
Abstract
Pre-exposure prophylaxis (PrEP) exemplifies a medical advance that is highly efficacious in reducing an individual’s risk of acquiring HIV. However, the use of PrEP remains considerably suboptimal in communities that could benefit from it most, especially in the southern United States where HIV infection rates are highest. We conducted a study using both qualitative methods and implementation science to develop and deploy a multicomponent implementation strategy to link individuals being released from jail to PrEP services in a southern US city. Implementation science supports the translation of evidence-based strategies from clinical knowledge to routine use; simultaneously, qualitative methodologies, given their emphasis on “how” to advance adoption, execution, and sustainment, are critical to implementation science. Our study design for supporting individuals along the “jail-to-community continuum” was rooted in the EPIS (Exploration-Preparation-Implementation-Sustainment) framework and the socioecological model. We began with iterative qualitative data collection involving semi-structured interviews, focus groups, and a community summit with formerly incarcerated individuals, jail clinicians and staff, and members of community organizations who work with justice involved individuals and those who provide PrEP and related services. Following rapid qualitative analysis, we drew on implementation mapping principles to create an action plan that guided the development of implementation strategies for PrEP. Our analysis plan will evaluate the feasibility, effectiveness, and sustainability of our multicomponent implementation strategy. We conclude by offering recommendations based on lessons learned and reflect on the synergistic relationship between qualitative methods and implementation science.
Introduction
Pre-exposure prophylaxis (PrEP) exemplifies a medical advance that is highly efficacious yet widely underutilized. When taken as prescribed in its oral or injectable formulations, PrEP has the potential to significantly reduce an individual’s risk of acquiring HIV. While the oral formulations of PrEP are taken daily or peri-coitally, the long-acting injectable formulations are administered intermittently (i.e., every two months or twice-yearly). Individuals receiving any PrEP formulations complete routine testing for HIV infection and other sexually transmitted infections (STIs), and oral PrEP use is accompanied by laboratory testing for adverse effects. Previous studies have shown that PrEP can reduce the risk of acquiring HIV through sex by up to 99% and by at least 74% through injection drug use (Centers for Disease Control and Prevention, 2025; National Institutes of Health, 2023).
The demonstrated effectiveness of PrEP has made it a pivotal tool in efforts to end the HIV epidemic. Despite this evidence, however, the use of PrEP in communities that could most benefit from it remains considerably suboptimal, including particularly low use among women, racial and ethnic minorities, and in specific geographic regions like the southern United States, where HIV infection rates are highest (Carneiro et al., 2022; Centers for Disease Control and Prevention, 2023). Many factors contributing to PrEP underuse have been identified and characterized in prior studies, including its cost, insurance coverage limitations, HIV-related stigma, low health literacy, misunderstanding about HIV risk, and lack of training and engagement in PrEP among health care professionals (Killelea et al., 2022; Ojikutu et al., 2018; Pichon et al., 2022; Sullivan et al., 2019). Such factors span multiple ecological levels, making them complicated to address and requiring multifaceted efforts to overcome.
As a field of research, implementation science is focused on supporting the “movement of evidence-based, effective health care approaches…from the clinical knowledge base into routine use” (Rubenstein & Pugh, 2006). The field’s ultimate goal is to enhance the uptake and use of medical interventions, programs, and treatments – like PrEP – that have been rigorously tested and demonstrated to improve health and well-being. In this pursuit to enhance the reach and use of evidence-based interventions, implementation strategies are the “how to” of supporting change and consist of techniques that can be employed to enhance the adoption, implementation, and sustained use of an intervention, program, or treatment as part of routine practice (Proctor et al., 2013). Qualitative inquiry and the techniques of qualitative data collection and analysis – with their focus on answering “how” and “why” questions in rigorous yet pragmatic ways – are integral to implementation efforts (Hamilton & Finley, 2019), particularly when they are applied with an eye towards generating timely insights capable of guiding subsequent action. It is common for implementation strategies to consist of multiple components, and strategies should reflect the contexts in which they will be used and the needs and preferences of stakeholders in those contexts. Although there are robust approaches and established literature to guide the identification and operationalization of implementation strategies (Powell et al., 2015; Proctor et al., 2013), somewhat less common are published case studies that report the process and experience of implementation strategy development, including those that describe how qualitative data collection and analysis techniques can best be incorporated into the process for maximum impact. Such contributions to the literature can not only serve as potential exemplars for others to follow but can also help advance critical dialogue in the field about the role and opportunity for both qualitative methods (and by extension, qualitative methodologists) in the field of implementation science.
