
Abstract
In this article, a neurorehabilitation system combining robot-aided rehabilitation with motor imagery–based brain–computer interface is presented. Feature extraction and classification algorithm for the motor imagery electroencephalography is implemented under our brain–computer interface research platform. The main hardware platform for functional recovery therapy is the Barrett Whole-Arm Manipulator. The mental imagination of upper limb movements is translated to trigger the Barrett Whole-Arm Manipulator Arm to stretch the affected upper limb to move along the predefined trajectory. A fuzzy proportional–derivative position controller is proposed to control the Whole-Arm Manipulator Arm to perform passive rehabilitation training effectively. A preliminary experiment aimed at testing the proposed system and gaining insight into the potential of motor imagery electroencephalography-triggered robotic therapy is reported.
Introduction
Stroke is a leading cause of disability, especially among the older people. Not only the motor system is affected after stroke, but also the cognitive systems are seriously impaired.1,2
In recent years, many different medical robots have been designed.3–7 In addition, there are a number of robot-aided rehabilitation therapy systems developed to enhance post-stroke rehabilitation of arm or hand movement and gaits (e.g. MIT-MANUS, 8 MIME, 9 ARM Guide, 10 and Bi-Manu-Track 11 ). The MIT-MANUS and the MIME show that recovery can be improved through additional therapy aided by robot technology. The ARM Guide and the Bi-Manu-Track demonstrate that use of simple devices makes possible intensive training for post-stroke patients with positive results. As compared to the traditional rehabilitation, robot-aided rehabilitation therapy can provide repetitive movement exercise and standardized delivery of therapy with the potential of enhancing quantification of the therapeutic process.12,13
One of the major difficulties in realizing rehabilitation by robots is the controller design. In the past few years, control system design of robot-assisted rehabilitation system has been an active research area. Different methods were utilized to control the rehabilitation robot to manipulate the impaired limb. They can be separated into three classes: force control, position control, and position and force control. At the initial stage of stroke therapy, the goal is to control the robot smoothly and stably to stretch the patient to move along a predefined trajectory with the position controller so that the rehabilitation therapy can reduce the muscle tone and spasticity of the impaired arm and increase its movable region. Several position controllers have been adopted. In O’Malley et al., 14 a traditional fixed-gain proportional–derivative (PD) trajectory controller was adopted to control the RiceWrist to move along the desired trajectory in the GoTo mode and Passive mode. This study found that the performance was dependent on the selection of PD gains. Wege et al. 15 designed a control system for hand exoskeleton which allows following recorded trajectories with sufficient accuracy, and a proportional–integral–derivative (PID) controller was implemented for the position control. Kung et al. 16 presented a position fuzzy logic controller, and the robot was controlled to stretch the forearm to perform pronation and supination.
Although the existing robot-aided rehabilitation systems provide convenient and effective tools for the post-stroke patients, there is no direct communication between the patient’s motor volitional thinking and the rehabilitation system, and the patient’s motor initiatives and attention processes may not be fully explored. In most cases, the patient can only passively follow the predefined program. 17
Brain–computer interface (BCI) technology is capable of bypassing the normal motor output neural pathways and can directly translate the electrical activity of the brain into commands to control the external devices. In recent years, BCI research is exploring many applications in different fields: environmental control, communication, and playing games. 18 Instead, the feasibility of using BCI systems to directly facilitate rehabilitation therapy of body parts impaired by neurological conditions has been demonstrated. 19 More importantly, noninvasive BCI has been shown to have a beneficial effect on the restoration of basic motor functions in stroke patients. 20 Broetz et al. 21 adopted the BCI to help a hemiplegic patient perform recovery training. Electroencephalogram (EEG) and magnetic brain activity (magnetoencephalogram (MEG)) were used to control a robot to manipulate the patient’s impaired upper limb. In this BCI-based system, the patient’s arm and hand were driven by his voluntary mu rhythm activity. Furthermore, goal-directed therapy was adopted in performing rehabilitation exercises. This research demonstrated that by combining BCI with goal-directed mechanism, motor abilities of patients after stroke can be partially recovered with physical therapy despite apparent initial paralysis. Prasad et al. developed a BCI system in which a game-based neurofeedback was provided to stroke subjects. The motor imagery task classification accuracy was adopted to evaluate the BCI performance. To some extent, this study shows that the physical therapy in conjunction with motor imagery EEG is a feasible way to perform rehabilitation training. 22
In this research, a rehabilitation system combining robot-assisted rehabilitation with motor imagery–based BCI is presented. Feature extraction and classification algorithm for the motor imagery EEG is implemented under our BCI research platform, which allows several BCI applications to be included into one single system. The main hardware platform for functional recovery therapy is the Barrett Whole-Arm Manipulator (WAM) Arm. Mental imagination of upper limb movements is translated to trigger the Barrett WAM Arm to stretch the affected upper limb to perform rehabilitation exercises. Meyer et al. 23 focus on understanding the neural correlates of motor learning which is helpful for evaluating recovery training and adjusting robot-aided rehabilitation strategies. Gomez-Rodriguez et al. mainly study how artificially closing the sensorimotor feedback loop influences BCI decoding of arm movement intention in six healthy subjects and two stroke patients. The main purpose of this work is to prove that haptic feedback can facilitate online decoding of arm movement intention in both healthy subjects and patients after stroke. 24 We mainly focus on detecting the patient’s movement intention and design an intelligent control system for the Barrett WAM to perform rehabilitation training effectively, instead of decoding multiple degree-of-freedom (DoF) from motor imagery EEG recordings. Thus, we can achieve high recognition rate of motor imagery EEG and explore the patient’s motor initiative as much as possible. A fuzzy PD position controller is proposed to control the WAM Arm to perform passive rehabilitation training, and it can reduce the vibration and chattering phenomena caused by the change in the patient’s physical condition.
