
Abstract
Cardiovascular disease (CVD) remains the leading cause of death and disability worldwide, with aging populations posing increasing challenges to healthcare systems. Recovery from acute myocardial infarction (AMI) requires compliance to treatment and lifestyle changes, but few patients comply with prescribed regimens. Participatory health research (PHR) has emerged as an effective approach for involving healthcare professionals and patients in jointly identifying root causes of problems, defining solutions, and evaluating interventions. This collaborative engagement fosters the development of more effective and sustainable outcomes. In clinical settings, the implementation of PHR presents both challenges and opportunities. This article offers a critical reflection on a PHR conducted with cardiology nurses in Portugal. The aim was to co-identify and co-develop solutions to the issue of low patient compliance following AMI, using the Ishikawa diagram as a co-reflective tool. This study used a participatory health approach and a qualitative design, incorporating focus groups supported by the Ishikawa diagram to identify the causes and potential solutions to low patient compliance after AMI. The cardiology nursing team (n = 16) identified factors influencing low patient compliance after AMI, categorized into patients, healthcare professionals, procedures, facilities, and policies. Proposed solutions include personalized education, improved hospital-PHC communication, resource optimization, and the need for patient-centered policy reforms. This reappraisal of a participatory study with cardiology nurses reveals both the promise and constraints of participatory health research in clinical settings. Meaningful engagement requires trust, transparency, ethical reflexivity, and recognition of systemic boundaries. While not all co-created solutions were implementable, the process generated critical insights and momentum for ongoing change. Future participatory projects must balance aspiration with structural analysis, ensuring that collaborative inquiry is both ethically grounded and strategically impactful.
Introduction
Cardiovascular disease (CVD) remains the leading cause of mortality and a major driver of disability in modern times. As populations age and survival rates improve after initial cardiac events, the burden of disability-adjusted life years continues to rise, posing significant challenges for healthcare systems (Byrne et al., 2023).
Recovering from an acute myocardial infarction (AMI) requires a comprehensive care plan that includes adherence to a structured therapeutic regimen (patient compliance) and the adoption of sustainable lifestyle modifications (Ski et al., 2023). Secondary prevention programs play a pivotal role after a cardiovascular event, offering cost-effective strategies that can be as critical to survival as the treatments provided during the acute phase. Implementing these interventions promptly is essential to optimizing outcomes and preventing recurrence (Byrne et al., 2023; Visseren et al., 2021).
Encouraging patient compliance, and maintaining over time, plays a crucial role in reducing the risk of recurrent cardiovascular events following AMI (Byrne et al., 2023). EUROASPIRE V study highlights that many coronary patients maintain unhealthy lifestyles, including smoking, poor dietary habits, and physical inactivity, which negatively affect key cardiovascular risk factors. Many also fail to meet targets for blood pressure, low-density lipoprotein cholesterol, and glucose levels (Kotseva et al., 2019).
Medication adherence in secondary prevention is also a significant challenge, with only 66% of patients maintaining optimal compliance, mainly due to polypharmacy, the complexity of drug regimens, challenges in the doctor–patient relationship, insufficient patient-centered care, difficulties in accepting the disease, concerns about side effects, cognitive impairments, mental and physical health conditions, financial constraints, social isolation, and depression (Byrne et al., 2023).
Compliance to prescribed treatments or lifestyle recommendations is influenced by complex psychological factors, making it essential to adopt a whole-systems approach. This involves educating health professionals, using patient-reported outcomes (PROM) and experience (PREM) measures, prioritizing patient education, and ensuring care is centered around the patient’s needs (Byrne et al., 2023; Ski et al., 2023).
Understanding the healthcare professionals’ perspective and collaboratively identifying the reasons behind low patient compliance after AMI, as well as potential solutions, can be fundamental in engaging the team in continuous improvement efforts. Ishikawa diagram (or root cause analysis) is a widely used quality method to understand what is happening, identify why it is happening, and determine measures to prevent recurrence (Harel et al., 2016).
This study aims to explore the perspectives of cardiology nurses regarding potential causes of low patient compliance after AMI. Insights gained from the focus group discussions, using the Ishikawa diagram, will help identify key areas for improvement in hospital discharge practices. These findings, allong with other ongoing studies from Cardiac Integrated Care project (Homem et al., 2024), will serve as a base for co-creating patient-centered solutions that prioritize care quality, enhance clinical outcomes, and improve patient satisfaction. In conclusion, we will critically reflect on the implementation of participatory research, highlighting both the challenges encountered and the opportunities it offers for improving clinical practice.