In this paper, we report our use of qualitative data collection and analysis techniques as part of the development of a multicomponent implementation strategy to support linkage to PrEP for justice-involved individuals being released from jail in an HIV “hotspot” city (i.e., a jurisdiction with high HIV incidence) in the southern United States. Our approach was informed by relevant theoretical perspectives, involved a multi-method formative evaluation, subsequent mapping exercises, and the development of an implementation action plan to guide our efforts in the jail setting. After presenting our approach, we discuss lessons learned and offer recommendations for other qualitative methodologists who are interested in implementation science and may seek to contribute to the identification and operationalization of implementation strategies for maximum uptake of evidence-based medical interventions, programs, and treatments.
Methods & Results
Design
We conducted a multi-method formative evaluation as the first of three aims in the “HOTSPOT” study, a
Prior to the launch of the HOTSPOT study and based on the existing literature noted above, we conceptualized the broad components of an implementation strategy that would be necessary to link individuals to PrEP services beginning when they entered the jail and forward through the time they were released to the community – a period that we referred to as the “jail-to-community continuum.” These components included (1) identifying individuals potentially at elevated risk for HIV but who are still HIV negative; (2) engaging those individuals while still in the jail to discuss PrEP; and subsequently (3) navigating those individuals who express interest to local community PrEP services upon release from the jail. These fundamental steps along the jail-to-community continuum offered a preliminary conceptualization of a multicomponent implementation strategy to support linkage to PrEP services, but one that would require operationalization and further context-specific tailoring.
The three specific aims of the HOTSPOT study are depicted in Figure 1, which illustrates how they were mapped to the Exploration-Preparation-Implementation-Sustainment (EPIS) Framework – our guiding framework. EPIS is a multi-level, multi-phase framework intended to represent the process of implementing an evidence-based intervention – PrEP in the case of this study – and the variety of factors that can impact that process (Moullin JC et al., 2020). EPIS was also originally developed to support rigorous approaches to implementation in public service sectors. Making it readily applicable to the jail setting in HOTSPOT. In this manuscript, we focus mostly on the role that specific qualitative data collection and analysis techniques played in Aims 1 and 2. In the pages that follow, we provide findings to illustrate, in detail, our approach and constituent steps for each of those Aims. Aim-specific approaches in the hotspot study mapped to the exploration-preparation-implementation-sustainment (EPIS) framework
Interviewers and facilitators of all qualitative data collection activities obtained informed verbal consent from participants prior to participation and audio-recording in accordance with the protocol approved by the Institutional Review Board (IRB) at the UT Southwestern Medical Center, STU 2021-0763 with site approval by Parkland Health. The IRB Committee includes an incarcerated individual representative, and all protocols were also approved by the Dallas County Jail correctional health leadership before beginning study activities. Locations for interviews within the jail were recommended by study personnel and approved by correctional health staff to meet the needs of confidentiality and safety of incarcerated individuals and interviewers. It has been our experience that verbal consent, which is typical and acceptable for interviews, is preferable for use with incarcerated populations to reduce anxiety related to the formality of written consent. Additional details related to the ethical considerations of this study can be found in our protocol manuscript (Nijhawan et al., 2025).
Data Collection
Aim 1: Assess Multi-Level Barriers to PrEP Care
Data collection in Aim 1 followed an exploratory sequential multi-method qualitative design (Fetters et al., 2013) to assess multi-level barriers to PrEP care. These activities comprised phase “E” (Exploration) of the EPIS framework, and included semi-structured interviews, a focus group, and a Summit event of community-based organizations.