Methods
Overview of the Barrett WAM Arm
The standard WAM Arm is a 4-DoF highly dexterous backdrivable manipulator. It utilizes a cable drive system, which generates less resistance than a gear mesh. This gives the WAM Arm human-like dexterity and inherent backdrivability. The cable drive system is controlled by high-performance miniature motor controllers with controller area network (CAN) bus interface. In addition, the WAM Arm is able to apply the appropriate torque to each joint to negate its own weight. A user can move the robot arm as if it is weightless, which allows for easy and natural control. With its advanced cabled drive system and high backdrivability, the WAM Arm is the ideal platform for realizing haptic, tele-operation and robot-assisted rehabilitation therapy with external force sensors.
Experimental apparatus
The standard 4-DoF Barrett WAM Arm, shown in Figure 1, is utilized as the main hardware platform for the functional recovery therapy in this research. The BCI-based upper limb rehabilitation setup consists of the EEG amplifier, a Barrett WAM Arm, a hand attachment device, a master PC (EEG recording and processing), and a slave PC (running the control loop of the Barrett WAM Arm). EEG recordings are performed with two differential channels of the EEG amplifier. Motor imagery EEG signals are measured over channels C3 and C4 according to the international 10–20 standard electrode placement. 25 The mu rhythm (8–13 Hz) and beta rhythm (13–30 Hz) originating in the sensorimotor cortex are considered as the main features for BCI systems. EEG signals are sampled at 128 Hz and band-pass filtered (0.5–30 Hz). 26

BCI-based robot-aided upper limb rehabilitation training system.
The master PC which is running with Windows 7 operating system is responsible for processing the EEG signals and sending the high-level command to the slave PC. Software of the master PC is developed under our BCI research platform which consists of recording module (record the data of multiple experiments according to the experimental timing), training module (calculate the parameters of the classifier according to the training data), and testing module (record experimental data and classify the feature vector).
A slave PC which is running with Ubuntu Linux operating system is in charge of receiving the high-level command from the master PC and supplying the WAM Arm with low-level command. The control loop running on the slave PC monitors the motor angles and torques continuously for the purpose of providing a smooth and safe motion of WAM Arm. Following the command from master PC, the affected upper limb of the subject will be stretched by the WAM rehabilitation robot and perform various rehabilitation training. Real-time communication between the slave PC and the motor pucks is realized by high-speed CAN bus with baud rate of 1 Mbps.
Interaction between the master and slave PC is implemented by client–server system with Transmission Control Protocol/Internet Protocol (TCP-IP). The master PC which is responsible for online pattern recognition of motor imagery acts as the server. The slave PC which runs the control loop of the WAM Arm serves as the client. After every BCI stimulus, the BCI system processes the motor imagery EEG signals and converts them into a command. Next, the master PC transfers the high-level command to the slave PC.
Controller design
Overview of the control architecture
Figure 2 shows the control scheme of the robotic rehabilitation system. It is designed as a two-level scheme, namely, the high level and low level. The feature extraction and classification algorithm 27 of motor imagery EEG is implemented by the high-level controller running on the master PC. Position control of WAM Arm is realized by the low-level controller running on the slave PC. After every BCI stimulus, the high-level controller processes the movement imagination EEG signals and converts them into a command. Next, the trigger command is transferred to the low-level controller via TCP/IP. Finally, the WAM rehabilitation robot will manipulate the participant to perform passive training according to the predefined trajectory.
