
Abstract
In long-term dementia care, simulative technology such as robotic pets and virtual reality is increasingly used to support psychosocial well-being. While their ethical use has been debated in the literature, the voices of stakeholders, including people living with dementia, family members and care staff have not been meaningfully represented. This protocol paper describes a two-phase qualitative study that aims to identify stakeholders’ perceptions of ethical issues relating to simulative technology use and ways to navigate these issues in long-term care contexts. In Phase 1, a constructivist grounded theory approach will be used to explore stakeholders’ perceptions of ethical issues; in-depth interviews or focus group discussions will be conducted with people living with dementia, their family members, long-term care staff, and managers. Discussions will be audio-recorded, transcribed verbatim, and analyzed. In Phase 2, a virtual Nominal Group Technique will be used to explore means in which ethical dilemmas can be navigated. Participants will include stakeholders as described in Phase 1, along with ethics experts and decision-makers. Participants will review the ethical issues and ways to navigate dilemmas as identified in Phase 1, suggest additional issues and strategies to navigate dilemmas, and a mixed-methods analysis will be applied to prioritize strategies, and a qualitative content analysis will be used to analyze free-text comments to identify rationales behind prioritization. The findings will inform the development of a resource guide that integrates the lived experiences and expert knowledge to support ethically informed technology use in long-term dementia care.
Keywords
Background
Worldwide, over 57 million people live with dementia; this number is expected to nearly triple to 152 million by 2050 (Nichols et al., 2022). People living with dementia are transitioned to long-term care (LTC) when care needs, family caregiver burden, safety concerns and care dependency increases (Toot et al., 2017). Long-term care, which has also been termed as nursing homes or residential aged care in different countries (Sanford et al., 2015), provide ongoing healthcare and support for older adults who are dependent on assistance with activities of daily living. Within LTC contexts, staff often experience challenges providing dementia care due to limited training, staff shortages and high staff turnover rates (Gilster et al., 2018; Rhodes & Martin-Matthews, 2023; Shen et al., 2023). In particular, managing behavioural and psychological symptoms of dementia, including aggression, agitation, anxiety, disinhibition (Makimoto et al., 2019) has been identified as a key source of stress. Correspondingly, a strain in the LTC workforce has been reported to lead to reduced dementia care quality (Costello et al., 2019). Rapid digital advancements have seen a range of innovative technologies being developed to support the LTC workforce and enhance dementia care quality (Astell et al., 2019). Simulative technologies are a stream of innovative technologies that are designed to provide simulated experiences and environments to improve psychosocial wellbeing, such as reducing behavioural and psychological symptoms. Prominent examples of simulative technologies include pet robots and virtual reality (VR). Pet robots are a type of robot that mimic the physical characteristics and behavioural responses of companion animals such as domestic pets (e.g., cats and dogs), simulating pet therapy (Bartneck & Forlizzi, 2004; Eachus, 2001). Immersive virtual reality provides a range of simulated three-dimensional (3D) environments, such as familiar scenery or novel environments (e.g., underwater scuba diving), for the purposes of reminiscence, relaxation or social engagement (Flynn, Brennan, et al., 2024; Webber et al., 2021). Emerging evidence indicates that simulative technologies have the potential to produce promising positive effects, such as reducing agitation, improving social engagement and mood (Flynn, Koh, et al., 2025; Koh et al., 2021; Pu et al., 2019).
