
Abstract
Image retake of radiological examinations not only increases the risk of radiation exposure of the patients, but also wastes the medical resource and degrades the quality of services of the hospitals. This study aimed at discovering factors affecting image retake of general digital radiography for setting guidelines to reduce the image retaking rate. A total of 98,503 general X-ray images retrieved from the picture archiving and communication system database of a medical center in central Taiwan were analyzed. The results showed that the total retaking rate was 4.89% with the position error (56.05%) was the main factor causing image retakes and chest examination showed the highest frequency (1544 cases). On the other hand, skull/face exhibited the highest retaking rate (9.81%) among various types of examinations. After discovering the factors affecting the image retaking rate, suitable guidelines were proposed and introduced. The image retake rate had been significantly reduced to 4.38% and 3.57% 1 month and 6 months, respectively, after the introduction of guidelines. In conclusion, image retake analysis is a quality indicator and is effective for quality assurance of digital radiology. Regular analysis of image retake can find factors inducing image retake and is useful for designing guidelines to reduce the image retake rate.
Introduction
The image retake rate of traditional film-based radiography was reported to be as high as 10%–15% due to incorrect exposure caused by limited dynamic range.1,2 After the introduction of digital radiography (DR), the retaking rate has been reduced to 5.5% in the United Kingdom3,4 and 5% in Australia and the United States.5,6 Some studies still exhibited high retaking rate in DR; as reported in the studies recently conducted in Norway7,8 and the United States, 9 the retaking rates were as high as 11%–12% and 8%–10%, respectively.
Image retakes of X-ray examinations impose patients to unnecessary ionizing radiation, which was suspected to have great risk in inducing cancer, 10 even at protracted low-dose exposure. 11 However, it is widely believed that the benefits outweigh the risks for medical imaging examinations, except the cases involving redundant examinations. 12 Therefore, decreasing image retakes is crucial in reducing X-ray exposure and inconvenience of patients, as well as in avoiding wasting of medical resources for quality assurance of a hospital.2,9,13
In this study, we analyzed the images stored in the picture archiving and communication system (PACS) database to discover factors affecting the image retake of general digital radiology. And then, appropriate strategies and guidelines, such as training technicians to improve their positioning skills and providing signs, marks, and hints onsite to ensure proper positioning, avoid machine operating problem, and prevent anatomy cutoff, were proposed and introduced to reduce the image retake rate for quality assurance of the hospital.
Materials and methods
Data source and analysis
Images of general DR acquired from July to December 2010 and stored in the PACS database of a university hospital located in central Taiwan area were retrieved for analysis. Among the 102,302 images retrieved from the PACS database, a total of 98,503 images were used for analysis after excluding 3822 images with uncompleted information. The images were further divided into two groups: retake image (4812; 4.89%) and non-retake image (93,691; 95.11%).
The independent variables included type of examinations, projection direction (anteroposterior and lateral), and factors causing image retake. The type of examinations was categorized into skull/face, spine, upper limb, chest, abdomen, and lower limb, whereas the factors affecting image retake were classified into position error and anatomy cutoff, artifact, patient motion, machine problem, and improper exposure.
The statistical software package SAS (version 9.1.3) was adopted for descriptive and inferential statistical analyses. In descriptive analysis, frequency was calculated for nominal variables, and then Pearson chi-square test was used for inferential statistical analysis to compare difference between the two groups. The level of significance was defined as p < 0.05.
Guidelines for reducing image retake rate
After having observed the factors affecting image retaking rate, a quality control team, consisting of senior physicians and technicians, was organized in May 2011 at the Radiological Department to propose guidelines for improving image retake rate.
After introduction of the proposed guidelines for 2 months from May to June 2011, the images collected from July to December 2011 were retrieved from the PACS database to conduct analysis of image retakes again to examine the improvement achieved. The image retake rate of each month was calculated for comparison with the retake rate before the proposed guidelines had been introduced.