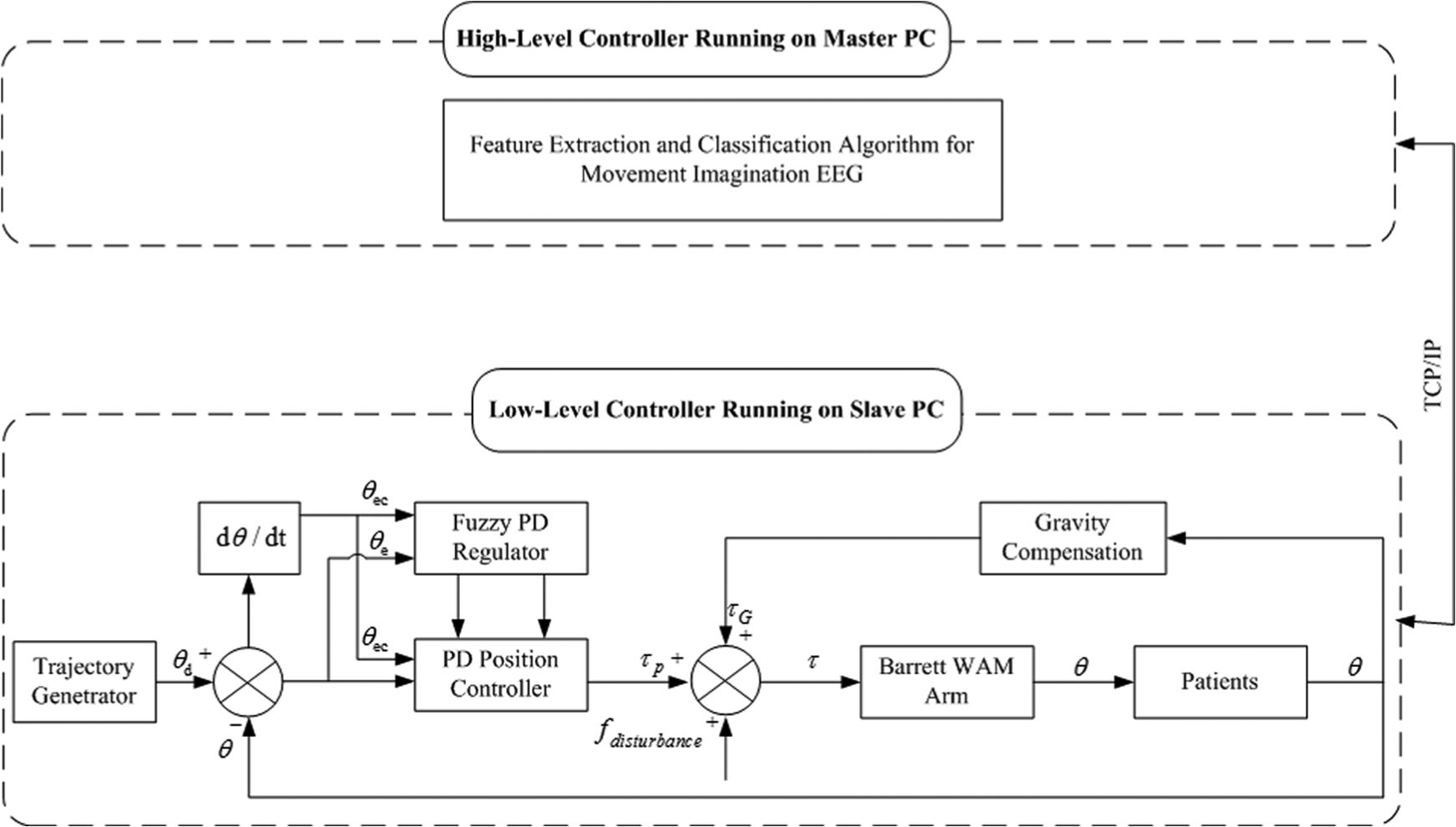
Control scheme of robotic neurorehabilitation system.
Feature extraction and classification
The flow chart of processing single-trial motor imagery EEG is shown in Figure 3. 27 First, the time window was used to filter the data in temporal domain in order to get the segment that contained the most obvious difference between the two motor imagery tasks. Then, EEG signals were decomposed into the frequency sub-bands using discrete wavelet transform (DWT), and a set of statistical features was extracted from the sub-bands to represent the distribution of wavelet coefficients according to the characteristics of motor imagery EEG signals. Also, the sixth-order autoregressive (AR) model coefficients of segmentation EEG signals were estimated using Burg’s algorithm. Next, the combination features of wavelet coefficients and the AR coefficients were used as an input vector. Finally, linear discriminant analysis (LDA) based on Mahalanobis distance was utilized to classify computed features into different categories that represent the left or right upper limb movement imagery.