Methods
Study Design
This study represents an initial phase of the Cardiac Integrated Care project (Homem et al., 2025), a participatory health approach, which aim to design and assess an integrated care initiative that bridges cardiology and PHC. Its goal is to enhance care transitions and foster therapeutic self-care for individuals recovering from AMI. To achieve this, a multidisciplinary research team has been established, comprising various experts healthcare professions (field experts cardiology and PHC nurses, cardiologists, general practitioners, and hospital and PHC pharmacists) along with representatives from patient organizations.
For this specific study, a qualitative approach was used by using the Ishikawa diagram in a focus group. This allows a better identification of the reasons behind low patient compliance after AMI, as well potential solutions and determining measures to prevent recurrence (Harel et al., 2016).
Ishikawa diagram or root cause analysis is a straightforward and widely used method for identifying quality issues. In the context of quality improvement, this approach is based on the idea that addressing the fundamental factors contributing to a specific outcome can lead to effective solutions (Harel et al., 2016; Watson and Spiridonova, 2019).
The focus groups, supported by the use of the Ishikawa diagram, were conducted during an in-service training session with all 16 cardiology nurses from a hospital in central Portugal in two moments.
Sampling and Setting
All cardiology nurses were recruited (n = 16). Regarding the participant’s composition, it consists of 1 man and 15 women, including 7 specialist nurses and 9 generalist nurses. Among them, 1 have less than 10 years of experience in cardiology, 8 have more than 10 years, and 7 have over 20 years of experience in the field.
The focus group sessions took place in a private and comfortable meeting room within the hospital, ensuring an appropriate environment for discussion. The sessions were facilitated by FH, a specialized nurse and PhD student, and AC, a specialized nurse and MSc student. Both facilitators were well-acquainted with the participant group and experienced in the focus group methodology. AC supported the primary moderator by observing the sessions, taking detailed notes, and assisting with the overall proceedings.
Data Collection and Analysis
The focus groups were conducted by FH and assisted by AC, using the Ishikawa diagram, on April 9 and May 14, 2024, and lasted an average of 45 minutes each. No participants refused to take part in the study.
The sessions began with a presentation by the moderator, including a brief overview of the purpose, an emphasis on the importance of participants’ contributions in identifying key areas for improving hospital discharge practices, and an explanation of how participants’ anonymity would be safeguarded.
The sessions were not recorded to foster a more open and relaxed environment, encouraging participants to share their opinions and ideas freely. Recording can sometimes hinder spontaneity and honesty, particularly when sensitive topics are being discussed. Instead, the observer documented the sessions through detailed field notes, capturing contextual and non-verbal elements that are crucial for understanding how participants’ contributions relate to the diagram (Nyumba et al., 2018).
Following the presentation of the Ishikawa diagram, participants were invited to reflect on potential causes of low patient compliance after AMI. To aid this process, yellow and green post-it notes were distributed to the participants.
Initially, participants were asked to write their thoughts on yellow post-it notes without identification, which were then collected. The moderator read the notes aloud and, through discussion with the group, grouped them according to the categories of the Ishikawa diagram: patients, healthcare professionals, procedures, facilities and resources, and policies. As the discussion progressed, additional ideas were introduced.
After discussing the identified causes, participants were asked to write possible solutions to the previously identified causes on the green post-it notes. The post-its were then collected, read aloud by the moderator, and regrouped according to the same axes.