Semi-Structured Interviews
Four individuals with postgraduate training in qualitative methods [RTH, ER, JL, MBT], conducted semi-structured interviews with members of three diverse stakeholder groups to obtain their unique perspectives about barriers to linking individuals recently released from jail to PrEP-related services. We interviewed: (1) employees at the local county jail, (2) formerly incarcerated individuals, and (3) members of community-based organizations that provide PrEP and HIV prevention education and services.
Members of the stakeholder groups expressed different views regarding barriers to PrEP services. One formerly incarcerated individual emphasized the stigma associated with having been incarcerated that followed him, making it difficult to secure housing and employment. “When a person gets out of jail or prison and they're looking for employment, employers turn their noses up. When the individual is looking for a place to live, the housing complex turns their noses up to them.”
In addition to stigma related to incarceration, community organization members observed that formerly incarcerated individuals could face multiple experiences of stigma that served as a barrier to PrEP care; these included stigma about being gay or transgender, being perceived as gay or transgender by being associated with an already-stigmatized illness (HIV) or medication (PrEP), having a substance use history, being poor, homeless, or unemployed, or being perceived as being sexually promiscuous. There’s a bunch of things that go into PrEP services that I think are not being discussed very openly, for multiple reasons, by different individuals. I think more conversation needs to be had around it all, not just incarceration, but like sexual stigmas, to the point where people are comfortable seeking therapy so that we can reduce the incidence of positive cases continuing to go up.
Beyond stigma, other barriers were commonly reported by individuals re-entering the community, especially lack of (or unstable) housing, lack of employment, unstable relationships, and lack of transportation. Securing shelter and a steady income were typically prioritized over addressing health-related needs, and sometimes it took months or even years to fully address basic health needs.
Focus Group
In addition to our Aim 1 interviews, the principal investigator, who is also trained in qualitative methods [AEN], conducted a focus group with members of the HIV/AIDS Re-entry Coalition, a group of county stakeholders committed to improving the care of individuals with HIV who are incarcerated or recently released from jail. During the focus group, some HIV/AIDS Re-entry Coalition members suggested a peer support strategy may be effective in reducing stigma and assisting recently released individuals in obtaining the PrEP-related services and other support they needed. Indeed, peer support has been documented in the literature to be a factor in reducing internalized stigma and preventing social isolation (Jones et al., 2025; Verinumbe et al., 2024). Right away, it’s an opportunity to build trust and to share something personal and really make it less stigmatized, things like that. “I don’t know about PrEP, but with recovery-oriented systems of care, peers helping peers has been one of the most effective things. And there’s a tremendous amount of research showing that peers are more open to sharing something with somebody and being open and discussing, and also having somebody to help them navigate the system.”
Summit Event
Our third and final Aim 1 activity involved conducting focus groups at an HIV Prevention Summit event to which we invited a variety of community members working in HIV prevention services across the county. The Summit was convened to understand members’ experiences navigating the dynamic landscape surrounding access to PrEP and HIV prevention resources more generally and to brainstorm strategies for collaborating across organizations to enhance engagement with initiation and maintenance in PrEP services. Focus groups were facilitated by investigators with qualitative expertise [TPH, RTH]. Financial barriers to PrEP were a prominent part of discussions among community members in attendance at the Summit. “We spend, I would say more than half of our time on prior authorizations for insurance. And then, if they deny it, then we'll do an appeal and sometimes they get approved, sometimes they don't.…The shortest time for a prior authorization could be five, 10 minutes and the longest, we're talking half the day. And even then, it's not even done, you're still having to wait until the answer comes a few days later. So, it can be a lot of time for just one person.”
