
Abstract
Objectives
Abdominal aortic aneurysms are conventionally treated by open repair surgery. While endovascular aortic repair improves survival in high-risk patients, younger patients (40–65 years) potentially at lower risk with asymptomatic abdominal aortic aneurysms undergoing endovascular aortic repair usually have poorer post-operative outcomes and require longer term follow-up. In this study, clinical data on younger patients were analyzed to investigate whether endovascular aortic repair leads to poorer short- and long-term outcomes.
Methods
This was a systematic review and meta-analysis of articles comparing clinical outcomes in patients aged 40–65 years undergoing open repair or endovascular aortic repair and published between 2000 and 2017. In-hospital mortality, long-term mortality, and post-operative complication data were retrieved from eligible studies and clinical outcomes were compared. Twenty-one retrospective cohort analyses were included, accounting for 250,837 patients (149,051 endovascular aortic repair; 101,786 open repair). Risk ratios were pooled using the DerSimonian and Laird random effects model. All statistical analyses were performed in Review Manager 5.3.
Results
Younger patients with asymptomatic abdominal aortic aneurysms undergoing endovascular aortic repair had a significantly reduced 30-day mortality (odds ratio (OR) = 0.40, 95% confidence intervals (CI) 0.28–0.57; p < 0.00001), long-term mortality (OR = 0.37, 95% CI 0.17–0.82; p = 0.01), incidence of reintervention (OR = 0.47, 95% CI 0.34–0.66; p < 0.0001), and incidence of renal failure (OR = 1.58, 95% CI 1.37–1.82; p < 0.00001).
Conclusions
Endovascular aortic repair may improve short- and long-term survival and reduce post-operative complications in younger patients with asymptomatic abdominal aortic aneurysms.
Keywords
Introduction
The surgical management of abdominal aortic aneurysms (AAA) aims to prevent aortic rupture, which is associated with a mortality rate of up to 80% and causes 9000 deaths every year in the United States.1,2 There are two main surgical strategies for patients with asymptomatic AAA: open repair (OPEN) and endovascular repair (EVAR). Over the last 15 years, EVAR has become the most widely used surgical modality for patients with AAA, accounting for 78% of all surgeries performed on patients with AAA in the United States.3–5
EVAR has a number of advantages over OPEN: decreased perioperative mortality, reduced length of stay in the intensive care unit, and earlier recovery. 6 Therefore, EVAR is generally indicated in older, high-risk patients and those deemed “unfit” for OPEN.7,8 However, patients undergoing EVAR require more frequent reassessments and are usually at higher risk of reintervention.9,10
Several studies have compared clinical outcomes from these surgical procedures in elderly/octogenarian patients, which show that the short-term clinical benefit of EVAR to patients older than 50 years is higher than that from OPEN.11–13 Nevertheless, it is still debated whether EVAR has poorer long-term outcomes in patients with asymptomatic AAA.7,8 Schwarze et al. showed that younger, middle-aged patients (40–65 years) have a reduced risk of perioperative death and morbidity compared to elderly patients with AAA undergoing either OPEN or EVAR. 14 Sirignano et al. reported that OPEN or EVAR are safe and have comparable short- and long-term clinical outcomes in middle-aged patients with AAA undergoing elective surgical repair. 15 Nevertheless, variable long-term outcomes and higher reintervention rates for EVAR have led not to perform this procedure in middle-aged patients.
This prompted us to conduct a systematic review and meta-analysis to quantify the clinical benefit of undergoing EVAR or OPEN in middle-aged patients (40–65 years) with asymptomatic AAA. In particular, differences in 30-day and long-term mortality between EVAR and OPEN patients and post-operative complications including reintervention and renal failure were assessed.
Patients and methods
Literature survey
A literature survey of the PubMed, EMBASE, Scopus, Science Direct, Web of Science, Cochrane Library, and China National Knowledge Infrastructure (CNKI) databases was performed to retrieve relevant full research papers published between 2000 and 2017. The following search terms were deployed to identify relevant studies: “asymptomatic AAA”, “EVAR/OPEN elective surgery”, “younger patients”, “middle-aged patients”, “less/younger than 65 years old”. No language restrictions were applied. Additional papers were also found from the reference lists of the articles retrieved. The “Preferred Reporting Items for Systematic Reviews and Meta-Analyses” (PRISMA) were strictly followed throughout this study. 8
Selection criteria
Prospective and retrospective original research studies reporting data on patients aged between 40 and 65 years of age with asymptomatic AAA undergoing either OPEN or EVAR surgical procedures were considered for inclusion. However, due to study heterogeneity, some patients beyond the target range of 40 to 65 may have been included; nevertheless, an average age within such pre-defined range in the patient cohorts considered was ensured. Each study had to include and report clinical outcomes for two cohorts of patients: the first undergoing EVAR and the other undergoing OPEN. The primary endpoints were: (i) 30-day mortality; (ii) long-term mortality; (iii) incidence of reintervention; and (iv) incidence of renal failure.