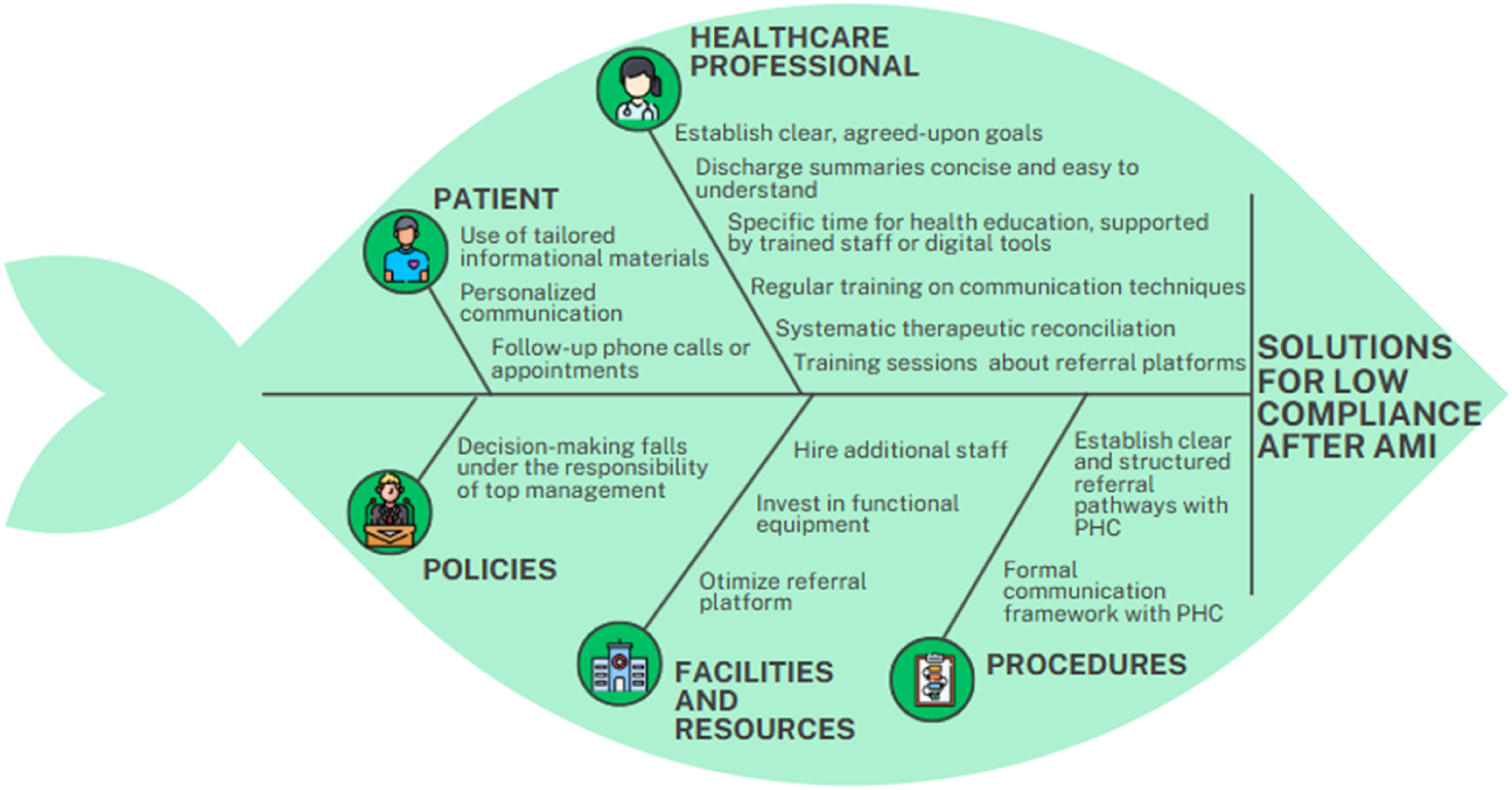
In this regard, two diagrams were created: one with the causes (Figure 1) and another with the potential solutions (Figure 2). By the end of the session, the team collaboratively developed strategies to improve hospital discharge practices. Potential Causes for Low Patient Compliance after AMI Possible Solutions to the Identified Causes for Low Patient Compliance after AMI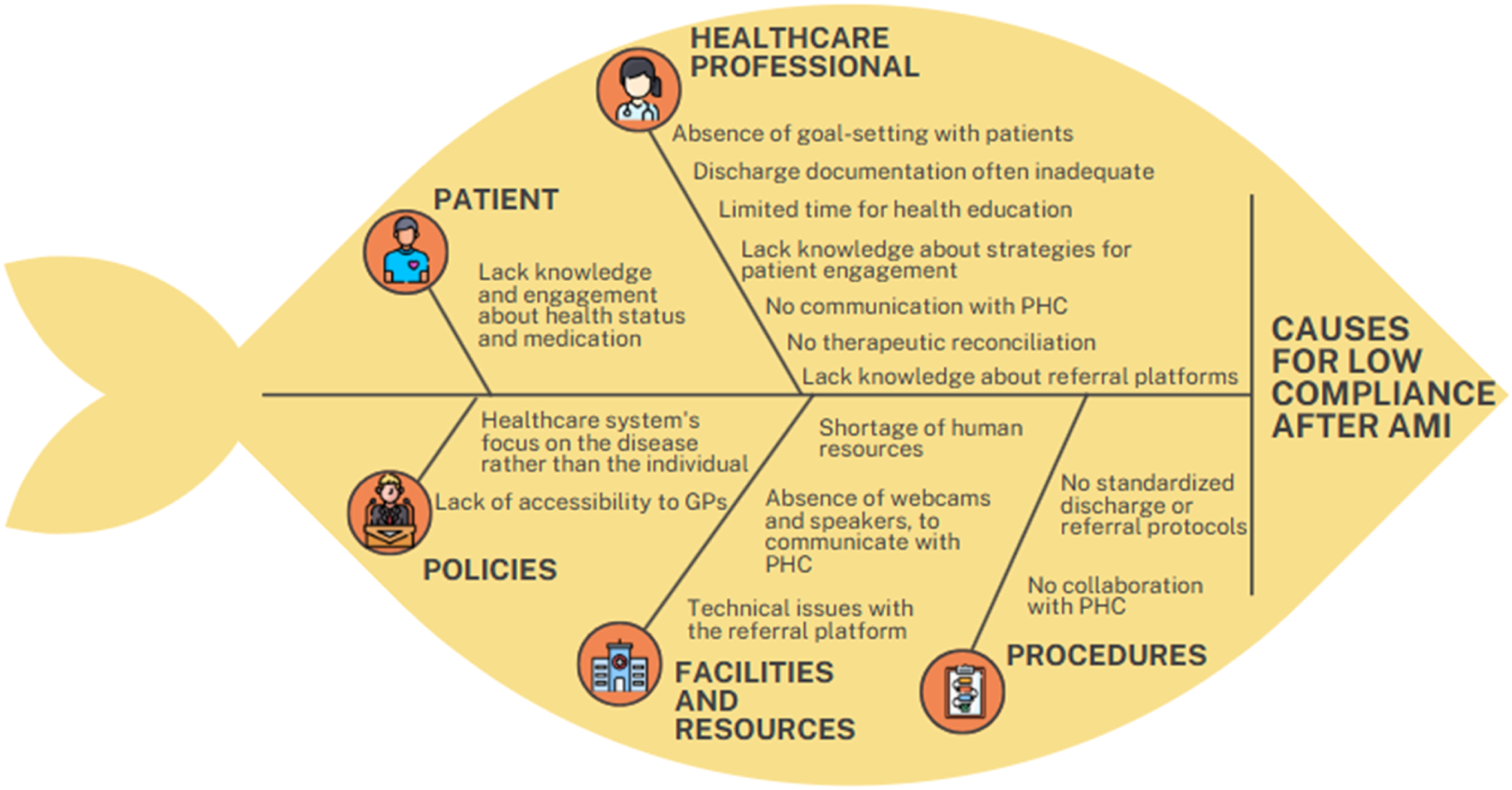
Results
The findings were grouped into the categories of the Ishikawa diagram: patients, healthcare professionals, procedures, facilities and resources, and policies.
Patients (Causes)
Regarding the low patient compliance after AMI, cardiology nurses report that many patients demonstrate a lack of knowledge and engagement about health status and medication, with limited involvement in their healthcare process and often struggle to accept their current health condition. This is often accompanied by a poor understanding of their medication regimen, as well as a lack of motivation and information on the importance of following prescribed treatments. Nurses emphasize that patients frequently underestimate the role of a proper healthy lifestyle and medication in managing their condition, along with the long-term implications of heart disease. As one statement highlights, “Low health literacy, particularly regarding common conditions such as diabetes, hypertension, and heart failure” is a significant contributing factor. This lack of knowledge and engagement with their treatment plan often leads to poor compliance, ultimately hindering long-term management and recovery.
Patients (Possible Solutions)
To address the lack of patient knowledge and engagement about health status and medication, several solutions have been suggested by cardiology nurses, to improve patient understanding, engagement, and motivation.