In sum, as part of our Aim 1 exploratory phase, we pursued various qualitative data collection activities as part of our multi-method formative evaluation to assemble a large corpus of data regarding barriers to PrEP services. We analyzed these data in a three-step process in Aim 2, parts A, B, and C, in Preparation (“P” in the EPIS framework) for Implementation (“I” in the EPIS framework) and the testing of a multicomponent strategy intended to support linkage to PrEP in Aim 3.
Data Analysis
Aim 2: Refine the Implementation Strategy
Use Rapid Qualitative Analysis and Map the Implementation Strategies
Concurrent with data collection in Aim 1, we conducted rapid qualitative analysis (RQA) of the semi-structured interview data using a matrix that corresponded to the main questions in the interview guides. The RQA was thus primarily deductively driven by the jail-to-community continuum, the socioecological model of health, which is widely used to foreground the kinds of multilevel (e.g., (i.e., individual, interpersonal, and community/structural) factors that can influence health and health-related behaviors (McClay A et al., 2023; Reupert, 2017; Sallis et al., 2008), and a review of the literature on PrEP and health services for incarcerated individuals. We used RQA because our study required the translation of findings from Aim 1 to Aim 3 in the shortest amount of time possible. RQA reduces data from their narrative form to capture the main idea(s) expressed by each interviewed participant in response to a given question or subtopic (St George et al., 2023). Our RQA also enhanced rigor by facilitating consistent data capture across multiple analysts, promoting communication about findings among study team members in real time at weekly study meetings, identifying guide questions that seemed particularly useful in soliciting participant feedback, and assisting in determining when thematic saturation had been reached (Vindrola-Padros & Johnson, 2020).
Excerpt of Rapid Qualitative Analysis Matrix for Interviews With Formerly Incarcerated Individuals
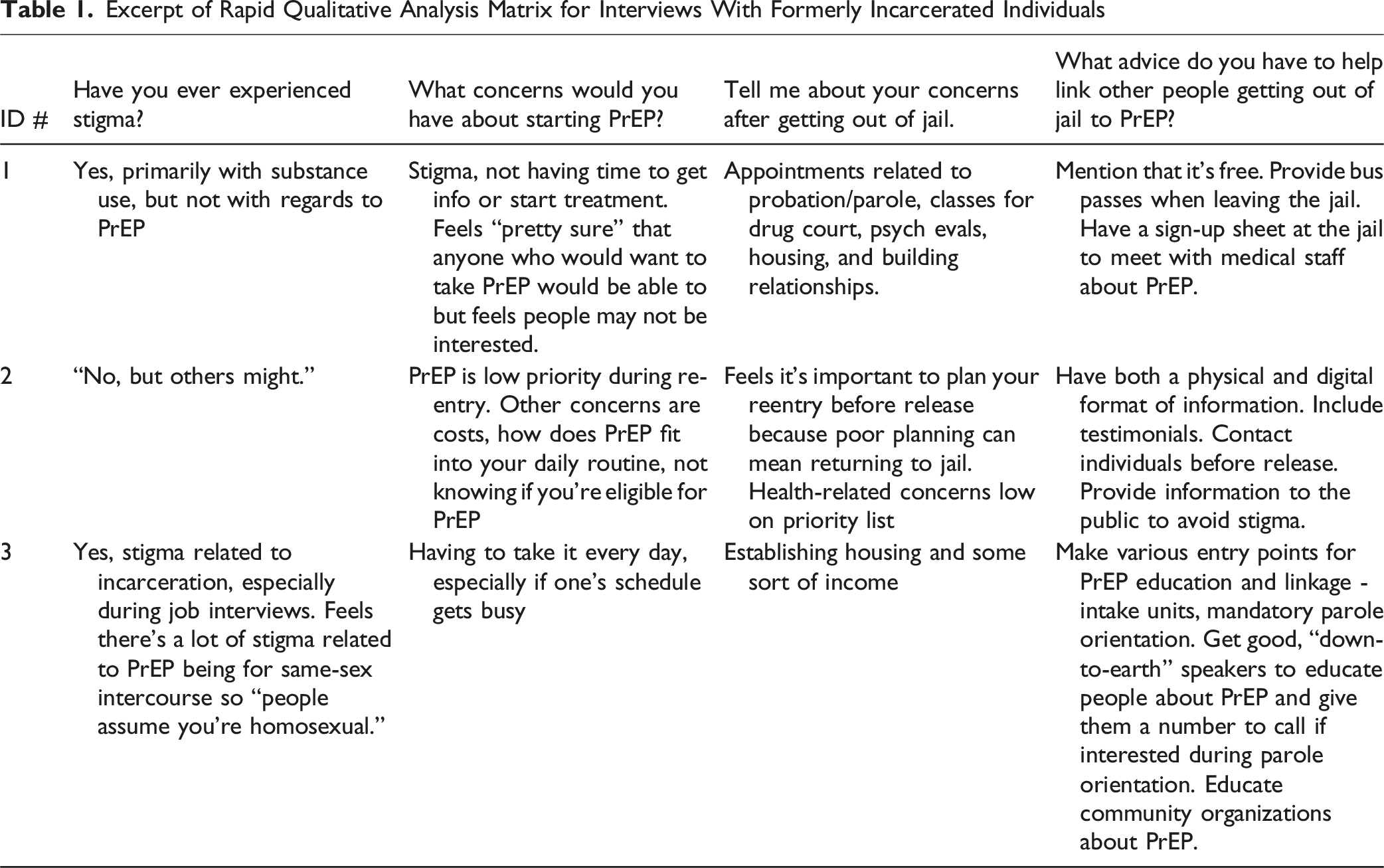
While the RQA led immediately to steps B and C below to quickly translate the Aim 1 findings to actionable strategies in Aim 3, research team members also conducted a separate thematic content analysis of data from the 27 transcripts. The thematic content analysis yielded rich narratives illuminating important contextual findings and experiences of participants, which are beyond the scope of this manuscript and have been reported elsewhere (Lee et al., 2025).
Excerpt of Barrier and Strategy Component Mapping

Develop the Implementation Action Plan
Excerpt of Implementation Action Plan

Discuss With Stakeholders