Flow chart of the EEG data processing.
Channels C3 and C4 were used for feature extraction, and only the data between t = 4 and 7 s were used in order to get the segment that contained the most obvious difference between the two motor imagery tasks. The following hybrid features were used:
Six statistical wavelet coefficients;
Six coefficients of the AR model, and Burg’s method was used.
Hence, we got six statistical wavelet coefficients and six AR coefficients for each channel, giving a total of 24 features for a motor imagery task. LDA classifier was utilized to classify computed features into different categories that represent the left or right upper limb movement imagery.
Position controller
In this article, a fuzzy-based PD position control method was proposed for the passive rehabilitation training to control the WAM robot stably and smoothly to manipulate the affected upper limb to move along the predefined trajectory. Owing to the ability of adjusting the control gains according to the changes of patient’s physical condition, the fuzzy PD position controller can achieve better performance than the conventional fixed-gain PD control strategy. The position controller acts as the low-level controller implemented using C language in the slave PC with Linux operation system.
The bottom part of Figure 2 is the block diagram of the fuzzy PD position controller in joint space. The proposed regulator had separate fuzzy logic for

where
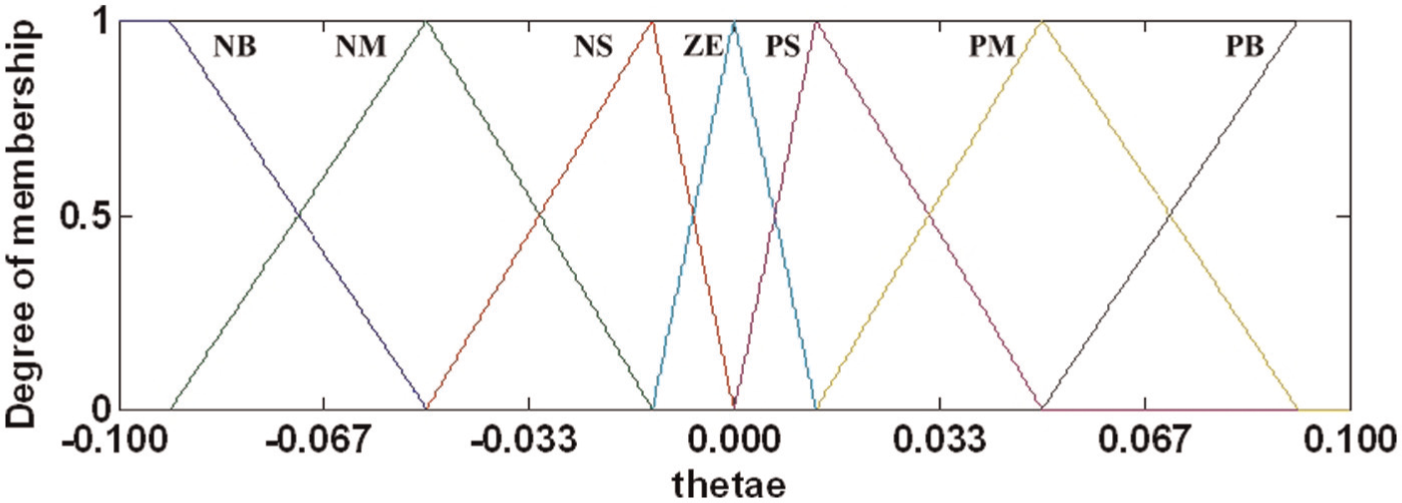
Membership functions of the input variable
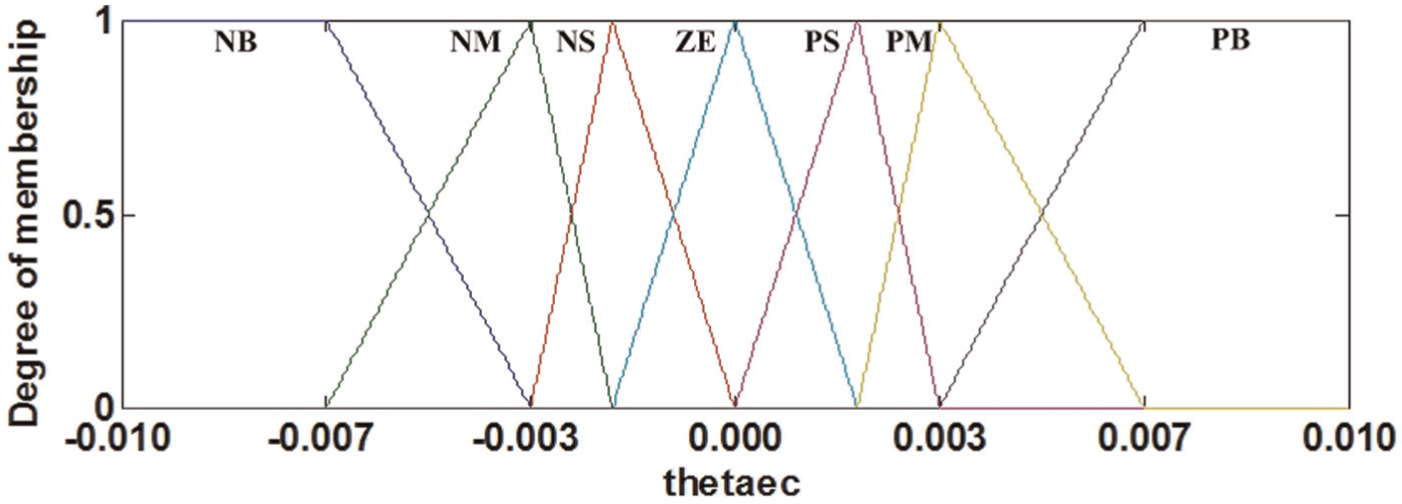
Membership functions of the input variable
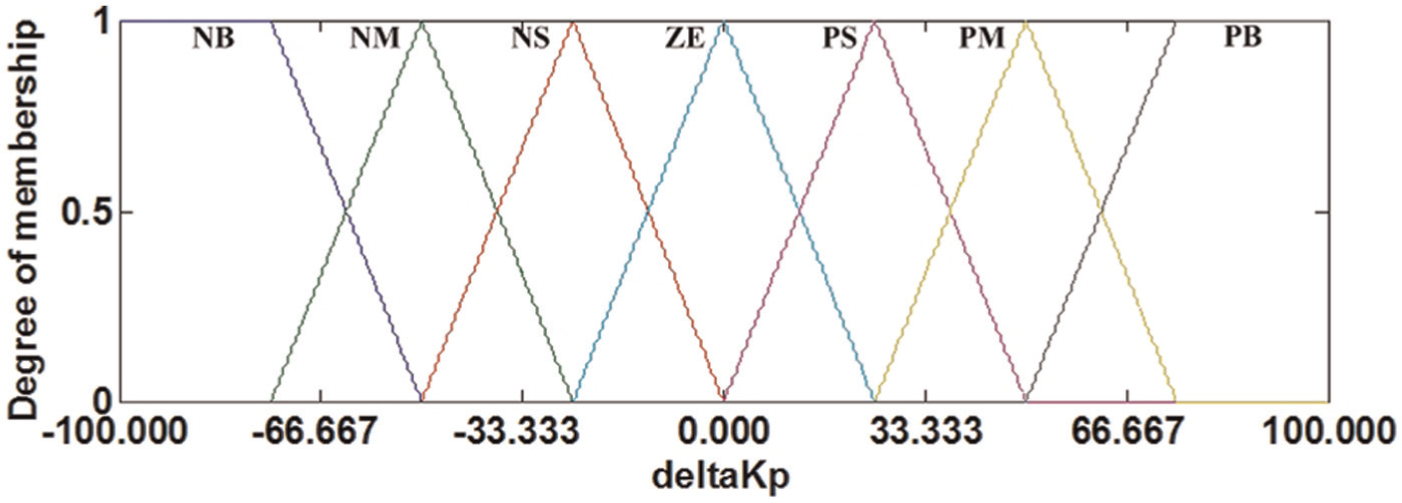
Membership functions of the input variable

Membership functions of the input variable
Inference rule table of