Results and discussions
Factors affecting image retake
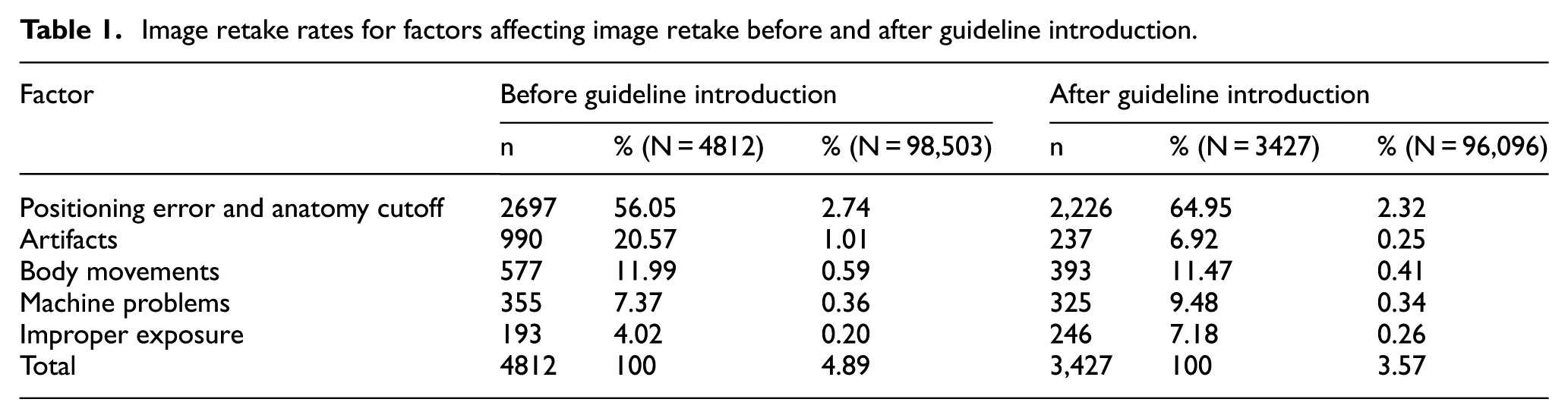
As shown in Table 1, among the 98,503 images used for analysis, 4812 (4.89%) image retakes were observed. Positioning error and anatomy cutoff (56.05%) was the most frequent factor causing image retake, followed by artifacts (20.57%), body movements (11.99%), machine problems (7.37%), and improper (over or under) exposure (4.02%). Table 2 compares the patient demography and type of examination between image retake and non-retake groups. It can be found that female patients (5.37%) had higher image retaking rate than the male patients (4.43%); elderly patients (5.93%) showed the highest retaking rate, followed by children (4.85%) and young/middle-aged patients (4.51%); and skull/facial bone (9.81%) is the type of examination having the greatest rate of image retakes, followed by abdomen (6.61%), chest (4.86%), spine (4.78%), lower limb (3.73%), and upper limb (3.55%).
Image retake rates for factors affecting image retake before and after guideline introduction.
Analysis of image retake in general X-ray digital radiography before guideline introduction.
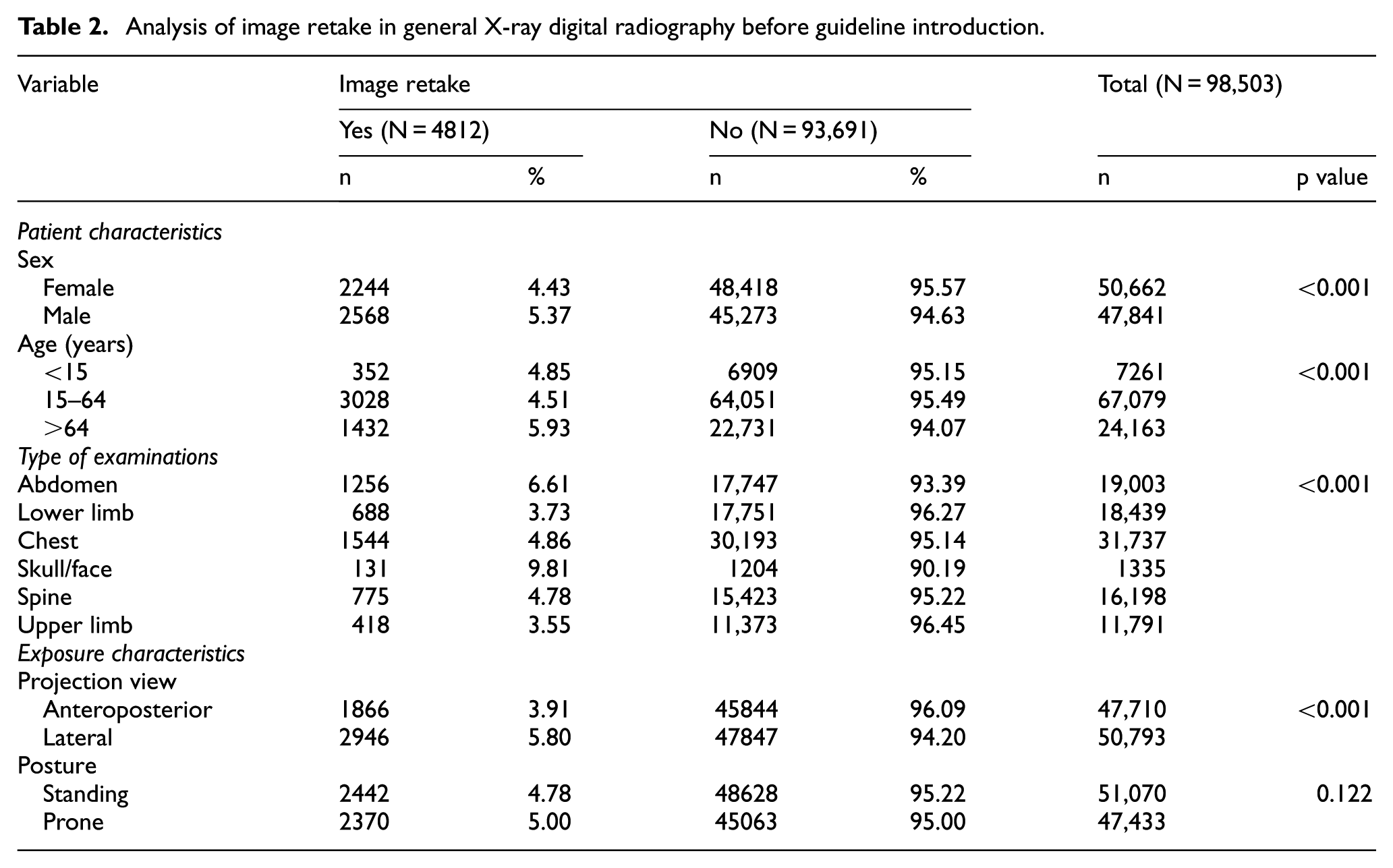
Both the demographic variables (sex and age) of patients were significantly related to image retake (chi-square test, p < 0.001). The retake rate of male patients (5.37%) was significantly higher than the female (4.43%), whereas the aged patients exhibited the highest retake rate (5.93%), followed by children (4.81%) as well as young- and middle-aged (4.51%) patients. Regarding projection view and posture, it can be found that lateral projection (5.8%) incurred significant higher image retake rate than the anterior-posterior (AP) projection (3.91%) with a level of significance (chi-square test, p < 0.001), while the image retaking rate was not significantly different between standing (4.78%) and prone (5.00%) postures (chi-square test, p > 0.05).
Proposed guidelines for reducing image retake rate
As shown in Table 3, in order to take images with good quality for reducing image retake rate, five guidelines were proposed for training less-experienced technicians to adjust patient posture and for posting at proper sites in the dressing rooms to request patients to remove artifacts or in the examination rooms to remind technicians to check machine status, to remove patients’ artifacts, and to adjust patients’ postures before examinations.