The overall purpose of sharing the implementation action plan was to take the component strategies that we created through our qualitative data collection and analytic procedures and “stress test” them with input from those working the frontlines of local HIV prevention, correctional, and community health. Discussion at these meetings was consensus-based and purpose-driven, the goal being to further synthesize our implementation strategy components in a lean, digestible format that could be readily used to facilitate communication with broader groups of frontline jail staff and community leaders.
We engaged various stakeholders in the review of our implementation action plan, including: (1) staff at our local safety net hospital system who were also members of a community health needs assessment team responsible for identifying the highest priority health issues facing local residents; (2) members of the HIV/AIDS Re-entry Coalition; and (3) leadership, clinicians, and staff of the county jail. Stakeholders were asked specifically about the potential feasibility and acceptability of our strategies from the perspectives of jail clinicians and staff, and staff from local community organizations. The discussions with members of the community health needs assessment team culminated in the development of the PrEP navigator protocol, engagement of the navigator in their education classes, referrals to the navigator, and assistance with follow-up on STI and HIV testing. Community based organization PrEP service providers facilitated on site visits from the jail PrEP navigator and established preferred communication strategies between the navigator and community organizations.
Aim 3: Deploy the Multicomponent Implementation Strategy and Assess Its Impact
Implement Strategies Outlined in the Implementation Action Plan
The implementation action plan that we deployed comprised several major components to improve the PrEP continuum of care. We first developed an automated algorithm that leverages electronic health record (EHR) data to estimate the risk for future HIV acquisition of all individuals in the county jail, which we use to identify potential candidates for PrEP. Variables in the algorithm include but are not limited to sex, gender identity, race, ethnicity, age, sexual orientation, history of incarceration, history of HIV testing, and history of positive sexually transmitted infections (e.g., syphilis, chlamydia, gonorrhea). This prediction model is designed to improve the efficiency with which the limited HIV prevention resources of the county jail are deployed, including which specific individuals are prioritized for HIV testing and discussions about PrEP. We also architected processes for identifying individuals for PrEP discussions through receipt of referrals from clinicians and health educators who interact with incarcerated individuals around sexually transmitted infections and sexual health care.