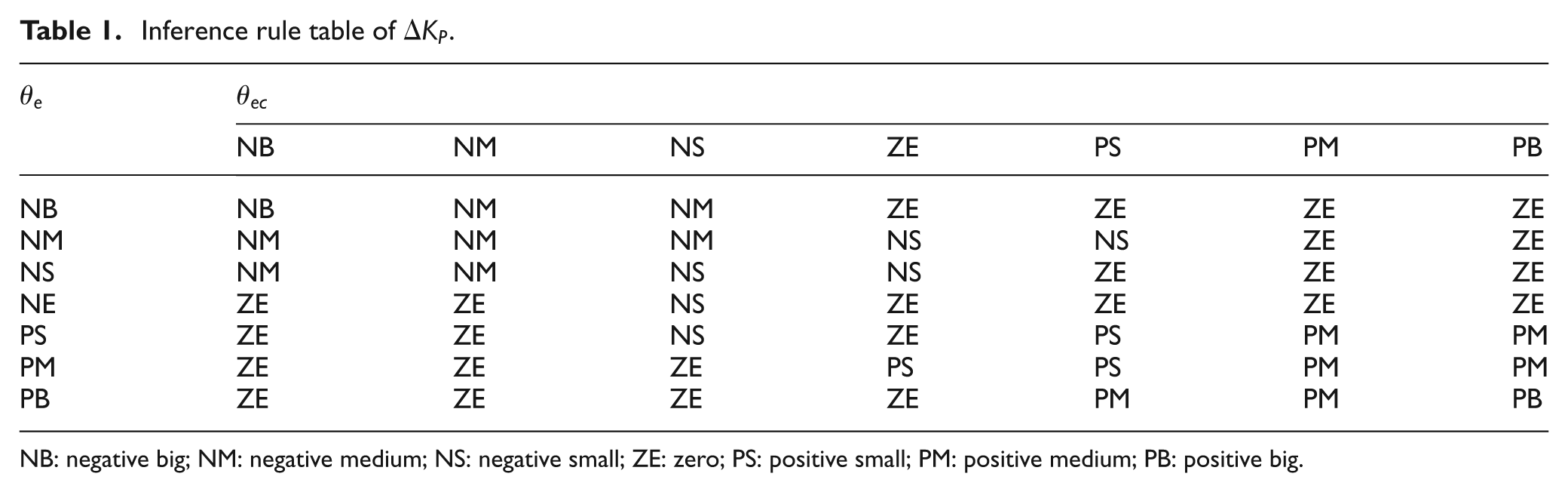
NB: negative big; NM: negative medium; NS: negative small; ZE: zero; PS: positive small; PM: positive medium; PB: positive big.

NB: negative big; NM: negative medium; NS: negative small; ZE: zero; PS: positive small; PM: positive medium; PB: positive big.
Subjects
The experiments were carried out with eight healthy participants (four females, four males) with ages ranging from 23 to 31 years. They had no previous experience with BCI system and rehabilitation training. All the participants were volunteers from Southeast University in Nanjing, China. Informed consent was obtained from the participants, and this research had been approved by local Ethics Committee.
Experimental procedures
Participants sat in a comfortable chair, watching two 19″ monitor screen at a distance of 1.2 m with black background. Before the beginning of each session, a researcher explained the task by using simple instructions and showing video. A trial was divided into four consecutive phases. Each trial started with the word “Attention” displayed on the master PC for 3 s. Then, participants were cued with three-dimensional animation of left or right upper limb movement between 3 and 7 s. Meanwhile, participants were asked to perform motor imagery of left or right upper limb movement. Next, the master PC processed the EEG signals and sent the high-level command to the slave PC. Finally, the slave PC provided the WAM with control command and the upper limb of the participant was stretched by WAM rehabilitation robot to perform rehabilitation training. Figure 8 illustrates the timing scheme of the experiment.

Timing scheme of the experiment.