Studies reporting data on patients undergoing repair surgery for AAA rupture or symptomatic AAA were excluded from the analysis due to their considerably higher short-term mortality than patients with asymptomatic AAA. 16 Case reports, case series, and conference abstracts were also excluded from the analysis. Further to the completion of a first selection of full-length journal papers, duplicate articles were removed. The titles and abstracts of the remaining articles were reviewed by two independent investigators responsible for determining whether the articles, based on the above-mentioned criteria, were eligible for inclusion. To eliminate inconsistencies, the investigators compared the lists of articles prior to reviewing the full text of the studies identified as eligible. When the final list of studies was complete, a third investigator resolved any discrepancies.
Data collection and quality assessment
A standardized, custom-written Microsoft Excel spreadsheet was used to extract all relevant data on the research design of the studies of interest, inclusion and exclusion criteria, sample size, baseline characteristics of the patient population, and short- and long-term clinical outcomes.
The scientific rigor and quality of the observational studies included in the analysis were assessed using the nine-point Newcastle-Ottawa scale, which attributes points to articles based on the selection procedure(s) adopted (0–4 points), comparability (0–2 points), and identification of the outcomes of the participants in the study (0–3 points).
Statistical analysis
All statistical analyses were performed using “Review Manager (REVMAN) 5.3 Copenhagen” (The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). Pooled results were computed as odds ratios (ORs) with 95% confidence intervals (CI) to summarize categorical data and means for continuous data. Publication bias was qualitatively assessed via