Despite their potential to enhance psychosocial wellbeing among people with dementia, the use and implementation of simulative technologies remains a contentious topic as the ethics underpinning their use are heavily debated in the literature (Vandemeulebroucke et al., 2018). For example, while simulative technologies could be empowering, they may potentially infringe upon users’ freedom; in addition, users may not be able to distinguish them from reality or be ‘deceived’ into believing that simulated experiences like virtual reality are real. Other ethical issues relate to concerns that such technologies may replace human caregiving or substitute human interactions, and that they could lead to psychological harm. These debates constitute important ethical considerations; however, they may not sufficiently reflect lived experience perspectives, which may differ from those of ethicists. In a study which explored the ethical intuitions of LTC staff when using pet robots in dementia care, Koh et al. (2023) found that staff prioritized the positive psychosocial impact of pet robots on residents with dementia and placed substantially less weight on the ‘deceptive’ nature of pet robots. This might be attributed to the notion that staff have a more nuanced understanding of the dynamic nature of dementia care in LTC contexts and its demands. Furthermore, staff across different disciplines and facilities had different notions of what constituted ethical use of pet robots; for example, some staff felt that pet robots must be introduced as robots, however others felt that they should introduce them as real pets if residents perceive them as real. This suggests that inconsistent and inequitable use of simulative technologies may exist within LTC facilities, depending on individual staff’s perceptions and values. To support LTC staff to use simulative technologies in ethically sound ways, stakeholder-informed and contextually relevant guidance is necessary. Nevertheless, current ethical debates lack collective input from stakeholders such as people with dementia and their family members. The exclusion of people with dementia from such research might be due to assumptions about their ability to engage in abstract thinking for ethical reasoning. In addition, traditional verbal interviewing methods may not be sufficiently inclusive to engage people with dementia in ethical discussions. Innovative, accessible approaches such as visual approaches are needed to engage people with dementia and other stakeholders in ethical discussions (Beuscher & Grando, 2009; Conway et al., 2023; Phillipson & Hammond, 2018). Collective input from people with dementia, family members and LTC staff is necessary to better understand their perceptions of ethical issues that may arise from simulative technology use, and how such situations may be navigated, considering contextual challenges within LTC contexts.
Objectives
The primary objective of this research is to develop the evidence that is needed to guide the ethical use of simulative technologies for dementia care, specifically in LTC settings for care staff, managers and decision-makers. Using inclusive and participatory approaches, this research will involve various key stakeholders in generating knowledge of the ethics of simulative technology use in dementia care, based on lived experiences and an understanding of the LTC context. This research will be conducted in two key phases to address the following research questions: Q1: What are key stakeholders’ (i.e.,people living with dementia, family caregivers, long-term care staff and managers) perceptions of ethical issues relating to the use of simulative technologies in dementia care? Q2: What strategies can be used to manage ethical issues relating to the use of simulative technologies in dementia care?
Public and Patient Involvement and Engagement
At the outset of this research, an advisory committee comprising two older adults with lived experiences of dementia and two family members with experience in informally supporting a person with dementia was established. An embedded consultation approach to public and patient involvement and engagement was adopted (Hughes & Duffy, 2018), with meetings scheduled every three to six months to receive feedback throughout the lifecycle of this research project. During the first meeting, held prior to designing and drafting this research protocol, the committee reviewed the research questions to ensure the overall approach to the study was meaningful. The committee also provided feedback on designing the ethical vignettes (described in detail in ‘Phase 1 - data collection’ section below), advising on the visual presentation format, clarity of the ethical vignettes script and accessibility for people living with dementia. Future meetings will review the findings and contribute to interpretation, contextualizing results within lived experience. The committee will also advise on dissemination strategies and formats to maximize accessibility for stakeholders.
Study Design and Methods
An overarching qualitative methodology will be employed across two phases; phase 1 aims to explore key stakeholders’ perceptions of ethical issues in simulative technology use in dementia care, and phase 2 aims to explore and identify ways to navigate ethical situations relating to the use of simulative technologies.