One solution is enhancing patient education through tailored informational materials. Nurses have found that providing clear, easy-to-understand resources helps bridge the gap in health literacy. As one nurse stated, “Using the hospital televisions to display information about disease management allows us to provide education passively, while still engaging patients when they have questions.” These resources include visual aids and step-by-step guides on managing medications, recognizing symptoms, and making lifestyle changes such as improving healthy habits.
In addition, there is an emphasis on personalized communication. Nurses highlight the importance of one-on-one counselling sessions to discuss the patient’s concerns, address misconceptions, and offer emotional support. A cardiology nurse noted, “By taking the time to understand each patient’s specific situation and concerns, we can motivate them to take ownership of their health.” Regarding medication compliance, one nurse stated that “Educating patients about the purpose, and possible side effects of each medication during hospital administration, is essential to improve compliance.”
Another critical strategy is the use of follow-up phone calls or appointments. Regular check-ins provide opportunities to monitor patient progress, offer reminders about the importance of compliance, and offer encouragement. According to one nurse, “Patients are more likely to stick to their treatment plan when they feel supported and accountable through consistent follow-up.”
Furthermore, improving motivation through behavioural change techniques, such as goal setting and positive reinforcement, has proven beneficial. Nurses emphasize the need to celebrate small victories, such as consistent medication intake or improved diet, to boost patient confidence.
Healthcare Professionals (Causes)
Regarding the low patient compliance after AMI, cardiology nurses report several factors related to healthcare professionals. One major issue is the absence of goal-setting agreements with patients. As one nurse explained, “Without clear, agreed-upon goals, patients struggle to understand the importance of adhering to their treatment plan.” Nurses also note that discharge documentation is often inadequate, which complicates follow-up care. “The discharge documents are often too long with much information that they do not understand, making it difficult for patients to understand the necessary next steps in their treatment,” one nurse mentioned.
Additionally, limited time for health education plays a significant role. “Sometimes we simply don’t have enough time to provide in-depth health education during our shifts,” another nurse remarked. This lack of time further contributes to the issue, as patients may leave the hospital without a full understanding of their condition and treatment.
Another factor is the lack of knowledge about the best strategies for patient engagement. “Sometimes, we don’t have the necessary tools or training to effectively communicate with patients about their treatment,” noted one nurse. Moreover, there is no communication with PHC, which could provide ongoing support after discharge. “Without communication between the hospital and PHC, patients may not receive the follow-up care they need,” a nurse pointed out.
Furthermore, there is no therapeutic reconciliation during hospitalization, leading to potential discrepancies in medication management. “Patients often question, ‘Why haven’t I been given the medication for my prostate yet?’ or ‘I’m used to taking this medication in the morning, not at night.’ Situations like these undermine the credibility of healthcare professionals and confuse the patients.” emphasized one nurse.
Lastly, there is a lack of information about referral platforms, which hinders the seamless transition of care. As one nurse explained, “I came across a new application for referring patients to PHC while writing a discharge note, but I don’t know what to write or what timelines to use.”
Healthcare Professionals (Possible Solutions)
To address the challenges identified by cardiology nurses regarding low patient compliance after AMI related to healthcare professionals, several solutions can be proposed.
One effective approach is to establish clear, agreed-upon goals during the hospital stay. “Setting realistic and individualized goals with patients ensures they understand the importance of compliance and feel actively involved in their care,” one nurse suggested. This could involve creating written agreements that outline specific treatment milestones and expectations.
Discharge summaries should be concise and easy to understand, tailored to the patient’s literacy level. “We can implement standardized templates that include essential information in simple language, supported by leaflets to make instructions clearer,” proposed a nurse. Additionally, providing patients with a checklist of immediate and long-term agreed-upon goals can enhance their comprehension. Creating feedback loops where patients can share their experiences post-discharge could help identify gaps in care and refine strategies. “Patients should be encouraged to provide feedback on their understanding of instructions and satisfaction with the discharge process,” a nurse suggested.
Allocating specific time slots for health education, supported by trained staff or digital tools, could address the issue of limited time during regular shifts. “Using the hospital televisions to display information about disease management allows us to provide education passively, while still engaging patients when they have questions.”
Healthcare providers should receive regular training on effective communication techniques and strategies for improving patient engagement. “Workshops focused on motivational interviewing and emotional intelligence can help us better connect with patients and address their concerns” a nurse suggested. Training could include real-life scenarios to build confidence in managing complex interactions.