Guidelines for improving image retake rate.

As shown in Figure 1, the image retake rate had been reduced from 4.89% before guideline introduction to 4.38% in the first month and gradually to 3.57% in the sixth month after guideline introduction, resulting in a mean retake rate of 3.97% (standard deviation (SD) = 0.28%). The significantly reduced retake rate (one-sample t test, p < 0.001) demonstrates the effectiveness of the proposed guidelines. Table 1 also compares the factors affecting image retake rates after guideline introduction with the ones before guideline introduction. Except the improper exposure, the retake rates for the other factors had been decreased after guideline introduction.

Monthly image retake rates starting from July to December 2011 after having introduced the proposed guidelines for 2 months from May to June 2011.
Table 4 shows the image retake rates after guideline introduction with regard to different types of examination. Similar to the retake rate before guideline introduction, skull/facial bone (7.93%) was still the examination having the greatest rate of image retakes, followed by abdomen (5.76%), spine (3.64%), lower limb (3.57%), upper limb (2.75%), and chest (2.53%). As shown in Tables 2 and 4, the retake rates had been reduced for all types of examinations after guideline introduction.
Image retake rates for different types of examination after guideline introduction.

Discussion
As observed in this investigation, the image retake rate before guideline introduction was 4.85%, which is much smaller than the conventional radiography with a reported retake rate of 11.4% 14 and is a little smaller than the retake rates of DR found in the United Kingdom (5.5%)3,4 as well as in Australia 5 and the United States (5%). 6 Surprisingly, the retake rates observed in more recent investigations still exhibited high retaking rate in general DR; for example, the retake rates were 11%–12% and 8–10% reported by the Norway7,8 and the US 9 investigations, respectively. In this study, the image retake rate had been significantly reduced from 4.89% to 3.57% 6 months after introduction with a mean retake rate of 3.97% (SD = 0.28%) within 6 months.