Phase 1: Exploring Ethical Perceptions
Stakeholder Group-Specific Eligibility Criteria
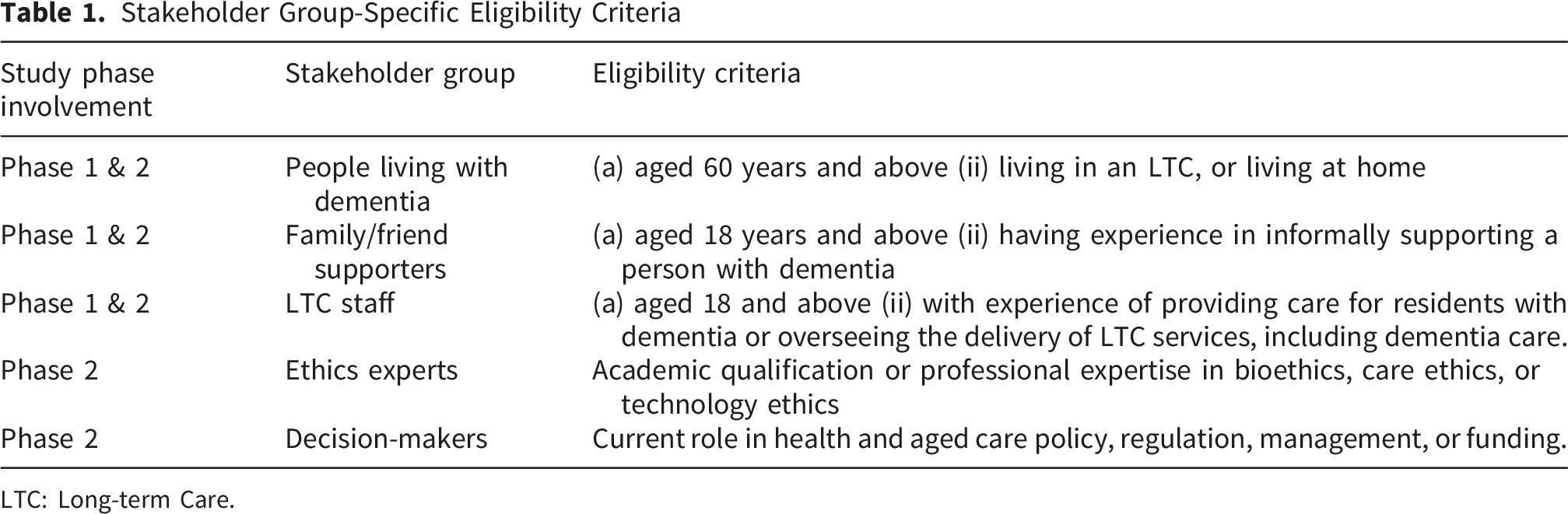
LTC: Long-term Care.
Phase 1 - Recruitment and Sampling
Participants will be the stakeholders involved in the use of simulative technologies within LTC. This will include three stakeholder groups (i) People living with dementia (ii) family members, (iii) LTC care staff (personal carers, health professionals) who provide care to residents with dementia, and LTC managers who oversee the delivery of care services, including dementia care. All participants must be able to provide written consent to participate in the study, understand and speak English, and either have used, are using, or are open to being introduced to simulative technologies. See Table 1 for the stakeholder group-specific eligibility criteria. Participants will be recruited from LTC and home care providers in Australia, dementia advocacy networks and support groups, snowball sampling, community-based venues, social media, and the StepUp for Dementia Research platform (Jeon et al., 2021). Sampling will continue until conceptual saturation is achieved, and categories and relationships between categories are well developed.
Phase 1 - Data Collection
Data will be collected through in-depth interviews and focus group discussions. Discussions will be guided by videos of ethical vignettes and a topic guide. Each ethical vignette comprises a short animation (approximately 10 seconds per vignette) depicting scenarios where the use of simulative technology (robotic pets or virtual reality) has evoked (or may evoke) ethical dilemmas. The use of videos as a media platform enhances the cognitive accessibility of vignettes for all participants, particularly for people living with dementia.