funnel plots and quantified with Egger’s test. A qualitative estimate of statistical heterogeneity between studies was evaluated using the Cochrane Q statistic. For the χ2 test, a p-value less than 0.05 was considered statistically significant. The I2 statistic was deployed to quantify the extent and significance of heterogeneity and was interpreted based on the Cochrane criteria, whereby 25%, 50%, and 75% correspond to low, medium, and high levels of heterogeneity, respectively.
Results
Literature survey
The systematic survey of the major electronic scientific and medical literature databases between 2000 and 2017 returned 4489 articles. After reviewing the titles and abstracts, 3873 studies were excluded, with 616 studies retained for further detailed evaluation. Based on the inclusion and exclusion criteria, 595 studies were excluded, leaving 21 (n = 21) cohort studies11–15,17–32 reporting clinical data of interest and meeting the inclusion criteria (Figure 1).
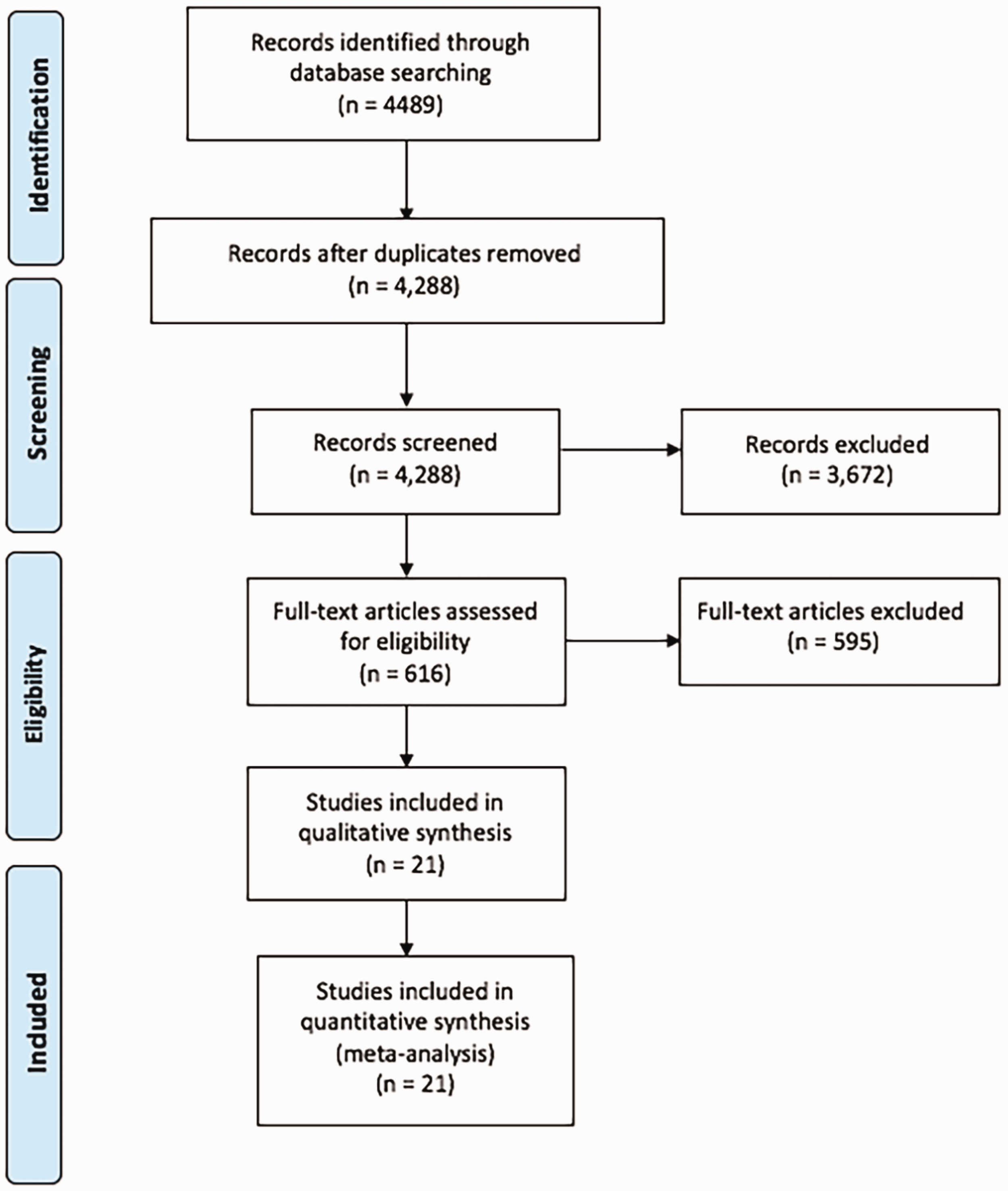
Flow chart presenting the selection process of eligible studies.
Study characteristics
The main characteristics of the included studies are summarized in Table 1. All 21 included studies were retrospective cohort analyses. A total of 250,837 patients with asymptomatic AAA were considered, 149,051 of whom had undergone EVAR (59.42%) and 101,786 OPEN surgery (40.58%). Most of the clinical data analyzed were derived from a single retrospective analysis reporting data on 99,211 patients. 28 One of the included studies reported experiences later than 2000 but included commercially available endografts implanted between 1994 and 2007 for research. 18 A comparison dated back from 1994 to date enables to normalize per type of device used, thus providing a more unbiased statistical snapshot of whether EVAR is a beneficial surgical intervention for the cohort of patients considered.