Among the retake images, position error and anatomy cutoff (56.05%) is the most frequently observed factor, which is consistent to the findings reported by previous investigations; for example, 51.3% reported by Hofmann et al., 7 77% by Andersen et al., 8 and 45% by Foos et al. 6 Possible solutions for reducing image retake rate are to provide the training courses for less-experienced technicians to increase their professional knowledge and communication skills, as well as to analyze the operation workflow.15,16 As indicated in Table 3, guidelines 2, 4, and 5 had been applied for successfully reducing position error and anatomy cutoff. Table 1 shows that the retake rate caused by position error and anatomy cutoff decreased from 2.74% to 2.32% after guideline introduction, demonstrating the usefulness of the proposed guidelines.
Artifacts and body movements were the next two most frequently observed factors causing image retakes before guideline introduction. Guidelines 3 and 4 were intentionally applied to improve the image retakes caused by artifacts and body movements, respectively. Notably, as presented in Table 1 the artifact exhibits the greatest improvement with a reduction in retake rate of 0.76%, decreasing from 1.01% to 0.25% after guideline introduction. The guidelines were also effective in reducing the image retakes caused by body movement with the retake rate being decreased from 0.59% to 0.41%.
Improper exposure has been substantially reduced because of the increased dynamic range provided by the DR systems. 2 Although machine problem and improper exposure were the least occurred factors in image retake, guideline 1 was still proposed to reduce the image retakes induced by these two factors. After the guideline introduction, the image retake rate caused by the machine problem was only slightly improved (from 0.36% to 0.34%), while the retake rate induced by improper exposure did not show any improvement (from 0.20% to 0.26%). Guideline 1 needs to be refined and more education is needed for training technician to reduce retake rate caused by improper exposure.
Among different types of examination, despite its lowest retake frequency (131 cases), skull/facial bone was the examination having the highest retake rate (9.81%). In contrast, chest examination exhibited the highest retake frequency (1544 cases) with a retake rate of 4.86% only. As reported by Foos et al., 6 skull/face examination demonstrated more than 10% of retake rates in two hospitals investigated (10.55% and 15.7%), which were greater than the chest examination (9% and 8.8%). We suspected that difficulty in fixing the head and setting the proper projection angle might be the reasons causing such a high retake rate in skull/face examination. Moreover, the highest rate and lowest frequency of image retakes might be caused by the fact that skull/face examinations have been gradually replaced by computed tomography and magnetic resonant imaging, making most technicians less-experienced in performing the examinations.
Similar to previous reports, chest examination was the most frequent type of examinations performed in the investigated hospital.6–8 It was shown that the chest examination exhibited the highest frequency of image retakes, which is consistent to the investigation conducted by Andersen et al., 8 but contradicting to Hofmann et al. 7 On the other hand, as observed by Andersen et al., 8 knee examination exhibited the highest retake rate, mainly caused by position error, among all types of examinations. Hofmann et al. 7 also found that knee was the type of examination having the highest frequency and the greatest rate of image retakes with position error was the main factor causing such retakes. In contrast, our analytical results showed that skull/face bone examination had the highest retake rate, even after guideline introduction. In this study, guidelines 2 and 5 were specifically proposed to improve position errors of knee and chest examinations, respectively. After guideline introduction, the retake rates of chest and lower limb examinations had been decreased from 4.86% to 2.53% and 3.73% to 3.57%, respectively, showing the effectiveness of the proposed guidelines. Regarding the examination type, chest examination shows the greatest improvement with a 2.33% decrease in image retake rate.
Image retake analysis is deemed as a quality indicator and is useful for quality assurance of digital radiology.6,17 Regular analysis of image retake is able to find factors causing retake and useful for designing guidelines to improve the retake rate.
Conclusion
After analyzing the retake images, position error and anatomy cutoff was shown to be the main factor causing image retake, followed by artifacts, patient movements, machine problems, and improper exposure. Skull/face examination exhibited the highest retake rate compared to other types of examinations, while chest examination had the highest retaking frequency. It was also observed that the lateral projection view exhibited significantly higher retake rate than the anteroposterior view.
The guidelines for reducing image retake rate had been proposed and introduced after image retake analysis and had been shown to be effective in reducing the retake rate. Image retake analysis is a quality indicator and is effective for quality assurance of digital radiology. Regular analysis of image retake can find factors affecting image retake and is useful for designing guidelines to reduce the image retake rate.
Footnotes
Acknowledgements
C.-S.L. and P.-C.C. contributed equally to this work.
Academic Editor: Stephen D Prior
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by Ministry of Science and Technology of Taiwan (Grant Nos. MOST104-2410-H-166-005 and MOST104-2622-H-166-001) and Lin Shin Hospital (Grant No. CTU102-LS-001).