Two to four ethical vignettes will be used to elicit discussions for each interview or focus group. A systematic process was applied to develop the vignettes. First, the chief investigator (WQK) undertook a literature review to identify ethical issues and concerns associated with the use of simulative technology in dementia care, based on seven ethical domains relating to the use of care robots in aged care as outlined by Vandemeulebroucke et al. (2018). They include: (1) respect for autonomy and privacy, (2) dignity, objectification and deception, (3) replacement for human care, (4) social isolation and loneliness, (5) safety, physical and psychological harm, (6) social justice, and (7) conceptions of care (Appendix 1-1.1). Consistent with constructivist grounded theory methodology recommendations, this review was conducted with a receptive, provisional, critical, and analytical approach to ensure emergent findings were not predetermined by prior research (Charmaz & Thornberg, 2021). The findings were discussed within the research team, comprising researchers with expertise in robotic pets for dementia care (WQK), innovative technology (JL), virtual reality (AF), care ethics, bioethics, and the ethics of technology (TV). They were also discussed with our advisory committee to leverage lived experiences. The ethical issues and concerns to be explored through the use of simulative technology are listed in Appendix 1-1.2. Second, the identified ethical issues and concerns were then transformed into animated videos comprising of ethical vignettes. Each vignette incorporates characters representing stakeholder groups (such as residents, LTC staff, or family members), narrative scenes depicting ethical scenarios and an ethical dilemma question to prompt reflection. For instance, one vignette introduces Debbie, a recreational officer who believes that Mark, a resident living with moderate dementia, might benefit from using virtual reality. The narrative unfolds to show Debbie’s reasoning in the context of Mark’s care (social engagement), concluding with the ethical question: “How should Debbie know if Mark might like virtual reality? [Ethical concept: Respect for autonomy]. See Appendix 1-1.3 for the vignette transcript.
Topic Guide for In-Depth Interviews and Focus Group Discussions

Phase 1 - Data Analysis
Data analysis will follow a constructivist approach, occurring iteratively and concurrently with data collection to facilitate constant comparison. Coding will follow two key phases; initial (open) coding followed by focused coding to synthesize and integrate the most significant or frequent codes. A research team member will familiarize themselves with and code the first five transcripts line by line while remaining close to the data. During this process, the researcher will take notes and memos to reflect on this initial analysis process. Next, focused coding will be applied to the sixth transcript, where codes of significance will be synthesized, analyzed, and conceptualized into tentative categories. Initial codes will be grouped, integrated or disintegrated; emerging codes will be applied to additional transcripts. Given that this is an iterative process, additional theoretical codes are expected to be generated and will be integrated into the evolving coding framework and concepts. Constant comparative analysis will be repeated until no new insights emerge from the data, and so conceptual saturation is reached. During the focused coding process, meetings with the wider research team and the Advisory committee will be held to ensure a holistic interpretation of the data. The findings will inform Phase 2, which includes Nominal Group Technique sessions.
Phase 2: Prioritize Strategies for Simulative Technology Use in Dementia Care
A virtual Nominal Group Technique (vNGT) will be employed to prioritize ways of navigating ethical issues related to simulative technology use in dementia care, as identified in Phase 1. This approach will integrate the lived experiences of stakeholders, their understanding of the operational complexity, and ethical considerations in LTC. vNGT is particularly suited to the study’s objective as we are looking to explore opinions, determine ethical priorities, and to have a balanced participation from different stakeholders (people with dementia and LTC staff, family members, ethics experts, and decision-makers), so that all stakeholders will have an equal voice based on their lived experience expertise, alongside professional ethics, policy and decision- making experts. The latter is a critical consideration given the power differentials inherent in mixed-stakeholder groups (McMillan et al., 2016). Sessions will be conducted online following Smith et al. (2024) recommendations for vNGT delivery, which has demonstrated methodological rigour while addressing logistical challenges associated with geographically dispersed stakeholders across Australia (Lee et al., 2024). Ethical approval will be obtained prior commencement of this study.
Phase 2 - Recruitment and Sampling
Phase 2 will recruit people living with dementia, their family members, and LTC staff using the same eligibility criteria described in Phase 1, with the addition of ethics experts and decision-makers (Refer to Table 1). Two to three participants from each stakeholder group will be recruited per session. This sample size aligns with McMillan et al. (2016) guidance of heterogeneous groups being acceptable when diverse perspectives are essential.