Main characteristics of the studies included in the analysis.
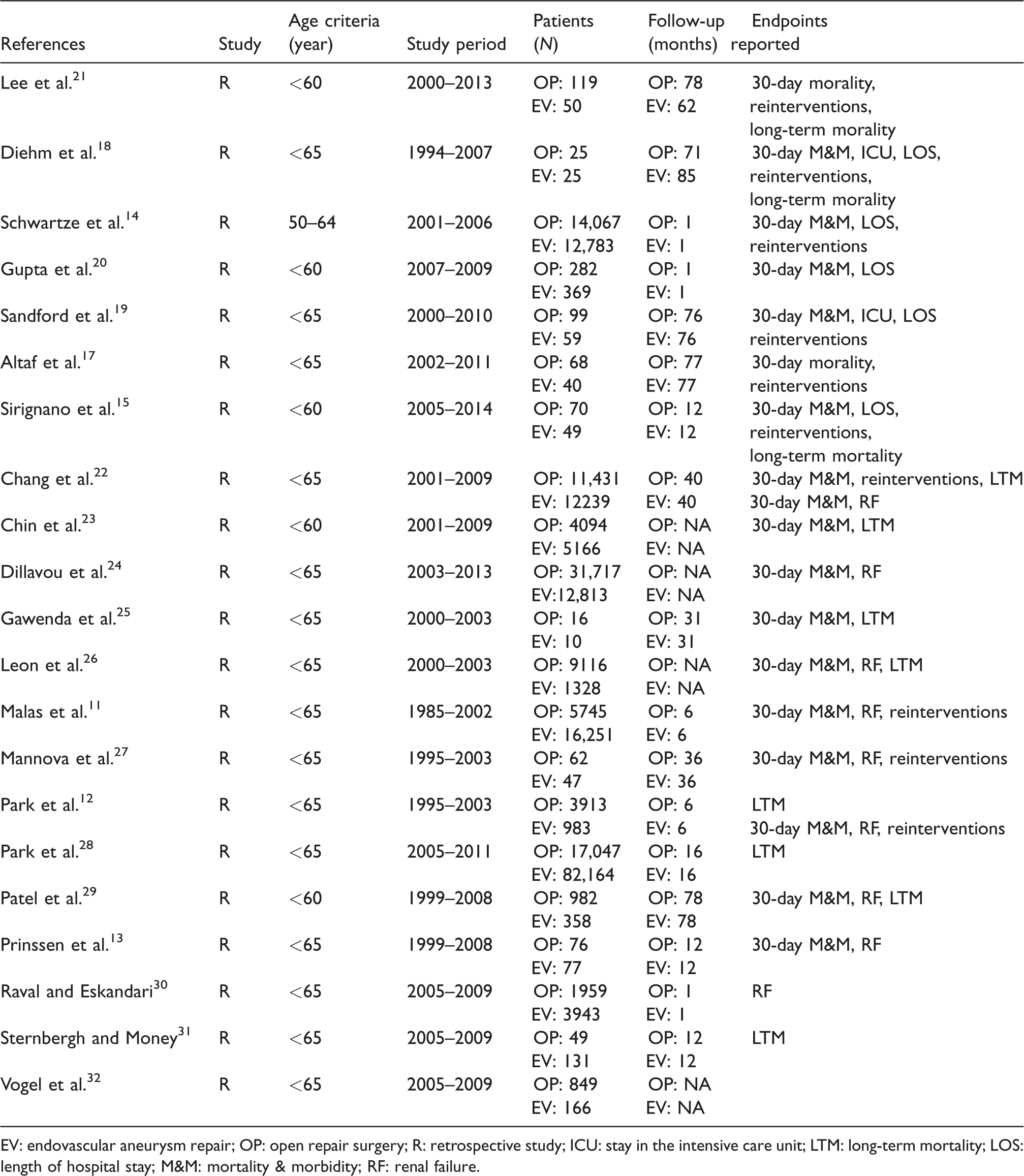
EV: endovascular aneurysm repair; OP: open repair surgery; R: retrospective study; ICU: stay in the intensive care unit; LTM: long-term mortality; LOS: length of hospital stay; M&M: mortality & morbidity; RF: renal failure.
The definition of “younger patients” was not consistent in the included studies, but the mean (±standard error) age of the included patients was from 40 to 65 years. Furthermore, to ensure an adequate sample size of patients being considered in this meta-analysis for deriving statistically meaningful conclusions on whether EVAR or OPEN would be the recommended surgical procedure for younger patients with asymptomatic AAA, the duration of follow-up varied between the selected studies and ranged from 30 days14,20,30 to 75.5 months.
The overall incidence of reintervention was 0.98% in patients undergoing EVAR (n = 937 out of 95,926 patients) and 1.93% in patients undergoing OPEN (n = 636 out of 32,949 patients). The incidence of renal failure was 8.16% in patients undergoing EVAR (n = 8880 out of 108,772 patients) and 8.50% in patients undergoing OPEN (n = 280 out of 32,961 patients). Baseline characteristics of the included studies are presented in Table 2.
Main baseline characteristics of patients retrieved from representative studies.
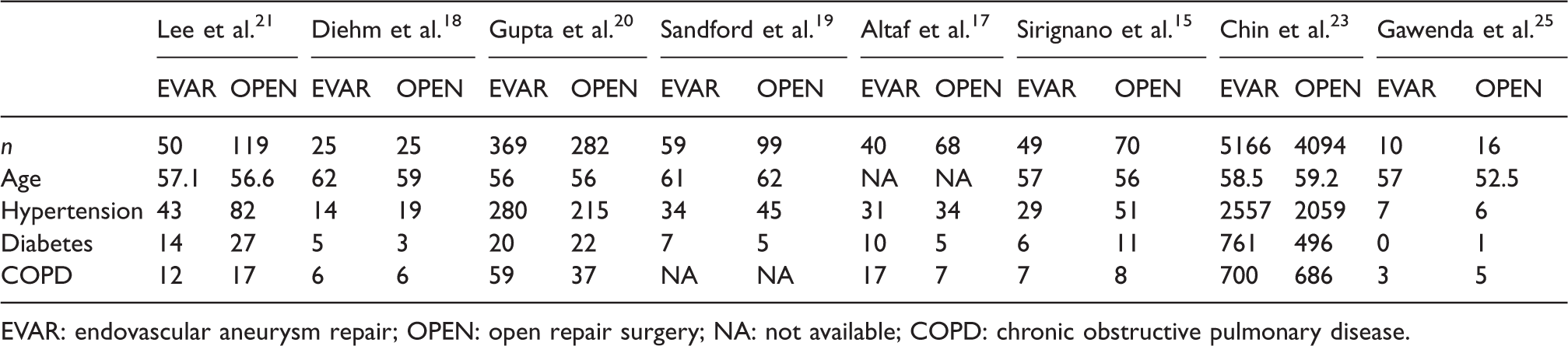
EVAR: endovascular aneurysm repair; OPEN: open repair surgery; NA: not available; COPD: chronic obstructive pulmonary disease.
Immediate perioperative outcomes
Thirty-day mortality data were extracted from 18 studies (n = 248,302 patients) and the risk of mortality was significantly lower in patients with asymptomatic AAA undergoing EVAR than those undergoing OPEN (OR = 0.40; 95% CI: 0.28–0.57; p < 0.00001; Figure 2). There was no evidence of significant heterogeneity amongst the studies considered (I2=0%, p = 0.62).
