
Abstract
Understanding the complexity of health services for older people living with dementia is a challenging research endeavor. We discuss a novel research approach that combines photographic methods with storyboarding techniques to understand the views of older people living with dementia who encounter the emergency department. A social ecological theoretical position was taken to study relationships between health care systems and processes and the social arrangements of those receiving care. The research approach uncovers complex contextual factors in health care systems that are amenable to change. The approach strengthens the contribution of older people living with dementia to have their voice included in research endeavors.
Understanding the complexity of being an older adult living with dementia in a busy emergency department (ED) is a challenging research endeavor. The challenge comes when we enter research settings that contain complex contextual factors like physical and social age–related features possessed by older people, circumstances imposed by the condition of dementia, converging perspectives of multiple people (the older person’s family and health care professionals), and the chaotic environment of the ED. The synergy of these converging factors confound research investigations.
This article presents a novel research approach that evolved from a previous study (Parke et al., 2013). The approach combines photographic methods with storyboarding techniques to address the methodological problem of systematically incorporating the views of older people living with dementia in research. Our approach does not simply describe contextual factors but illuminates influences, relationships, and resulting synergies to mitigate harmful outcomes.
Background Justification for the Research Approach
Practice and policy changes in health care systems are more meaningful when those directly affected by such change are included. Unfortunately, older people tend to be excluded from research (Lee, Alexander, Hammill, Pasquali, & Peterson, 2001; Tetley, 2013), and those who also live with dementia are even more likely to be excluded (Tanner, 2012). The views of those living with dementia are discounted or seen through a proxy decision maker (Fetherstonhaugh, Tarzia & Nay, 2013; Tanner, 2012; Taylor, DeMers, Vig, & Borson, 2012). Recruitment problems (Harris & Dyson, 2001; Marcantonio et al., 2008) and underrepresentation of their views (Darling & Parra, 2013; Dupuis et al., 2012) create difficulty in the application of research findings into practice and policy change.
Estimates indicate 44.4 million people are living with dementia worldwide (Alzheimer’s Association, 2013; Alzheimer’s Disease International, 2013). A worldwide rise in the number of people living with dementia is expected to increase to 135.5 million by 2050 (World Health Organization, 2012). Studies from many countries reflect concern about meeting the needs of people with dementia within health care systems, including EDs (Chen et al., 2013; Clevenger, Chu, Yang, & Hepburn, 2012; Cummings et al., 2012; Hallberg et al., 2013; Howie, 2012; Hustey & Meldon, 2002; Tan, Jennings, & Reuben, 2014). Internationally, the prevalence of dementia in hospital is high and increasing, which makes uncovering all facets of complex interactions an imperative.
Older people living with dementia can contribute to research because they are uniquely qualified to do so when the research approach capitalizes on their strengths and abilities. Finding ways to include them as partners in research is needed to inform evolving health care services. Further, changes in interdisciplinary practices require a deeper understanding of what influences success of complex health care transitions for this population. Finally, the research approach we discuss meets recommendations set forth by professional organizations and health ethic review boards for persons living with dementia.
Theoretical Perspective
Our theoretical perspective for this research approach rests in social ecological theory (Bronfenbrenner, 1979; Rubinstein & De Medeiros, 2004). Social ecological theory is concerned with dynamic processes and behaviors that stem from interactions between individuals and the environments in which they live and work. There is a relationship between the personal characteristics of people and the characteristics found in the environment. The interaction between the two result in reinforcing consequences. This perspective is ideally suited to study complex relationships between health care systems and processes and the social arrangements of the people who provide or receive care. Clark (2013) suggests that complex health interventions are composed of powerful parts that form a whole; this notion is also applicable to transitions within health care systems. Drawing on these theoretical perspectives, we derived two assumptions that underpin the approach: (a) the fit between people and their environment is determined by understanding needs and expectations within the context of where care is received and provided and (b) transitional care processes are a personal experience that arise from multiple interactions (e.g., transfers, communication of information, and clinical interventions) within a journey of coming to, being in, and leaving a health care setting like the ED. Figure 1 is a representation of our theoretical perspective illustrating that when older people and the hospital environment come together, transitions occur that produce reinforcing consequences, which require adaptive responses from both the people and the environment.