The experiment was made up of two runs for each of the three different cases: robot-alone without manipulating a subject, with a normal subject in passive movement, and with unpredictable disturbance when performing exercises. Each run consisted of 10 trials for each of the two conditions, shown in Table 3. Participants were allowed to take rest at the end of each run or every 10 trials.
Two different conditions for the experiment.

PD: proportional–derivative.

Vertical flexion/extension movement trajectory for upper limb.
For the left upper limb rehabilitation exercise, the WAM Arm will manipulate the impaired left upper limb in a similar way as during a physical therapy exercise in case the left upper limb movement imagination is detected correctly. If the right upper limb movement imagination is recognized, the virtual right upper limb is provided by the master PC for the purpose of strengthening the process of motor imagery. Conversely, for the right upper limb recovery training, the master PC will give the virtual left upper limb movement so as to enhance the motor imagery process if the left upper limb movement imagination is recognized. WAM rehabilitation robot will stretch the affected right upper limb to perform recovery training on condition that right upper limb movement imagination is decoded correctly.
Experiment results
The experiments were conducted on the motor imagery–based robotic rehabilitation system with vertical and flexion/extension exercises. We studied three different cases: robot-alone without stretching a subject, a normal subject in passive movement, and with unpredictable disturbance where a normal passive subject is still performing exercises. Furthermore, a sinusoidal movement trajectory was designed to verify the effectiveness of the proposed position control strategy based on the fuzzy method.