Forest plot of mean differences in 30-day mortality in patients with asymptomatic abdominal aortic aneurysm (AAA) treated via an open repair (OPEN) surgical procedure or endovascular aortic repair (EVAR) via stent grafting. Raw differences in means are estimated with a random effects model.
Long-term outcomes
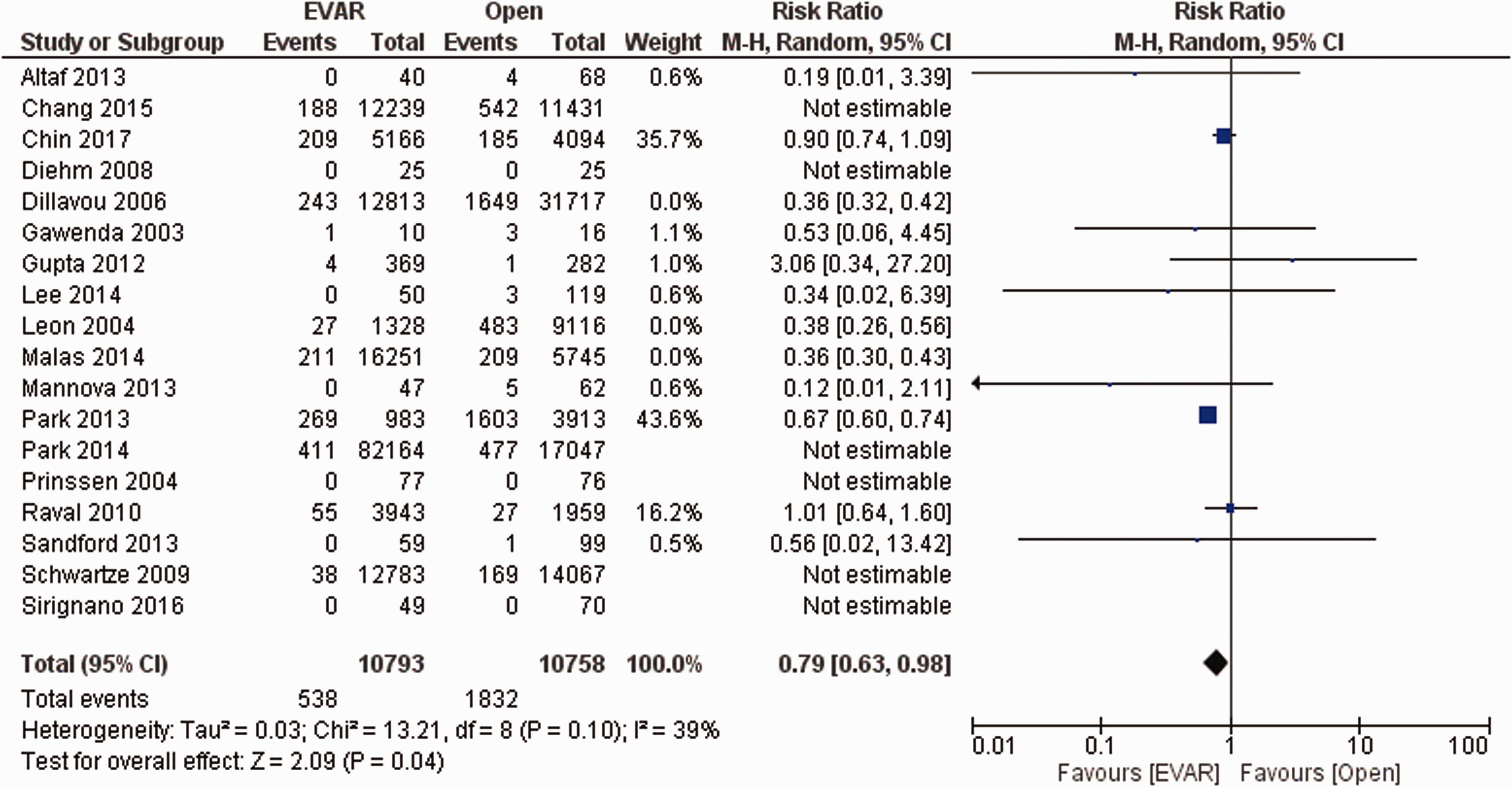
Follow-up ranged from 30 days to 75.5 months, and long-term reintervention data were extracted from eight studies (n = 128,875 patients). As illustrated in Figure 3, reinterventions were significantly less common in patients undergoing EVAR than those undergoing OPEN (OR = 0.47; 95% CI: 0.34–0.66; p < 0.0001) and there was no significant heterogeneity (I2=50%, p = 0.08). Heterogeneity bias was overcome further to a sensitivity analysis, thus selecting the maximum number of studies per each of the events sought for evaluation that would have yielded statistically meaningful and reliable results.
