14 atm for 3 min followed by (c) DCB angioplasty (Selution SLR 3.5 × 150 mm2) at 10 atm for 2 min. Completion angiography after (d) ATA UltraScore and Selution DCB angioplasty and (e) peroneal artery PTA balloon and Selution DCB angioplasty.
Discussion
Several factors need to be considered when deciding whether to revascularize a patient or the strategy to be employed to achieve this end – age, comorbidities, clinical presentation, lesion location, length and severity. However, the more prognostic factors of outcome include the presence and extent of tissue injury and wound infection severity as encapsulated by the WIfI classification system. The WIfI classification system is an important factor which allows accurate staging of the severity of limb threat with high predictive value of 1-year amputation risk and potential benefit from revascularization. 9 Moreover, it has been shown in recent studies to be a stronger predictor of diabetic foot healing than the angiosome concept approach. 9 de Athayde Soares et al. 10 demonstrated that WIfI classification 0–1 is associated with faster and higher wound healing rates than WIfI classification 2–3. For our two cases, the WIfI classification indicates a moderate risk of major amputation at 1 year with medical therapy alone and a moderate to high benefit from revascularization according to the Delphi Consensus.
These cases demonstrate the synergistic effect of lesion preparation with scoring balloon followed by sirolimus DCB in both femoropopliteal and below the knee regions. There are several different scoring systems on the quantification of vascular calcification. Frequently cited calcium scales include PACSS and Peripheral Academic Research Consortium (PARC). In our study, the grade of vascular calcification according to PACSS was 4 for both cases, indicating that these are lesions with high degree of calcium. As successful as modern endovascular interventions in achieving revascularization, vessel wall calcification is associated with increased procedural complications and long-term treatment failure. 8 It not only makes navigating guidewires across the stenosis/occlusion difficult, the decreased compliance of calcified vessels also leads to more acute vessel recoil and requires higher pressures for balloon expansion during angioplasty, increasing the risk of arterial wall dissection and perforation. Dissection is managed usually by stent placement, which carries the risk of poor expansion, malposition and fractures due to the calcification. 8 Moreover, Fanelli et al. 11 demonstrated that vessel wall calcification appeared to decrease the efficacy of DCBs by reducing the absorption of antiproliferative agents, while de Athayde Soares et al. 12 reported worse primary patency rates for femoropopliteal lesions of PACSS grade > 2. The potential benefit of scoring technology to create deeper clefts within the calcium barrier to facilitate drug absorption and the newer transfer technology of sirolimus-eluting balloons may improve the efficacy of drug absorption into the arterial wall and allowing longer vessel patency.
By concentrating force at the scoring element, scoring balloons have been shown in vitro to apply a threefold higher stress to the calcified plaque and induces cracks at lower inflation pressures. 13 This decreases rates of dissection and bailout stenting. The semi-compliant scoring balloons may be enveloped by helical (Angiosculpt™; Philips, San Diego, US) or triangular scoring elements (Non-slip element (NSE) Alpha™; Braun, Melsungen, Germany) or longitudinal wires (UltraScore; BD Interventional, New Jersey, US) and embedded with a rigid polymer (Advance Enforcer™; Cook Medical, Limerick, Ireland) or serrated strips (Serranator Alto™; Cagent Vascular, Wayne, USA). The first scoring balloon was the AngioSculpt Balloon Catheter developed in 2003 for the treatment of complex coronary disease. It has subsequently been evaluated for the treatment of infrapopliteal disease and more recently, with the development of longer devices, for SFA disease and stenosis involving haemodialysis fistulae. It has shown sustained benefit in achieving limb salvage in patients with CLTI up to 1 year after treatment with low dissection rates, no perforations and no significant device slippage. 14 The most cited registry on scoring balloons is the single-centre PANTHER registry which examined the treatment of femoropopliteal lesions with the Angiosculpt scoring balloon. 15 It included 124 calcified de novo and restenotic lesions in 101 consecutive patients with claudication (65.3%) and critical limb ischaemia (34.7%). Three arms were investigated. The first arm included lesions treated by scoring balloon alone (37.1%), the second scoring balloon followed by drug-eluting balloon (32.3%), and the third scoring balloon plus stent deployment (30.6%). The primary patency rate was 83.9% at 12 months. When stratified by calcification severity, there was no difference in patency rates among the groups. This suggests that calcification severity does not affect patency in the setting of scoring balloon use.