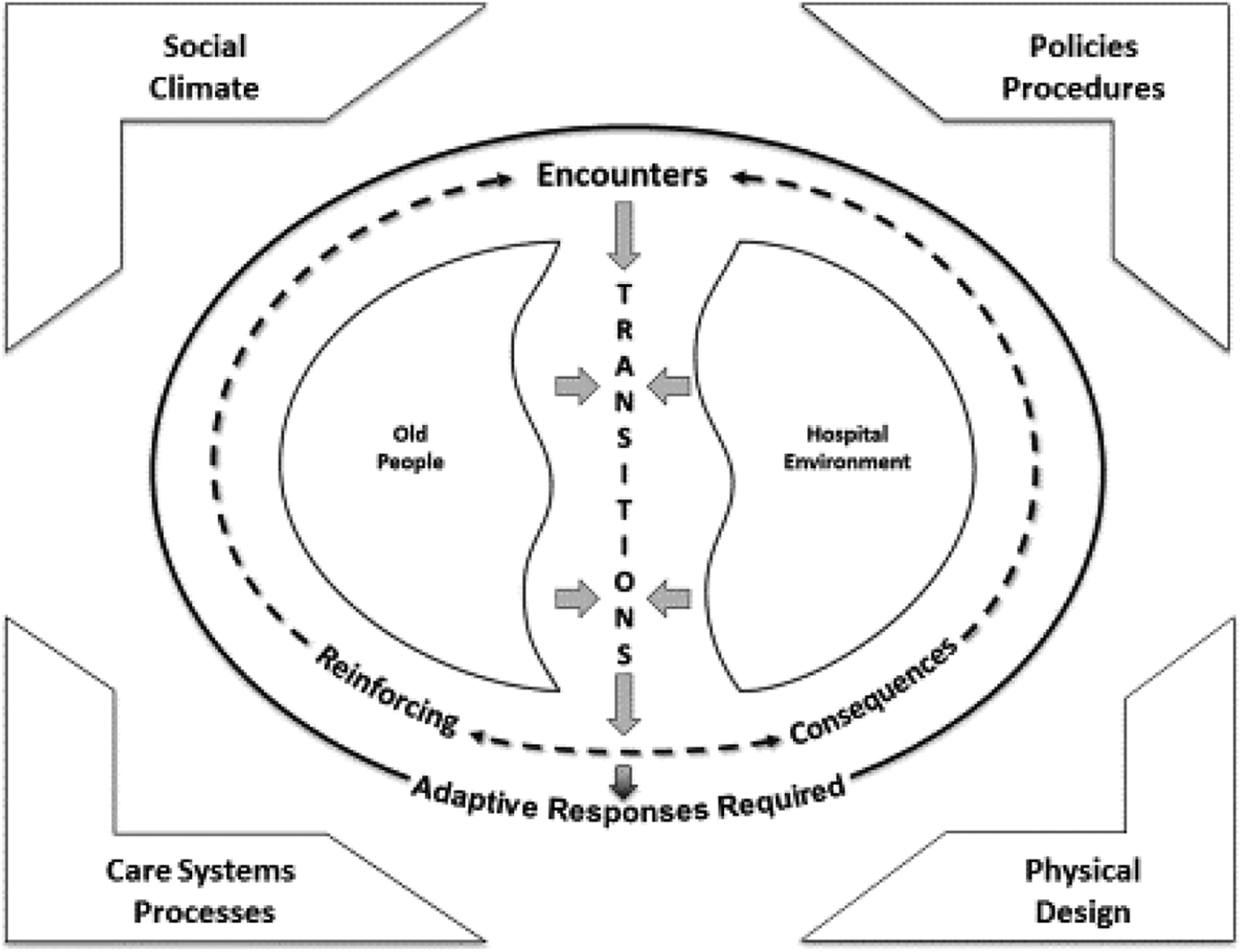
A social ecological model of older adult hospital environment fit. Adapted from Parke & Chappell, 2010.
Adaptive responses are needed because older people have altered presentation of disease and illness that may go unrecognized (depicted on the left sphere of Figure 1). The alteration in presentation may be compounded by dementia, a form of cognitive impairment known to cause clinical challenges for physicians and nurses (Parke, Beaith, Slater, & Clarke, 2011). As an example, difficulty arises when older people with dementia encounter the chaotic atmosphere of the ED. Finding new environments challenging, these older people may have difficulty communicating and become easily overwhelmed in a fast-paced ED. The ED hospital environment where complex interventions occur (depicted on the right sphere of Figure 1) is in continuous motion. The continuous motion represents factors from four dimensions: social climate, policy and procedure, physical design, and care systems and processes. These dimensions have been utilized in previous research to understand the dynamics operating in an elder-friendly hospital (Boltz, Parke, Shuluk, Capezuti, & Gavin, 2013; Parke & Chappell, 2010). Both older persons and the ED environment are mutually affected by both positive and negative reinforcing consequences that emerge when contextual factors from the four dimensions converge.
Methodological Approach
Our approach arose from a primary study conducted to understand the barriers and the facilitators to safe transitional care in the ED for those living with dementia. Data sources for the primary study were interviews with dyads (older adults living with dementia, n = 10; caregivers, n = 10), egistered nurses (RNs; n = 4), and nurse practitioners (NPs; n = 4). Photographic data were taken to simulate thematic events to create a photographic narrative journal (PNJ). The PNJ illustrated experiences in different locations of the hospital ED. The process of coming to, being in, and leaving the ED was identified from our analysis. The PNJ was then used in two photo elicitation focus groups: one with caregivers (n = 4) and the other with RN-NPs (n = 4). For a more complete report of initial results of this qualitative study, the reader is directed to Parke et al. (2013). We draw from this study to highlight examples of our approach.