Forest plot of mean difference in reinterventions in patients with asymptomatic abdominal aortic aneurysm (AAA) either treated via an open repair (OPEN) surgical procedure or endovascular aortic repair (EVAR) via stent grafting. Raw differences in means are estimated with a random effects model.
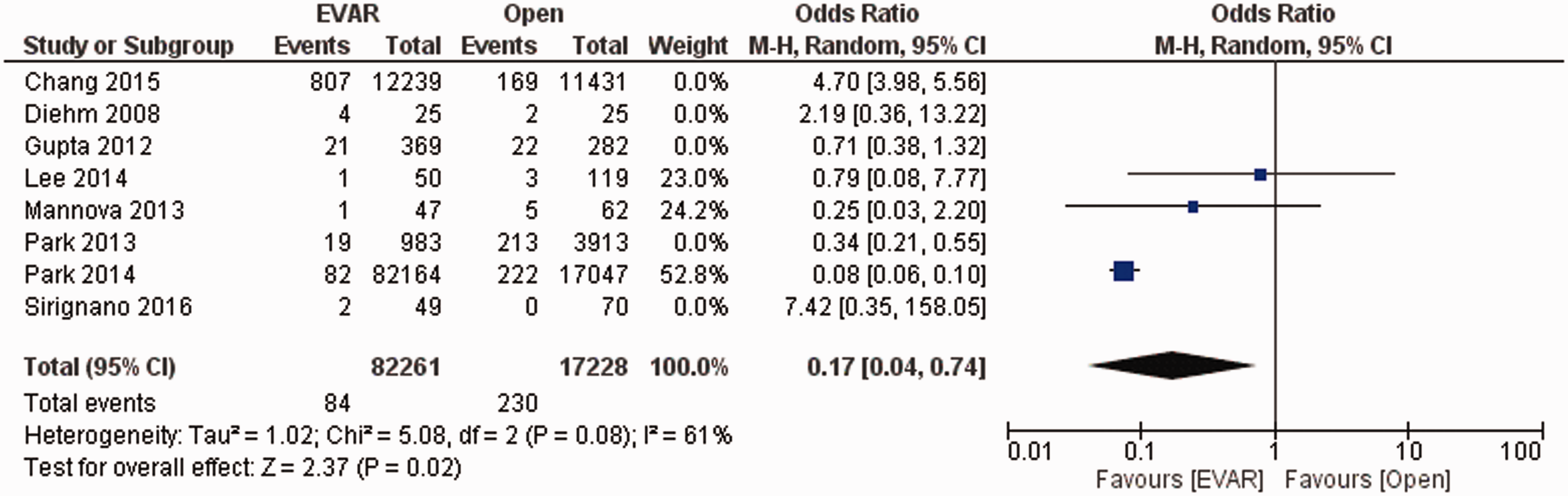
Long-term mortality data were extracted from 13 studies (n = 135,340 patients) and was significantly lower in patients undergoing EVAR (OR = 0.37; 95% CI: 0.17–0.82; p = 0.01), with no evidence of significant heterogeneity (I2=48%, p = 0.08; Figure 4).
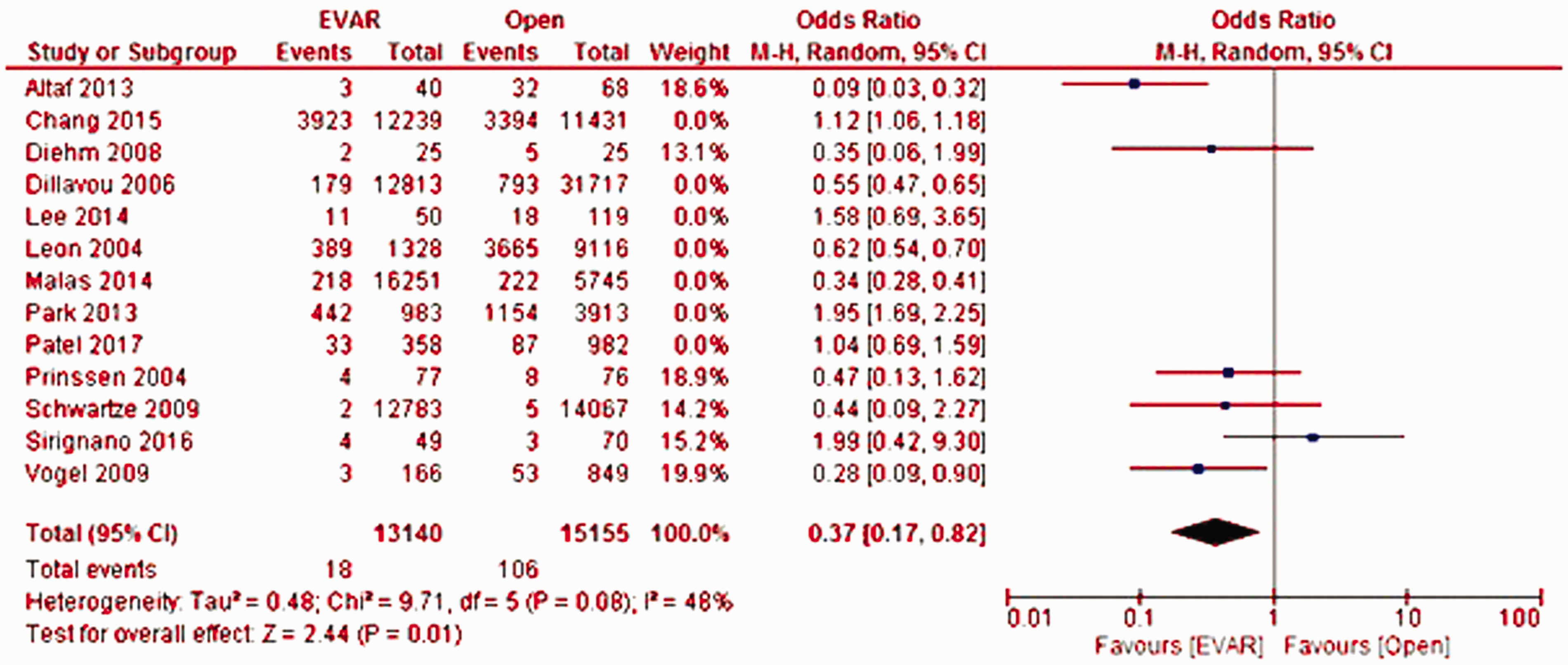
Forest plot of mean difference in long-term mortality in patients with asymptomatic abdominal aortic aneurysm (AAA) either treated via an open