Phase 2 - Data Collection
Data will be collected through vNGT sessions. Materials for the vNGT session will be developed based on the findings from Phase 1 qualitative interviews. Specifically, suggestions identified by participants during Phase 1 will be presented for each case scenario. This approach ensures that Phase 2 consensus-building is firmly grounded in the voices of participants, while inviting vNGT participants to expand beyond Phase 1’s findings by generating additional ways of navigating ethical dilemmas that were not previously captured. All materials will be piloted with the advisory committee prior to the vNGT session to ensure clarity and appropriateness for the diverse stakeholder group. Each session will comprise three key stages as described below. Stage 1 - Individual Responses: Participants will independently generate suggestions in response to ethical dilemma scenarios presented, then share the suggestions in a round-robin format, one suggestion at a time. This round will be repeated until no new suggestion is elicited. All suggestions will be recorded on a shared document visible to all participants. Stage 2 - Clarification and Discussion: During this stage, participants will be invited to seek clarification of suggestions recorded in Stage 1. This step ensures that the appropriate meanings of every idea are captured. Similar ideas will be merged with a group agreement. Stage 3 - Voting and Ranking: The primary objective of this stage is to prioritize the suggestions obtained in the previous stages. Participants will independently rank their top priority strategies using an online polling tool such as Qualtrics or Microsoft Forms. The ranking scale will be between 1 (most preferred suggestion) and 5 (least preferred suggestion).
Phase 2 - Data Analysis
A mixed-method analysis will be employed. A quantitative analysis will be conducted to identify prioritised suggestions for each ethical dilemma. An aggregate score for each suggestion will be generated and ranked to prioritise it. To do this, each suggestion (item) will be given a score between 0 and 5 [Score 0, if the suggestion was not ranked; Score 5, 4, 3, 2, 1 for Rank 1, 2, 3, 4, 5 respectively], and a summative ranking will be calculated. In parallel, content analysis will be completed of vNGT sessions to establish the reasoning behind prioritisations made and ethical reasoning.
Phase 1 & 2: Ethics
Participant information sheets and informed consent forms will be provided to all participants, detailing the purpose of the study, data collection procedures, potential risks and benefits, confidentiality measures, and their right to withdraw without prejudice or consequences.
Researchers will seek both assent and consent from participants with dementia to ensure their voluntary participation is acknowledged and valued. Assent will be sought as an affirmative agreement to participate (Cahill & Wichman, 2000). This approach recognizes that individuals with dementia retain varying degrees of understanding, reasoning, and the ability to express choices. If participants show verbal or non-verbal dissent, such as discomfort or unwillingness to engage, their decision will be respected. Consent will be obtained directly from participants with dementia whenever possible. If a participant is unable to provide consent independently, their legally appointed decision-maker will be approached. Family members or next of kin will also be informed and provided with study materials for transparency. We also acknowledge that the capacity to consent is time-specific, and people with dementia often experience memory difficulties, which may affect their ability to retain and recall the information about the study or their consent to participate. Hence, people living with dementia will receive study information seven days before participation, and verbal consent will be obtained again before each interview or focus group to ensure ongoing willingness to participate.
Strategies for Inclusive Research Approach: Several strategies will be put in place to support participants to engage in this research considering different abilities. A phone call will be made to prospective participants with dementia upon receiving their expression of interest to explain the study, answer questions and discuss support needs such as comfort level with logging onto a Zoom (videoconferencing platform), and whether a family member will be able to assist if needed.
Data collection materials and interview questions were discussed and developed in consultation with our Advisory panel to maximize their cognitive accessibility for participants. All data will be managed in accordance with The University of Queensland Research Data Management Policy. Online data collection sessions will be conducted via Zoom (Institutional Zoom account); prior to each interview or focus group, participants will be offered the opportunity for an early log-on to Zoom to troubleshoot any prospective technical issues. If a participant shows signs of distress or fatigue during an interview or focus group, such as restlessness or discomfort, the session will be paused, and participants will be offered a break, or the opportunity to withdraw or reschedule, depending on their preference. If the participant continues to show signs of distress, the researcher will also ask for permission to contact the participant’s next-of-kin or preferred contact person to ensure appropriate support is provided.
Rigour
Rigour will be maintained to ensure the credibility, transferability, dependability, and confirmability of this research. A clear research methodology and participant selection criteria, including sampling considerations, interview procedures, and the development of ethical vignettes, will ensure transparency and reduce the influence of researcher bias. A detailed research record will be maintained as a transparent audit trail, documenting all decisions made throughout the study. NVivo software will be used to facilitate data analysis of verbatim transcripts, enabling consistent coding and providing an audit trail for the analysis process.