Our research approach used a three-phase iterative process that combined interviews, photographic methods, and storyboarding techniques. Constant comparative analysis (Goetz & LeCompte, 1984; Loisell, Profetto-McGrath, Polit, & Beck, 2011) and coding (Miles, Huberman, & Saldana, 2013) were applied to all three phases. We used NVIVO 8 software to manage all interview data. See Figure 2 for the outline of our iterative three-phase approach.

Analysis Process. CCA = constant comparative analysis; PNJ = photographic narrative journal.
Phase 1: Individual and Dyad Interviews with Multiple Key Groups
Key participant groups are identified. In the primary study, they were characterized as a collection of individuals directly involved in a component of the ED journey (i.e., coming to, being in, and then leaving the ED). Specifically, older adult and caregiver dyads, RNs, and NPs (see Figure 2) made up the key participant groups instead of individuals from a “single”-oriented participant group (i.e., RNs or NPs or only older adult–caregiver dyads or caregivers themselves). This provided three data sets, which allowed us access to a range of perspectives to achieve maximum variation, not only within a single group but also across the groups. Although other professional groups such as physicians, physio therapists, and social workers could participate in future studies, our sample was determined by the goals of the primary study.
As required by the research ethics board, older adults with dementia had to be interviewed with their caregivers, hence older adult–caregiver dyads. Older adults with mild to moderate dementia were the primary participant group. These were individuals who retained verbal skills and the cognitive ability to express feelings about how it felt for them to experience an ED encounter. We gave precedence to the older person living with dementia by posing interview questions primarily to them rather than the caregiver.
Gaining consent from older people living with dementia is a complicated issue that is governed by legislation, which is enacted differently across international boundaries, and jurisdictions within a country (Sherratt, Soteriou, & Evans, 2007). We assumed in our research approach that a person has capacity until proven otherwise. This assumption is supported by geriatric best practice from multiple jurisdictions for determining informed consent prior to implementing a clinical intervention (National Institute for Health and Clinical Excellence, 2012; Schnitker, Martin-Khan, Beattie, & Gray, 2013). To explain, as in law for all adults, the older adult is competent until there is evidence to the contrary. Since there is no test for global competency, the “rule” used to adjudicate competency where participants are adults applies equally to older adults. Furthermore, where an individual has dementia, they may still have the “capacity” to understand and make certain decisions (Dewing, 2008; Sherratt et al., 2007). The issue of giving voluntary informed consent relates to their ability to understand what is being asked and the consequence of their decision to participate in the research (Dewing, 2008). Our approach included a research protocol to determine and document capacity. Previously published (Parke et al., 2013), the protocol involved what Dewing (2008) describes as process consent. Our approach was in keeping with the Canadian Tri Council Human Ethics Guidelines (Canadian Institutes of Health Research, Natural Sciences and Engineering Research Council of Canada, & Social Sciences and Humanities Research Council of Canada, 2010), recommendations from Alzheimer Europe (2014), and previous studies (Dewing, 2007; Hubbard, Downs, & Tester, 2003; McKeown, Clarke, Ingleton, & Repper, 2010).
Data analysis and outcome
Our analytic approach in Phase 1 involved two sequential activities. First, individual interview data were categorized into participant groups so that we could preserve what was germane to each single group. Team members individually coded and then as a team we clustered the codes within each data set separately (i.e., older adult/caregiver, RN, and NP) to arrive at specific themes for each group (see Figure 2). Analyzing data sets separately provided us an opportunity to work with more than one perspective in a single group. This allowed us to determine each groups’ views of the barriers and facilitators to safe ED care transitions. Team discussions were held to resolve disagreements and come to consensus on themes.
Second, beginning with the dyad themes, and then using the dyad themes that featured the older adults’ voice as the primary focus, we contrasted and compared those themes across the other two participant group themes (RNs and NPs; see Figure 2). This analytic technique permitted explorations of a range of similarities and differences across the groups to illuminate themes representing shared messages.
Phase 2: Photographic Storyboarding Technique to Arrive at a PNJ
We modified photographic research techniques (Harper, 2002; Lockett, Willis, & Edwards, 2005; Marck et al., 2006, Marck, 2010; Mitchell, 2011) and combined these with storyboarding techniques (Truong, Hayes, & Abowd, 2006). The use of these techniques enabled us to create the PNJ. The PNJ is a pictorial representation of ED care processes. We organized photographic scenes sequentially depicting “movement” through ED to illustrate a journey of coming to, being in, and leaving the department. To develop a PNJ, we progressed in four stages: scene development, pre-photo shoot activities, shooting the scenes in a natural setting of the ED, and a post-photo shoot analysis.