We then hired, trained, and deployed a PrEP navigator who engages individuals during their incarceration, provides them with information about PrEP, assesses their interest in PrEP use, and links them to clinical care for PrEP after community re-entry, as appropriate. Our navigator is an African American female with experience in data science and a focus on community health, and we have found that her empathic, non-judgmental approach and other interpersonal characteristics have allowed her to rapidly build rapport and successfully complete PrEP discussions with a majority of individuals whom she meets. These characteristics facilitate navigator-client trust, excellent communication, and adaptability when operationalizing workflows in the busy jail setting. Her approach is informed by the implementation action plan and involves meeting with patients after they have been assigned housing within the jail, assessing their risk for HIV, providing PrEP education tailored to patient’s literacy level, collecting detailed contact information, providing referrals for patient-reported barriers to care (e.g. health insurance, housing, re-entry services) and providing a warm handoff to preferred PrEP clinics for those interested in receiving PrEP.
In addition, ongoing and future implementation activities include the development of posters and flyers related to HIV/STI testing and PrEP to be displayed at the jail, providing PrEP education sessions to jail clinicians, expanding referrals to the study navigator to include individuals who test positive for STIs, and expanding referrals for patients to free or low-cost phone services to improve post-release communication with the navigator.
Evaluate Implementation, Effectiveness, and Sustainability Outcomes, the Integration of These into Routine Processes, and the Duration of Their Effects
Given our hybrid implementation-effectiveness study design, our primary evaluation metrics include implementation and effectiveness outcomes over a 24-month study period. Our main effectiveness outcomes will be improvements in testing for HIV and other sexually transmitted infections in the county jail and referrals to community healthcare service providers and prescriptions for PrEP (Nijhawan et al., 2025). For implementation outcomes, including how well our strategy components are integrated into routine processes at the county jail, we will track use of our automated prediction algorithm to identify candidates for PrEP and the navigator’s ability to engage and navigate individuals who are referred to her. The navigator is using a secure web-based application (REDCap) to track her activities, including but not limited to counts of individuals appropriate to approach, efforts made to reach them, and counts of those individuals she is able to engage. Such data has potential to inform resource allocations and future planning for any further scale-up of our implementation strategy beyond this study. The navigator also keep a log of her experiences in the role, including challenges encountered and success stories, takes fieldnotes to assist in contextualizing outcomes, and incorporates feedback from direct observations by other research team members to improve her communication and workflow efficiency. Such information can be invaluable to the training of future HIV-prevention navigators working in justice-involved settings. At the time of this writing, data collection as part of the hybrid implementation-effectiveness trial has begun, and our early review of data quality suggests that we are likely to be successful in collecting the kinds of data necessary for rigorous evaluation of both our effectiveness and implementation outcomes. After our main study period, we will continue to track our full suite of outcomes for an additional six months to learn more about the sustainability of our implementation action plan after the resources from our research study, including salary support for a PrEP navigator, are no longer available.
Discussion
This paper presents a case study applying qualitative methods to advance the real-time design of an implementation strategy for linking justice involved individuals at risk for HIV to PrEP care. Our approach was theoretically grounded and employed multiple qualitative data collection and analysis approaches as part of several constituent steps: (1) gathering data from key stakeholders through varied qualitative approaches (individual semi-structured interviews, focus groups, stakeholder summit) to understand multi-level barriers to PrEP care; (2) conducting rapid analyses of these data to generate actionable insights for implementation strategy design; (3) drawing on implementation mapping principles to further specify the strategy components; (4) drafting an implementation action plan; and (5) vetting the action plan and implementation strategy components it contained with stakeholders. At present, our implementation action plan and component strategies are being deployed as part of the HOTSPOT study’s hybrid implementation-effectiveness trial. In time, we will better understand the extent to which its strategies were (or were not) effective at enhancing linkage to PrEP care for this extremely vulnerable population. Prior studies have directly compared different qualitative analytic approaches to gauge their relative performance and contributions to broader implementation initiatives (Brown et al., 2025; Gale et al., 2019; Nevedal et al., 2021). While it was not possible to draw such comparisons in the present study due to time and resource constraints, we offer a detailed case study showcasing the application of qualitative methods for others who may seek to apply them in the context of broader implementation initiatives.