repair (OPEN) surgical procedure or endovascular aortic repair (EVAR) via stent grafting. Raw differences in means are estimated with a random effects model.
Data on the incidence of renal failure were extracted from nine studies (n = 141,733 patients), which was significantly lower in patients undergoing EVAR (OR = 1.58; 95% CI: 1.37–1.82; p < 0.00001), with no evidence of significant heterogeneity (I2=38%, p = 0.14; Figure 5).
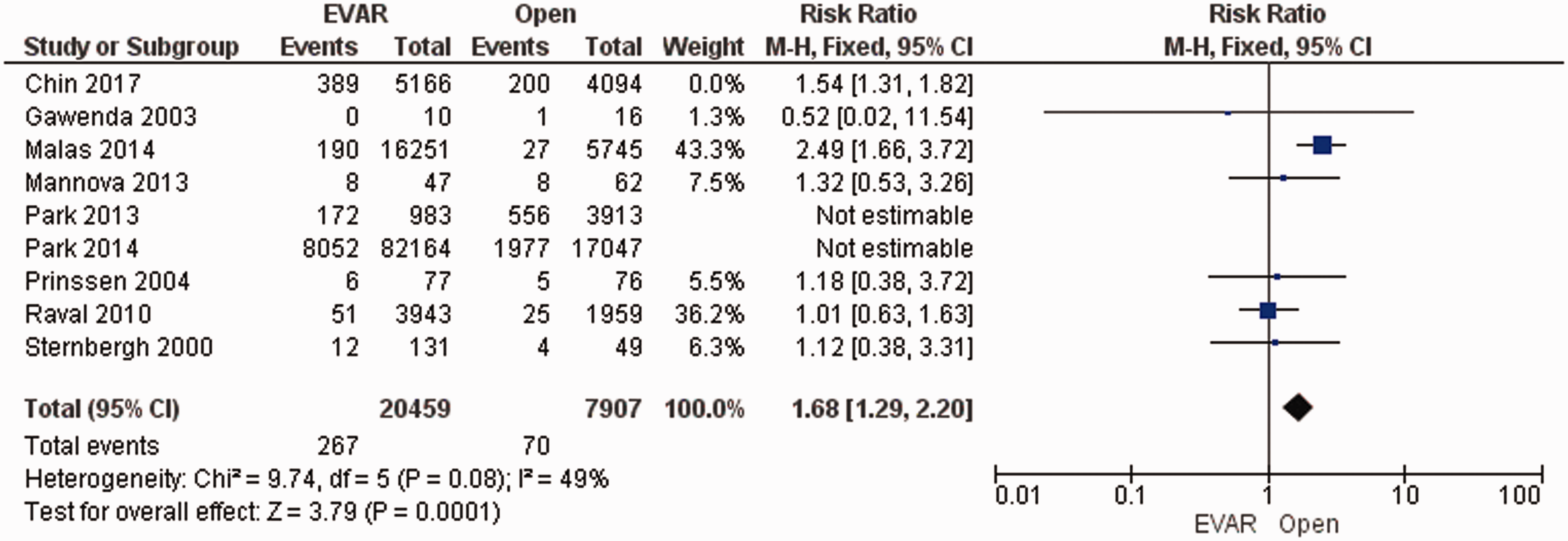
Forest plot of mean difference in incidence of renal failure in patients with asymptomatic abdominal aortic aneurysm (AAA) either treated via an open repair (OPEN) surgical procedure or endovascular aortic repair (EVAR) via stent grafting. Raw differences in means are estimated with a random effects model.