Scene development
The first challenge we faced was to authentically represent clinical transitional processes in constant motion rather than static events or separate environmental features such as a stretcher in a cubicle surrounded by medical paraphernalia. This required uncovering all facets of complex interactions between people and the environment together, as a whole system. We used the themes between and across data sets to arrive at shared messages (Phase 1 analysis). This analytic process assisted us to uncover and then select contextual factors relevant to the development of potential scenes.
We envisioned that showing people in interaction with the environment and with each other would bring focus to common experiences moving through the ED, while methodologically, setting opportunity for deeper discussion in Phase 3, the Photo Elicitation Focus Group (see Figure 2). We adopted storyboarding techniques to illustrate both positive and negative reinforcing consequences because it offered a means to match the narrative interview data with photographic sequencing to form a whole transition. Video data collection may have been a suitable solution to the challenge of capturing a transitional process but was not an option due to organizational constraints.
Developing a Storyboard
Storyboarding occurred once Phase 1 data analysis was complete. The process required writing scenes to provide insight into the complex factors operating between people (older adults living with dementia, caregivers, and the health care team) and the environment where care was received. Box 1 is the template we used for the creation of all scenes and illustrates a storyboard for the process of “being in.” The final step to storyboarding was to analyze the written scenes to ensure that the content represented the nuances of each theme.
Storyboarding Template for “Being in.”
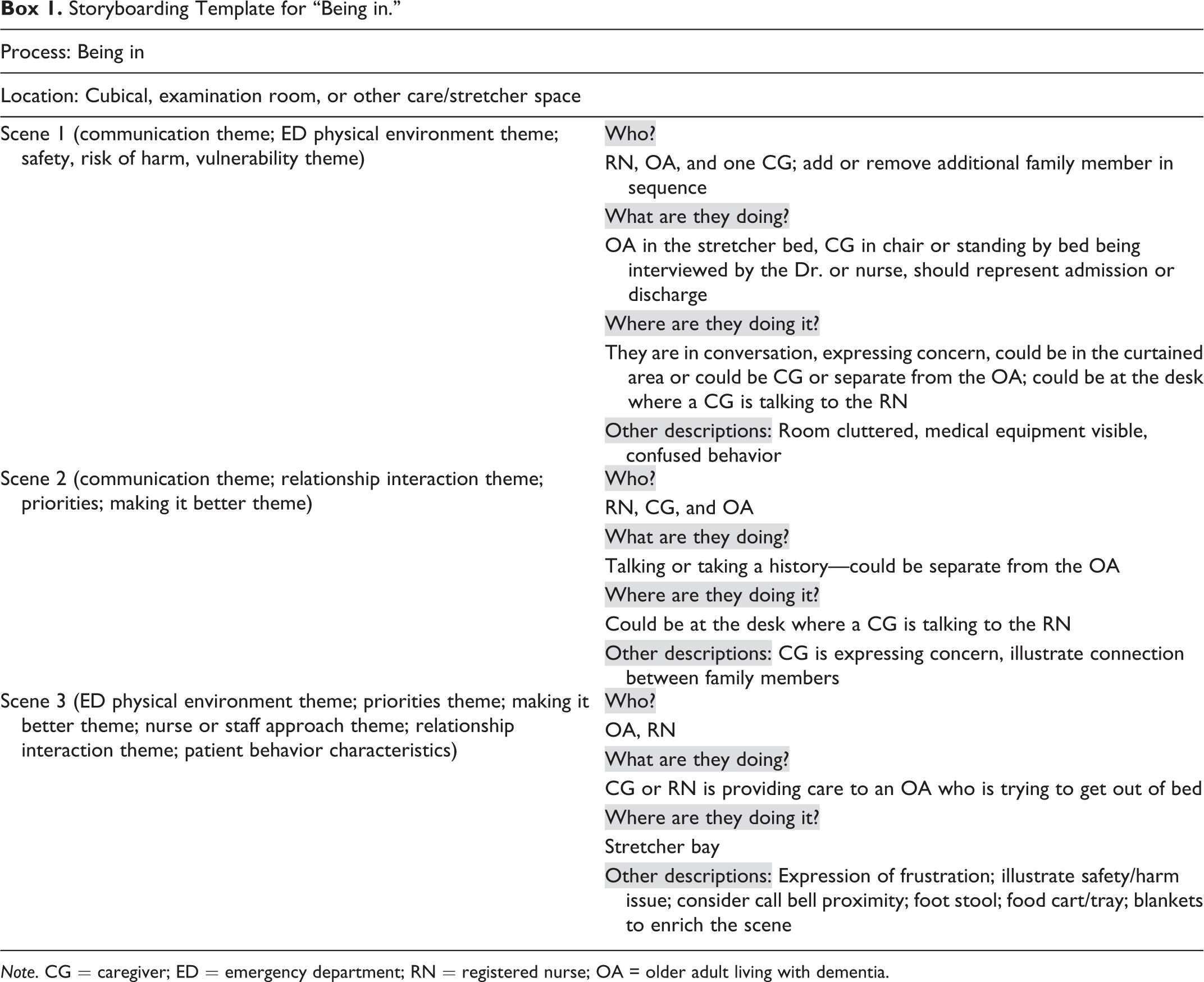
Note. CG = caregiver; ED = emergency department; RN = registered nurse; OA = older adult living with dementia.