As others have noted, the lengthy data collection and analytic periods that often characterize traditional qualitative methods may have the unintended consequence of spurring the very evidence-to-practice gap that implementation science seeks to overcome (Beidas et al., 2022; Brown et al., 2025). For this reason, there is increasing discussion of pragmatic approaches to using qualitative methods in the context of implementation that are intended to simultaneously address both research and practice goals (Ramanadhan et al., 2021). Such pragmatic approaches increase the likelihood that the crucially important contributions that qualitative data collection and analysis techniques have to make to implementation science – revealing complex processes, understanding contextual factors, and pinpointing ways to enhance implementation success (Hagaman et al., 2021) – are fully realized.
We began the HOTSPOT study with a general conceptualization of implementation strategy components, based on the existing literature, which would be necessary to link justice-involved individuals to PrEP services beginning when they entered the jail and forward through the time they were released to the community. The jail-to-community continuum provided our team with a foundation from which to launch a multi-method formative evaluation, grounded in qualitative methods, to move from this general conceptualization to an accessible implementation action plan based on a thorough assessment of barriers, facilitators, timing, and feasibility. We recognize that the case study we have presented is an inherently prospective approach to implementation strategy development, which has been previously criticized for assuming that context is static and unchanging (Lewis et al., 2018). While we agree this is a shortcoming, we also feel that our close partnership with frontline staff and leadership at the county jail and our rapport with community organizations has provided open feedback loops which have supported iterative refinements to our component implementation strategies. Moreover, we speculate that our involvement of key stakeholders from the settings that are so central to forging linkages to PrEP care for justice-involved individuals may also be fueling a sense of investment in the HOTSPOT study efforts (e.g., Lewis et al., 2018). Since the start of our hybrid implementation-effectiveness trial, our PrEP navigator has received multiple referrals from jail staff members regarding individuals who they feel may benefit from increased awareness of and education about PrEP. Lastly, our implementation action plan and component strategies appropriately reflect the challenges of establishing linkages to PrEP care with a highly vulnerable population faced with assorted competing demands in a sociopolitical environment that poses still further multilevel challenges.
Several strengths of the methodological approaches we report here may be applicable in other settings. First, we leveraged an interdisciplinary team approach including infectious disease physicians, implementation and qualitative research scientists, an epidemiologist, informatician, and statistician, in addition to multiple research staff. Given the large scope of the study, it was important to achieve both scientific rigor and efficiency; hence, we conducted a rapid qualitative analysis to expedite translation of data collection findings to the eventual implementation action plan. Importantly, we enlisted feedback from dozens of stakeholders from the jail, community members in diverse roles, and formerly incarcerated individuals, throughout our implementation strategy development process to promote both relevance and sustainability. Our study was informed by theory, but we also exercised practicality when needed. For example, we learned that the county jail’s EHR system would be transitioning to a new platform midway through the evaluation phase of our study, which would impact the availability of data for our HIV risk prediction model. Our team proactively worked with the information technology experts at the county jail to devise novel approaches to maintain access to critical data across new as well as legacy datasets. An essential component of implementation research is this kind of ability to adapt, retain flexibility, and find alternative means to meet study goals when needed.