Strengthening the connection between hospitals and PHCs through referral protocols is essential for seamless continuity of care. “Developing a structured referral process can ensure PHCs have the information they need to provide follow-up care” one nurse emphasized. Regular meetings or updates between hospital teams and PHCs could further improve communication and create synergies.
Introducing systematic therapeutic reconciliation during hospitalization can help prevent medication discrepancies. “By involving a multidisciplinary team to review and align medications, we can ensure patients receive the correct prescriptions and reduce confusion after discharge” one nurse suggested. This process could be complemented by a patient-facing medication schedule to clarify dosage times and purposes.
To address the lack of information about referral platforms, training sessions should be provided to familiarize staff with these tools. “Providing practical training on referral applications and establishing clear guidelines for timing and content would make it easier for us to use these platforms effectively” one nurse recommended.
Procedures (Causes)
Several procedural shortcomings significantly contribute to the low patient compliance after AMI. One major issue is the absence of standardized discharge or referral protocols. “Without clear referral pathways, patients are often left without adequate follow-up care or guidance once they leave the hospital” noted one nurse. This lack of structure creates gaps in care continuity, leading to confusion and a higher likelihood of non-compliance.
Additionally, there is no established collaboration between cardiology and PHC. “The lack of communication and coordination between cardiology and PHC means that patients are not consistently supported in managing their condition post-discharge,” explained another nurse. This disconnect often results in patients feeling isolated and uninformed about their treatment plans.
Procedures (Possible Solutions)
To address the procedural shortcomings contributing to low patient compliance after AMI, several solutions can be proposed.
Establishing clear and structured referral pathways between cardiology and PHC is essential. As said before “Developing a structured referral process can ensure PHCs have the information they need to provide follow-up care”. These protocols should include detailed steps, timelines, and responsibilities for each healthcare provider involved. Establishing feedback systems to regularly review and improve referral and discharge protocols can ensure their effectiveness over time. “Collecting feedback from both patients and healthcare professionals allows us to identify gaps and make necessary adjustments,” suggested a nurse.
Creating a formal communication framework between cardiology and PHC is critical for improving care continuity. “Regular meetings and shared electronic health records would allow for seamless information exchange and better patient monitoring,” emphasized another nurse. This collaboration could include joint care plans, shared access to patient data, and defined roles for follow-up appointments. Providing training sessions for healthcare professionals on how to use referral platforms effectively is another key solution. This training could also address common challenges and provide ongoing support for staff.
Facilities and Resources (Causes)
The lack of adequate facilities and resources plays a significant role in the low patient compliance after AMI. One primary issue is the shortage of human resources. “We often don’t have enough staff to provide the necessary time and attention for patient education” a nurse explained. This understaffing limits the ability to ensure patients fully understand their treatment plans and the importance of compliance, particularly during the discharge process.
Another challenge is the absence of functional equipment, such as webcams and speakers, to facilitate communication with PHC. “Without proper tools for virtual communication, it’s nearly impossible to coordinate effectively with PHC teams” emphasized one nurse. This lack of technological infrastructure hinders the ability to provide real-time support and collaborative care, both of which are critical for ensuring compliance.
In addition, technical issues with the referral platform exacerbate the problem. “The referral platform doesn’t work. I tried using it and followed up with the patient, who mentioned they were never contacted by the PHC” another nurse noted. This disruption creates significant gaps in care continuity, leaving patients without the necessary support and guidance after hospital discharge.
Facilities and Resources (Possible Solutions)
To address the facility and resource limitations that contribute to low patient compliance after AMI, several solutions can be implemented:
Hiring additional staff is essential to ensure sufficient time for patient education. “With more personnel, we can dedicate the necessary attention to educating patients“ suggested one nurse. Increasing the workforce would also alleviate the burden on existing staff, enabling them to provide more comprehensive and personalized care.
Investing in functional equipment, such as webcams and speakers, is critical for improving communication with PHC. “Providing the right tools for virtual communication would allow us to coordinate seamlessly with PHC teams” emphasized another nurse. These tools can facilitate remote consultations, case discussions, and real-time problem-solving, enhancing the transition of care. Long-term advocacy for increased funding and investment in healthcare infrastructure is essential. “We need to push for better resource allocation to ensure hospitals and PHC have the equipment and staff needed to support patients effectively” a nurse emphasized. Partnerships with governmental and non-governmental organizations could provide additional funding and resources for these initiatives.