Pre-photo shoot activities
In keeping with Mitchell (2011), our methodological decisions were informed with an appreciation for the nuances specific to the environment we were trying to investigate. Preliminary workup and preparation for entry into the natural setting was a distinct phase of our approach and included a pre-shoot visit to the site. We prepared to take pictures by getting to know the staff on-site, building relationships, and drawing on their wisdom. We established a local ED point-of-care research team consisting of the ED manager, clinical nurse educator, staff nurses, and geriatric team specialists to enhance collaboration and cooperation. This contributed to an insider’s versus an outsider’s view of the clinical setting. This also mitigated technical issues related to scene setup, available equipment, and camera angles and other theoretical composition factors.
Next we created descriptions of potential photographic scenes (see Box 1). Drawing from the work of Caulkins, Trosset, Painter, and Good (2000), we wrote a description for each scene that was based on the data from the primary study. Our methodological question at this stage was concerned with how to capture images in a way that would open up space for discussing the less tangible aspects of the ED experience captured in the themes from Phase 1 analysis. Examples of less tangible themes were communication and relationship building in the ED and a sense of “being cared for” or “being ignored or forgotten.” This was a key consideration because all data sets in Phase 1 showed that these relational themes were not merely peripheral but essential to successful and safe transitional processes for older adults living with dementia. Moreover, they were not static in any participants’ experience with an ED encounter. The relational themes became key elements of complex health care transitions for older people with dementia and their caregivers.
Writing the scenes involved a two-step process: first, determining the activities and processes relevant to coming to, being in, or leaving the ED. Second, as in Box 1, we identified who was in the scene, what they were doing, and the location of where the scene would occur in the ED (Parke et al., 2013). We adopted the term transition locus to distinguish smaller transitions occurring within care processes delivered in specific locations of the department from the overall experience of coming to, being in, or leaving the ED. This gave us the ability to analytically drill more deeply into specific events as experienced by our participants.
More than one scene was written for each transition locus. Storyboarding technique provided a means to mentally walk-through various transition loci to form a complete journey of an encounter prior to the photo shoot.
We considered a series of analytical questions in designing potential scenes (see Box 2). The point-of-care research team members were involved throughout the analytic process. The scenes were designed to represent common experiences (e.g., sitting in the waiting room in a wheelchair and lying in the cubicle with a family member and RN present) but also evoke new messages not yet identified. A spectrum of experiences occur in the ED, so we selected photographs that could be used to discuss alternative views on the same theme to gain variation in perspectives.
Point-of-Care Research Team: Pre-Photographic Scene Analytic Questions.

Note. ED = emergency department.
Shooting of simulation scenes in a natural setting of the ED
In the primary study, the scenes were staged in an urban ED for photographic data collection with research actors portraying RNs, older adults living with dementia, and caregivers. Eighty-six photos of planned scenes were taken during a 4-hr photo shoot. The photos were taken using a digital camera by a research assistant familiar with the scenarios and the intent of what was to be captured.
Each photo was numbered and catalogued on a data collection sheet according to a Phase 2 theme. Some scenes were shot more than once at different angles to address technical issues of flash, natural lighting, or glare on surfaces. All photographs were uploaded onto a research office computer for analysis.
Post-photo shoot analysis
All photographs were analyzed for content and visual significance. During this activity, analytic memos captured our emerging ideas of relevant themes. We then documented and analyzed our comments for each photograph in light of themes from Phase 1 and 2 data analyses (see Figure 2). This thematic analysis was then juxtaposed to the four dimensions of an elder-friendly hospital (social climate, policy and procedure, physical design, and care systems and processes) Parke, & Chappell, 2010).
We selected the highest quality photographs, which were determined by appearance and substantive nature of the content found within the photograph. We excluded photographs that represented too narrow an experience or had the potential to draw participant conversation away from the research question posed in the primary study. Our final decision was based on the potential of the photograph to yield further narrative depth. Each photo was reanalyzed according to the analytic questions in Box 1. As a team, we continually debriefed, worked to find consensus, and kept methodological field notes at different stages of the analytic process.