The performance of the BCI was evaluated by the recognition rates of the movement imagination task. Figure 10 demonstrates the average recognition rates of the two runs for all participants in three different cases. It can be seen from the figure that participants achieved an average recognition rate between 83.00% and 93.00%. Using the combined feature vectors of DWT and AR is capable of extracting more useful information from the simultaneously acquired motor imagery EEG. Additionally, a recognition rate between 80.00% and 90.00% was obtained during the first session.

Average recognition rate of each subject.
In the vertical flexion/extension experiment, the performance of fuzzy and conventional PD position controllers in regard to the fourth joint of the WAM Arm was studied. The range of movement for upper limb, expressed in the world coordinates of WAM Arm, was set as −5.3 rad in flexion and −3.9 rad in extension. The gains
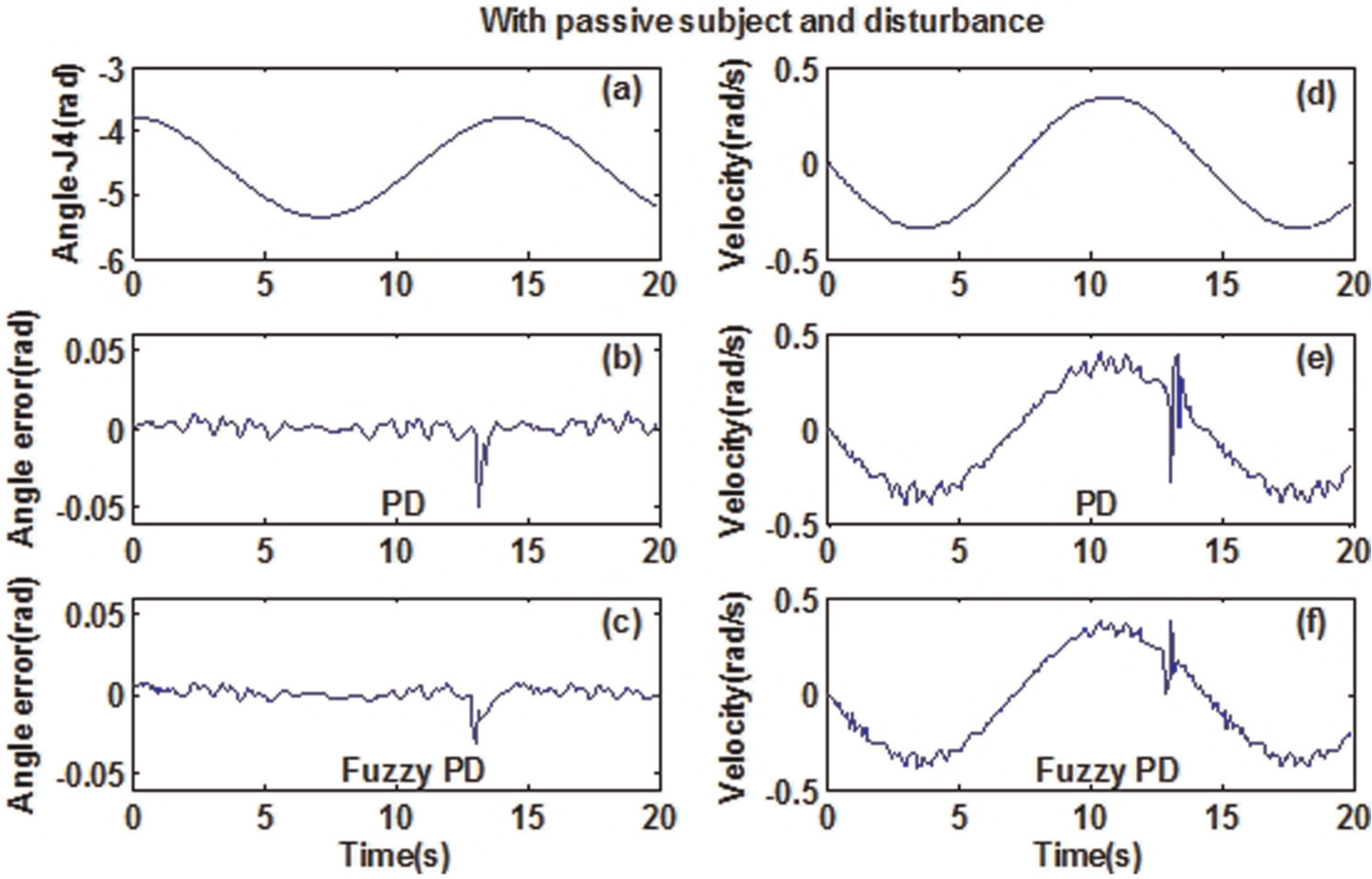
Figures 11–13 show the experimental results of the fuzzy and traditional PD position controllers in three different cases. The subject performs passive recovery training using sinusoidal trajectory. The results reveal that both position control strategies succeed in implementing the desire trajectory. However, the tracking of the predefined trajectory is better achieved with the fuzzy-based PD controller, which can be observed from the error of angle control and joint velocity tracking.