Discussion
Surgery is typically recommended when the aneurysm diameter is greater than 5.5 cm in men and 5.0 cm in women. 4 AAAs may be repaired either via OPEN or EVAR procedures. After 2003, EVAR became the treatment of choice for AAA, replacing OPEN as the most common surgical intervention for AAA repair. 33 Recently, Davidovic et al. 34 showed that short-term mortality after OPEN surgical repair of AAA in high-volume centers with highly experienced anesthesiologic and surgical teams might be very low. Furthermore, in the same study, 34 OPEN improved clinical outcomes in patients with a hostile abdomen, unsuitable anatomy, or young patients. However, this study 34 did not directly compare clinical outcomes with EVAR, as it only included patients undergoing OPEN. While patients with AAA undergoing EVAR typically have a better short-term survival and reduced length of hospital stay than patients undergoing OPEN, EVAR may have detrimental long-term clinical outcomes.7,35 However, analyzing results from large randomized clinical trials up to 2014, Paravastu et al. did not find any discrepancies in long-term clinical outcome between the two cohorts of patients. 36
Several studies have shown that patients treated with EVAR have a higher incidence of long-term reintervention. 37 AAA affects between 2 and 8% of males over 65 years. Considering that long-term outcomes between patients undergoing OPEN and EVAR are comparable, 38 we hypothesized that EVAR would be more beneficial in younger patients aged between 40 and 65 years), so this study aimed to quantify the clinical benefit from undergoing EVAR compared to OPEN in younger patients with AAA.
We showed that younger patients with asymptomatic AAA undergoing EVAR had better short- (30-day) and long-term survival and significantly reduced incidences of long-term reinterventions and renal failure than younger patients with asymptomatic AAA undergoing OPEN. Such outcomes disagree with previous studies as this meta-analysis comprehensively included research since 1994, thus from the beginning of the commercialization of EVAR grafts to date, thus resulting in unbiased findings. Such results are, thus, related to the surgical intervention itself, rather than relying on the type of device used. Therefore, EVAR seems to be superior to OPEN for younger patients with asymptomatic AAA.
However, this study has a number of limitations. We only considered data from retrospective studies due to the constraint of the relatively young age of the population of interest (40–65 years). Furthermore, most studies considered a relatively small sample size, except for one study, 14 and newer grafts may influence the long-term outcomes reported.
In contrast to some other studies,39,40 patients undergoing OPEN had a higher incidence of long-term reinterventions due to higher risk associated with such patients, the more complex epidemiology in such a cohort of subjects, along with the higher invasiveness of the procedure. Besides its minimal invasiveness, new generation EVAR grafts, such as the EndoAnchors used to treat intra-operative endoleaks, may not only reduce perioperative complications 41 but also the incidence of reinterventions as compared to patients undergoing OPEN surgery. Since this technology might bias the comparison of clinical outcomes between EVAR and OPEN, the likelihood of a prospective clinical trial in this arena is quite low, at least at present. Furthermore, the hospital costs associated with EVAR are still higher than OPEN, with the device costing over $5000. 31 However, as EVAR becomes more widely adopted,42–44 despite its potential complications 45 and current associated costs, 46 the technology is expected to become much cheaper over time, making it not only a safer but also a more affordable treatment in the future and contributing to a wider adoption.
Since the long-term outcomes of atypical use of EVAR with respect to the international and UK AAA guidelines47,48 are still largely undocumented, this topic was not discussed as we could not deal with it in sufficient detail in this study. Therefore, the use of such an aggressive approach must be considered against the likely clinical benefit derived from adopting it, for which there are currently no clinical guidelines/recommendations.
Nevertheless, there was significant variation in duration of follow-up amongst the studies included in this systematic review and meta-analysis, which may partly explain the high heterogeneity of the short- and long-term post-operative clinical outcomes analyzed.
Conclusions
From this systematic review and meta-analysis, EVAR was shown to improve short- and long-term survival in younger patients (40–65 years) with asymptomatic AAA compared to OPEN procedures. Furthermore, there was a significant reduction in the incidences of reintervention and renal failure in these younger patients undergoing EVAR compared to those undergoing OPEN. In conclusion, considering the unbiased results with regard to the type of device used and focused, instead, on the underlying difference in the surgical procedures of interest, our findings support the use of EVAR over OPEN in younger patients with asymptomatic AAA. Future randomized clinical trials and cohort studies should focus on collecting longer term clinical outcomes in younger patients with AAA, thereby enabling us to investigate clinical benefit from EVAR further and contributing to preoperative risk stratification and treatment planning.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article