Illustrative example: Scene construction to theme
Photograph 1 simulates the theme, communication. Participants’ experiences fell along the continuum of believing staff were actively involved in information sharing with the caregiver and patient and being left alone, ignored, or uninformed during their visit. Communication and the experiences around staff engagement were areas where we decided to construct a scene about the facilitators and barriers to safe quality care.

Simulation of the communication theme.
We returned to storyboarding technique to sort and organize the still photographs into the transition locus of coming to, being in, or leaving the ED. A simulated example of “being in” is found in the photographic scenes noted subsequently. Our aim was to portray a whole transitional process through a sequence of individual pictures. Photographs 2a, 2b, and 2c simulate how storyboarding resulted in a series of three photos for one element of the transitional care process, being in, which became a section in the PNJ. The complete PNJ was taken to Phase 3 (see Figure 2).
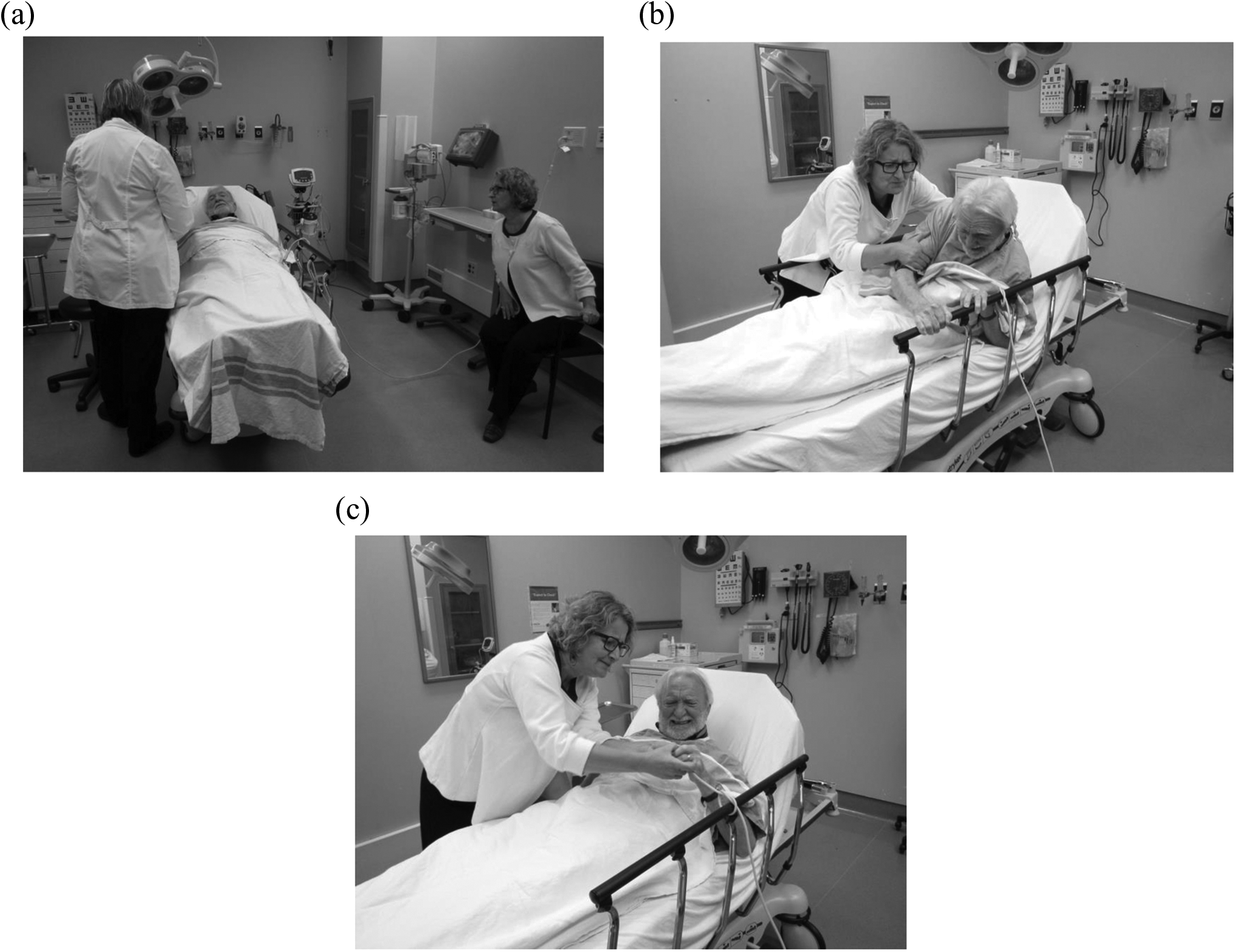
Illustration of Being In photographic Sequence, (a), (b) and (c).