Joint position control in vertical flexion/extension training without carrying a subject. Sinusoidal trajectory control of the fourth joint: (a) target trajectory, (b) angle error under traditional PD control method, (c) angle error of fuzzy PD control strategy, (d) target velocity, (e) velocity tracking using traditional PD controller, and (f) velocity tracking by fuzzy PD controller.

Joint position control in vertical flexion/extension training with a passive normal subject. Sinusoidal trajectory control of the fourth joint: (a) target trajectory, (b) angle error under traditional PD control method, (c) angle error of fuzzy PD control strategy, (d) target velocity, (e) velocity tracking using traditional PD controller, and (f) velocity tracking by fuzzy PD controller.
Joint position control in vertical flexion/extension training with disturbance in the Z direction. Sinusoidal trajectory control of the fourth joint: (a) target trajectory, (b) angle error under traditional PD control method, (c) angle error of fuzzy PD control strategy, (d) target velocity, (e) velocity tracking using traditional PD controller, and (f) velocity tracking by fuzzy PD controller.
The performances of the position controllers were evaluated by two indices: the means and standard deviations (MSDs) of the trajectory tracking errors and the maximum of the absolute error (MAE). These results are presented in Table 4. It is clear that, in three different cases, the fuzzy-based position controller gets the small MSD and MAE values, and a better position control accuracy is achieved.
Comparison of fourth joint position control performance.

MSD: mean and standard deviation; MAE: maximum of the absolute error; PD: proportional–derivative.
Figures 14 and 15 illustrate the joint torque of the two position controllers in the vertical flexion/extension exercises. In the case of a normal subject in passive movements, it can be observed that the position control method based on a fuzzy controller achieves less vibration than the conventional PD method. In addition, a large torque overshoot happens in the traditional PD position method when we apply a disturbance. However, the fuzzy-based controller obtains very small vibration.

Torque of the fourth joint in vertical flexion/extension with passive subject: (a) traditional PD position controller and (b) fuzzy-based position controller.

Torque of the fourth joint in vertical flexion/extension with disturbance: (a) traditional PD position controller and (b) fuzzy-based position controller.
Conclusion and future work
In this article, a new approach to offer recovery training for stroke patients was proposed. We investigated the feasibility of integrating robotic rehabilitation with motor imagery–based BCI. The pattern recognition algorithm for upper limb movement imagination EEG was realized under our BCI research platform. The Barrett WAM Arm was utilized as the main hardware platform for the functional recovery therapy. Mental imagination of upper limb movement was detected to trigger the Barrett WAM Arm to manipulate the impaired upper limb to perform rehabilitation training. The fuzzy-based PD position control strategy was used to control the WAM Arm to move along predefined trajectories for passive recovery exercise.
The preliminary results on unimpaired participants demonstrate the following. (1) By translating subject’s motor intention into a high-level command to trigger the WAM rehabilitation robot, the patient’s motor initiatives or attention processes can be fully explored and the WAM rehabilitation robot can stretch the upper limb of stroke patients to perform recovery exercise effectively. (2) By using fuzzy position control strategy, the WAM Arm can manipulate the subject’s upper extremity to move along predefined trajectories stably and smoothly. Also, the vibration and chattering phenomena caused by the change of the patient’s physical condition can be reduced. (3) The combination of robot-aided physical therapy and motor imagery–based BCI can be expected to constitute a promising approach to stroke rehabilitation, particularly for severely impaired stroke patients.
In order to further evaluate the proposed motor imagery EEG-based robotic rehabilitation training system, clinical study with stroke patients is currently undertaken.
Footnotes
Academic Editor: Zhuming Bi
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Natural Science Foundation of China (No. 61325018, No. 61104206, No. 61305095, and No. 61302131), Natural Science Foundation of Jiangsu Province (No. BK20141284), National High Technology Research and Development Program of China (No. 2013AA013703), Key Technology R&D Program of the Ministry of Science and Technology of Jiangsu Province (No. BE2012740), RD Project of China Southern Power Grid (K-GX2014-208, K-GX2014-062-49), the Open Fund of Jiangsu Province Key Laboratory for Remote Measuring and Control (No. YCCK201005, No. YCCK201205), and RD Projects of Guangdong Province and Guangzhou City.