In the recently published PRELUDE-BTK study evaluating the safety and efficacy of the Serranator PTA balloon, device success was 91.7% and freedom from major adverse limb events and perioperative death through 30 days was 95.7%. Pretreatment stenosis of 82% was reduced to 21.8% and only 1 (1.9%) grade D dissection occurred requiring bailout stenting. 16 Karashima et al. 17 investigated the NSE balloon in the treatment of femoropopliteal lesions and noted fewer severe dissections (8.8% vs 29.7%, p = 0.027) and shorter total dissection length (11.5 ± 12.8 vs 35.7 ± 24.1 mm, p = 0.027) with lower bailout stenting rate (17.6% versus 40.5%, p = 0.035) compared to CBA. The Advance Enforcer PTA balloon catheter has only been investigated in treating stenosis of mature arteriovenous (AV) haemodialysis access circuits.
Meta-analyses of paclitaxel-coated devices have revealed increased risk of major amputation and late mortality compared to bare devices, possibly from long-term, low-level exposure to the cytotoxic drug.7,8 This finding has led to a significant dampening of enthusiasm for their use. 18 Sirolimus and its analogs are alternative antiproliferative agents for DCB and are supported by solid clinical evidence in terms of safety and efficacy as seen in coronary drug-eluting stents. 8 The hydrophilic nature of sirolimus meant drug retention in the vessel wall and sustained release was a major challenge. Recently, encapsulating sirolimus in micro-reservoirs has facilitated the development of effective sirolimus DCBs. To date, there are three commercially available sirolimus DCB – MagicTouch™ (Concept Medical), Selution (Med Alliance) and Virtue™ (Orchestra BioMed). The coating formulation of the Selution DCB consists of four excipients. The first excipient is a biodegradable polymer poly(lactic-co-glycolic acid) intermixed with the sirolimus to form micro-reservoirs, regulating drug release through matrix degradation. The remaining three excipients constitute a phospholipid blend that reduces drug wash off in the bloodstream during insertion and lesion crossing, optimizes drug transfer during short-term balloon dilatation and adheres the micro-reservoirs to the tissue after the Selution DCB is deflated. The PRESTIGE study looked at the use of Selution DCB in patients with CLTI for TASC-II C and D tibial occlusive disease. At 6 months, primary patency was 81.5%, freedom from Target Lesion Revascularization (TLR) was 83.3%, AFS was 84.0%, and wound healing was 81.0%. 19 Outcomes of freedom from TLR, AFS and wound healing were sustained at 12 months. This is highly promising particularly when compared to SINGA-PACLI trial which looked at a paclitaxel DCB in BTK patients and showed patency of just 43% at 6 months. 20
In accordance with the ESVS Global Vascular Guidelines on the Management of Chronic Limb-Threatening Ischemia and the recommendations from the Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, Case 1 had advanced limb-threatening ischaemia (WIfI Stage 3) and high complexity of disease (GLASS Stage 3) and would be a suitable candidate for open surgical bypass. 21 However, the fact that combination endovascular therapy with scoring and sirolimus-coated balloon gave good outcomes with sustained primary patency at 4 months demonstrates that endovascular revascularization could be a feasible option for selected high-risk patients.
Conclusion
Scoring and sirolimus drug-eluting balloons have synergistic effect when used in tandem, especially for calcified arterial lesions, and demonstrates good technical and procedural success. A randomized trial of scoring balloon followed by DCB angioplasty versus conventional balloon and DCB angioplasty powered to look for long-term clinical benefits is required to fully answer the question as to the true efficacy of this novel technique.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: T.Y.T. has received speaking honoraria and physician-initiated grants from Bard BD and MedAlliance.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Guarantor
T.Y.T.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.