Phase 3: Photo Elicitation Focus Groups
Phase 3 involved the use of the PNJ to facilitate two audio-recorded photo elicitation focus groups with a subgroup of Phase 1 participants (see Figure 2). Focus group method was selected because it offered the advantage of being efficient and cost-effective. As a data collection method, focus groups provided access to group interaction where participant synergy could bring about unanticipated information (Creswell, 2007). Generally, high face validity at low cost produces quick results on determining what participants see as important in the photographic images with the potential for emerging new ideas (Kidd & Parshall, 2000).
Our process for both focus groups, previously reported in Parke et al. (2013), involved systematically presenting the PNJ. The PNJ permitted participants to see the journey through the ED as a whole first, followed by a focused contextually based discussion on each transition locus using a semistructured guide specific to the dimensions of an elder-friendly hospital. The team was then able to verify, elaborate, and challenge emerging themes and relevant events identified in Phase 1 and 2 analyses.
It was impossible to fully anticipate what a participant might see in a photograph of the ED, or what memories, thoughts, or new ideas that the visual probe might evoke. This openness was most appealing about focus group as a data collection method in our overall approach. We hypothesized that a single photographic “scene” could be used as a focal point to explore multiple areas of interest. The older participants we targeted in the primary study had memory impairments but not to the point that they were unable to bring forth feelings that were evoked because of how they experienced the ED. We anticipated the visual cue of the photograph would elicit greater understanding through their ability to talk about what it felt like for them to be in the ED, although they might not remember the specific date or hospital.
Analyzing all the data to understand what solutions might interrupt iatrogenic harms involved matching the focus group data to the photographs and then using constant comparative techniques to the dimensions of an elder-friendly hospital (Parke, & Chappell, 2010). Once this process was completed for both focus groups individually, we integrated focus group data to arrive at one set of solutions for safe ED transitional processes for this population.
Rigor is inherent to our three-phase approach for the following reasons: triangulating data sources, peer debriefing, and multiple checks (Creswell, 2007). In addition, we maintained a methodological audit trail of decisions. The visual images were also used to validate preliminary themes, whereas the focus groups allowed us to elicit further feedback on safe transitional care in the ED.
Discussion
Our aim was to “hear the voice” of the older person living with dementia by including them as the primary participants. We were able to achieve this literally in Phase 1 data collection and the analysis. However, involving older adults living with dementia in Phase 3 photo elicitation focus groups became problematic. As previously reported (Parke et al., 2013), those who agreed to participate declined on focus group interview day because of ill health. Some caregivers were also concerned that a group interview would be too stressful for their family member. Although this effort meets the recommendation set forth by Alzheimer Europe (2014) that people living with dementia should speak for themselves, this was achieved only in part. Participation of older people living with dementia did not happen in Phase 3 focus groups. We believe however that we were able to capture their perspective in our PNJ.
While we were figuratively and literally able to include older people living with dementia in the first phase, questions remain: Does this actually constitute being able to “hear the voice” of older people living with dementia? Does this mean that their “voice” was only partially embedded in the approach we discuss in this article? We argue that Phase 1 is critical to our approach, and here, older people living with dementia personally contributed their own narrative data. Figuratively, their “voice” is represented and carried through all phases of the primary study because of the analytic power given to their contribution in Phase 1, and subsequently all methodological phases lead from their contribution.
Using photographs in research is not new. Previous studies have used photographs taken by participants, the researcher, a professional photographer, or already existing photos from archives or family albums to bring up memories or elicit comments from research participants (Mitchell, 2011; Pink, 2012; Riley & Manias, 2004). Photographic methods have also been used in early stage Alzheimer’s disease (Wiersma, 2011), understanding authentic partnerships (Dupuis et al., 2012), and the concept of leisure in dementia care (Genoe & Dupuis, 2013).
Visual methods provide greater person-centered data collection. Photographs, for example, exert a particular agency, and they play an active role in encouraging participants to recall certain events or encouraging them to consider the circumstances of events in ways they had not thought of before (Banks, 2001; Hartel & Thomson, 2011; Radley & Taylor, 2003a). These methods have the potential to provide direct understanding of illness and disease in the context of health systems and professional practices (Lorenz & Kolb, 2009). This can be accomplished because photographic images with text elicit deeper meaning than the written word contained in transcripts of in-depth interviews (Harper, 2002). Photographs combined with storytelling have the potential to uncover emotions and feelings that are difficult to express in words alone (Ortega-Alcazar & Dyck, 2012; Radley & Taylor, 2003b). This is in keeping with the strengths and abilities of older people living with dementia who encounter the fast-paced ED environment. Our approach mitigates the contextual circumstances that hinder this population from participating in research. We are able to access transitional processes in the ED for these people because “being-in” the ED is more than being located in a health care treatment setting. The photographs, therefore, support memory recall and provide context when they are discussed because they are a means to join the narrative with the objective world (Radley & Taylor, 2003a) as we did with the PNJ. Although our older participants may not have recalled specific dates and times, the PNJ evoked recall of feelings and emotions that illuminated how they were treated and what it was like for them to be in the ED receiving care in a health care system.