The Standards for Reporting Qualitative Research (SRQR) checklist (O’Brien et al., 2014) will guide the reporting of findings, ensuring comprehensive and transparent documentation of the research process. Additionally, the iterative nature of data collection and grounded theory analysis will further enhance the trustworthiness of the findings by incorporating constant comparison and multidisciplinary team input.
Researcher Position
The research team acknowledges their positioning as allied health researchers with varying degrees of experience in dementia care, innovative technology, qualitative research, and co-design methods. The lead investigator’s background is in occupational therapy and has predominantly worked in dementia care and with various technologies for people living with dementia, which provides contextual understanding of both clinical care and technology systems. This positioning might potentially create assumptions about technology benefits that require reflexivity. A constructivist epistemological stance is adopted by the researchers, recognizing that research findings will be generated through co-creation and collaborative interpretation between researchers and participants (Mills et al., 2006). A reflexive practice will be maintained using reflexive journals, memo writing, category identification, and regular team meetings to discuss these topics. Regular consultations with the advisory committee will be conducted to ensure that the researcher’s perspectives do not overshadow the voices and lived experiences of participants.
Discussion
Innovative technologies for dementia care are advancing globally, yet there is a lack of evidence to guide their ethical implementation in LTC settings. This two-phase study aims to develop a resource guide that integrates the lived experiences of stakeholders with ethical theory and expert knowledge. Phase 1 employs a constructivist grounded theory approach, using in-depth interviews and focus groups with people living with dementia, their carers (family members and friends), and LTC staff to explore nuanced ethical tensions. Phase 2 employs vNGT to build consensus on strategies for addressing the ethical issues identified in Phase 1, bringing together stakeholders with ethics experts and decision-makers.
The use of vignettes in Phase 1 is an innovative, inclusive way to elicit participants’ responses to complex ethical scenarios, as they provide concrete, contextualized situations that participants can engage with meaningfully (Tremblay et al., 2022). This approach helps participants visualize scenarios based on real-world experiences in an LTC context, which provides participants with dementia who do not reside in LTC an understanding of contextual influences. The decision to conduct NGT virtually addresses logistical challenges associated with geographically dispersed stakeholders while maintaining methodological rigour. Virtual delivery also reduces travel burden for participants in remote areas and those with mobility challenges.
The dissemination strategy will target multiple audiences, including LTC community providers, managers, and other staff; dementia researchers working in the field of innovative technology; technology developers; and consumers and the general public. Visual and plain English summaries will be shared with all consumers and participants. Findings will be published in open-access, peer-reviewed journals. All non-identifying materials that cannot be included in publications (e.g., due to word limits or journal restrictions on supplementary materials) will be made publicly available on the Open Science Framework, ensuring that findings and materials are openly accessible for transparency and reproducibility. Findings will be shared via social media and the Chief Investigator’s institutional media and communications team to reach the broader public.
The findings of this study will aim to balance the benefits of technology with the complexities of dementia care, providing practical recommendations and resources for LTC facilities while respecting the dignity and preferences of people living with dementia and other key stakeholders. This work has the potential to inform policy, improve care practices, and support the responsible integration of technology in dementia care.
Supplemental Material
Supplemental Material - Ethical Use of Simulative Technologies for Dementia Care in Long-Term Residential Facilities – A Qualitative Study Protocol
Supplemental Material for Ethical Use of Simulative Technologies for Dementia Care in Long-Term Residential Facilities – A Qualitative Study Protocol by Divya Anantharaman, Jacki Liddle, Aisling Flynn, Tijs Vandemeulebroucke, Chris King, Bobby Redman, Kevin Edward Roache, Gillian Woodhouse, Wei Qi Koh in International Journal of Qualitative Methods
Footnotes
Acknowledgement
We acknowledge the Dementia Advocates Program for helping us establish our advisory committee.
Ethical Considerations
Ethical approval for Phase 1 research was granted by the Human Research Ethics office of The University of Queensland (Ethic Id: 2025/HE000459).
Funding
The authors disclosed receipt of the following financial support for the research, and/or publication of this article: This project is funded by Dementia Australia Research Foundation Project Grants and the University of Queensland, School of Health and Rehabilitation Sciences New Staff Start-Up Grant.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.