This study has several limitations. First, our research team first drafted the implementation action plan based on weekly group discussions about the potential feasibility of strategy components and related resource constraints. Lewis et al. (2018) followed a more structured approach to implementation action planning including the use of Likert scale ratings (Lewis et al., 2018). One disadvantage of collecting only qualitative data, as we report here and has been done in other studies (e.g., (Zbukvic et al., 2022), is that fewer data overall are collected. Yet, the literature is unclear about how different approaches ultimately translate to the sustainability of evidence-based practices over time. Second, to comment on our implementation action plan, we engaged stakeholders from the county jail, providers of services for justice-involved individuals, and community members involved in the delivery of PrEP and related services. However, we did not gather stakeholders from the different groups together at the same time, potentially missing opportunities for cross-pollination of ideas or opportunities to identify concerns about feasibility or impacts of certain implementation strategy components on other sectors of the community. Third, this study aimed to demonstrate how qualitative methods can be utilized as part of larger implementation studies to inform implementation strategies intended to support maximum uptake of evidence-based interventions. It is noteworthy, however, that an undertaking like ours required direct, intensive participation by two faculty and three research staff with expertise in qualitative methods and/or implementation science plus weekly engagement with multiple other faculty and stakeholders who comprised the investigative team. As prominent qualitative methodologists have noted, RQA does indeed place a premium on organization and teamwork (Hamilton & Finley, 2019). It would be difficult to replicate our approach without a similar level of interdisciplinary expertise and team member involvement. Lastly, we conducted our multi-method formative evaluation using diverse qualitative data collection and analysis techniques prior to the publication of tools like the Planning and Assessing Rigor in Rapid Qualitative Analysis (PARRQA) (Kowalski et al., 2024), which are intended to enhance methodological quality and rigor; thus, we are pleased that the majority of those best practice recommendations are documented in our methods.
Conclusions
We set out to determine what implementation strategies would best improve linkage to PrEP among recently incarcerated individuals in a large southern US city, and how best to accomplish those strategies. In this case study, we have tried to illustrate how qualitative methods are integral to answering these and other fundamental implementation-related questions. Our experiences in the HOTSPOT study underscore that RQA, mapping techniques, iterative, stakeholder-driven refinement, and other qualitative approaches have the potential to provide the kinds of rich, nuanced insights necessary to inform subsequent action in near real time. As pressure mounts to realize healthcare improvements through enhanced evidence-based practice, there will undoubtedly be a critical need for qualitative methodologists to further deploy these methods effectively and shape their use for maximum impact. In so doing, qualitative methodologists can play a critical role in furthering the uptake of medical interventions, programs, and treatments – like PrEP – and to the advancement of the implementation science field more generally.
Footnotes
Acknowledgments
We would like to acknowledge Asharhri Falls and Marlon Brown for their participation and contributions to the success of this project.
Ethical Considerations
All participants gave informed verbal consent prior to participation in interviews and focus groups, in accordance with the protocol approved by the Institutional Review Board at the University of Texas Southwestern Medical Center (STU, 2021-0763) and site approval by Parkland Health in July 2024.
Author Contributions
Conceptualization: AEN, DK
Methodology: RTH, TPH, AEN, DK
Validation: RTH, TPH, AEN, DK
Investigation: RTH, ER, JL, MBT
Writing-original draft: RTH, TPH, AEN, DK
Project administration: MBT
Funding acquisition: AEN, DK
Formal analysis: all authors, Writing-review and editing: all authors
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was primarily supported by the National Institute of Mental Health (NIMH), R01MH129185-01 (MPI: Nijhawan/Krakower). We also received support from UT Southwestern’s Clinical and Translational Science Award Program (CTSA), NIH UL1TR003163. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Krakower has conducted research with funding from Gilead Sciences and Merck to his institution, has received personal funds to develop medical education content for Medscape and UpToDate. Inc., and has received support from PrEP4All for travel to a conference on a national plan for HIV pre-exposure prophylaxis. Dr. Nijhawan and Dr. Higashi have conducted research with funding from Gilead Sciences to their institution. All other authors assert they have no relevant conflicts of interest to disclose.
Data Availability Statement
The data that support these findings are not publicly available due to IRB-related concerns regarding the protection of participants’ confidentiality, but may be available from the corresponding author, upon reasonable request.