Health services research is dominated by biomedical perspectives that can unintentionally impede fully understanding the complex nature of dementia and dementia care (Bond & Corner, 2001). Photographic methods in social ecological research can facilitate investigating such complex health care system interventions. For example, photographic methods in studies of health care settings have been successfully used to illustrate and elicit data about medication safety in hospital and home care environments (Marck et al., 2006, 2010), children’s health issues (Clark & Zimmer, 2001), and care on hospital wards (Radley & Taylor, 2003b). Our approach extends the work of previous researchers by permitting access to processes of care that are fluid and in motion while at the same time capturing variability in the experiences of people who receive and provide care. Single, still photographs offer a static representation of phenomena, but sequenced in a PNJ with narrative elicitation opens the potential for a more holistic and flowing view of information when video data are unavailable.
We made use of the technique of storyboarding, which has a long history in the film and cartoon industry with application to other contexts (Dony, Mateer, & Robinson, 2005; Truong et al., 2006). For example, Barnes (1996) used the technique with university students to brainstorm elements of health promotion and wellness by organizing and prioritizing ideas. In another study, men were asked to take photos and organize the photos into a storyboard to document or represent their process through and experience of living with prostate cancer (Oliffe & Bottorff, 2007).
We found storyboarding a particularly useful technique for systematically integrating multiple data sets and different types of data to arrive at a cohesive whole. Storyboarding technique permitted an interpretation of reinforcing consequences and adaptive responses to uncover the best fit between older people living with dementia and ED, a complex heath care system. The ED context considered in this way shows that transitional care processes are not static or limited to service utilization or patient flow processes.
The theoretical perspective supports further understanding of factors in and among microsystems, mesosystems, and macrosystems. An in-depth analysis of context to reveal the arrangements of factors exerting influence on both a person living with dementia and the ED environment become exposed. This is an important feature in our approach because transitions occurring in health care settings impact the personal experiences of caregivers and health care professionals. Each group encounters positive and negative reinforcing consequence because of their interactions with the ED environment and with each other.
Our approach also facilitates the discovery of factors that were interdependent or adaptive and therefore amenable to change. Health-promoting solutions could be found in positive reinforcing consequences, and the harms found in the environment mitigated from producing negative reinforcing consequences. The theoretical positioning assisted us to unpack the complexity of these arrangements. We were positioned to ask methodological questions like are there characteristics about the older person living with dementia or the ED environment that evoke different responses by others (or even older adults themselves) when they encounter this practice setting? From this line of inquiry, investigating interactions across time and space (Lounsbury & Michell, 2009) become accessible.
Lessons Learned
Extensive preplanning is needed to ensure the best outcomes. If the analysis is weak or incomplete in Phases 1 and 2, the quality of photographs generated is diminished because the photographs lack substantive content. A strong relationship with local point-of-care research team members affects the quality of data and the depth of the analysis. Time must be spent investing in these relationships. Establishing point-of-care research teams in practice settings is a new way to bridge the research to practice gap and thus support reciprocal knowledge translation activity.
Researchers using this approach must consider their theoretical positioning, the timing and sequence of data collection, and the functional abilities of participants living with dementia. Although we considered functional abilities at the onset of the primary study, we recommend more attention to functional abilities be given throughout study when using this approach. Purposeful effort must go into matching the data collection setting and methods to the abilities of older participants living with dementia. From our experience, we believe this would strengthen authentic participation while accounting for progression of the disease. Although we see these as essential considerations, we acknowledge that they are not always predictable in advance across a study time line but worth ongoing consideration as the study evolves. In the future, we need to explore alternative ways to use in the PNJ for photo elicitation procedures with this group of older adults. Going forward into the future, we will explore other ways to involve older adults living with dementia in Phase 3. For example, returning to dyad interviews rather than attempting focus groups.
Conclusion
As Pauwels (2012) notes “Scholarly work, be it written, visual, or numeric, is not (just) about describing or reflecting aspects of the outer world, but about making it more revealing, accessible, insightful, and possibly more predictable or controllable” (p. 250). Our approach does this by drawing on the voices of those with dementia, a group often excluded from participating in studies about themselves. It is only those living and encountering the ED that can speak to their unique experience while also considering the impact of the context of others who also share the experience. We remain committed to finding approaches to further the researchers’ ability to “hear the voices” of those living with dementia.
Footnotes
Acknowledgments
We acknowledge the influence older people living with dementia have had on our thinking. Our desire to ensure that their voice is included in research-based practice change is based on our genuine belief that they offer important information to direct our nursing practice.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: It is acknowledged that funding was received for the original study where the approach that we have reported in this article was developed from: Alzheimer Society of Canada, CIHR, Parkinson Society Canada, and the Canadian Nurses Foundation. Grant # CPC-102349; RES0001383.