Otimizing the referral platform is paramount for streamlining the transition of care. This can include software updates, system testing, and user feedback to ensure the platform functions effectively. Training sessions for staff (hospital and PHC) on how to use the platform efficiently would further enhance its impact. Establishing feedback mechanisms to identify and address gaps in the referral process can enhance accountability and reliability. “Patients should have a way to report if they haven’t been contacted by PHC, so we can follow up and resolve any issues” noted a nurse. Regular audits and patient satisfaction surveys can also ensure continuous improvement in the process.
Policies (Causes)
Policy-related factors significantly impact the patient compliance after AMI. One major issue is the healthcare system’s focus on the disease rather than the individual. “The current approach prioritizes treating the condition over addressing the person’s unique needs and circumstances” noted one nurse. This disease-centered model often overlooks the importance of patient-centered care, where understanding the patient’s lifestyle, barriers, and motivations is key to ensuring compliance.
Another challenge is the lack of accessibility to general practitioners (GPs), which hinders patients’ ability to receive ongoing support and follow-up care. “Many patients report difficulty in scheduling timely appointments with their GPs, leaving them without the guidance they need after discharge” explained a nurse. This limited access increases the risk of poor management of symptoms and misunderstanding of the treatment plan, contributing to non-compliance.
Policies (Possible Solutions)
Regarding policies, the nursing team unanimously agreed that proposing measures beyond their scope of decision-making falls under the responsibility of top management. “It’s not within our authority to implement changes at the policy level; these decisions rest with top leadership” one nurse explained.
The team emphasized that while they can identify issues and suggest improvements, such as enhancing patient-centered care or increasing accessibility to family physicians, implementing these changes requires strategic decisions at higher organizational levels. “Our role is to advocate for our patients and highlight the barriers we observe, but ultimately, it’s up to leadership to take action,” noted another nurse.
Discussion
The findings highlight significant challenges and potential solutions for improving patient compliance after AMI. Categorization these challenges into patients, healthcare professionals, procedures, facilities and resources, and policies underscores the multifactorial nature of non-compliance.
Patients
A recurring challenge is the difficulty patients face in understanding their condition and the critical importance of treatment compliance. This is consistent with evidence linking low health literacy to poor health outcomes. Limited knowledge about conditions such as AMI, diabetes, and hypertension has been shown to negatively impact compliance to prescribed medications and lifestyle modifications (Guo et al., 2023). Patients with low health literacy are more likely to misinterpret medication instructions, fail to recognize symptoms and neglect essential follow-up care.
Tailored educational interventions, as suggested by participants, offer a promising solution to address these gaps. Systematic reviews highlight the effectiveness of patient education programs that combine written materials with verbal explanations and visual aids (9). For instance, delivering educational content through hospital televisions has been shown to improve knowledge retention. Additionally, follow-up interventions, such as phone calls or telemonitoring, have proven effective in reinforcing patient compliance (Homem et al., 2024; Huriani et al., 2022).
Beyond education, shared decision-making (SDM) has emerged as a key patient-centered strategy. SDM involves collaborative clinical decision-making that integrates the patient’s preferences, values, and goals with the best available scientific evidence and the expertise of healthcare professionals. This approach is especially relevant in cardiology, where managing complex conditions like heart failure, hypertension, and coronary artery disease requires active patient engagement. Research shows that patients involved in decision-making are more likely to adhere to prescribed treatments, which is essential for preventing adverse events and achieving optimal long-term outcomes (Himmelfarb et al., 2018).
Recognizing the importance of SDM, leading organizations such as the European Society of Cardiology (ESC) and the American Heart Association (AHA) emphasize its role, particularly in decisions involving invasive procedures or long-term pharmacological therapies c By fostering collaboration, SDM not only supports patient autonomy but also empowers individuals to take an active role in managing their health, thereby addressing a key determinant of patient compliance.
Healthcare Professionals
The identified barriers align with evidence showing that time constraints are a significant obstacle to patient education (WHO, 2023). Poorly structured discharge summaries further contribute to fragmented care transitions and reduced compliance (Ski et al., 2023).
Simplifying discharge documentation through standardized templates, as suggested, aligns with evidence advocating for structured and patient-centered discharge processes (Byrne et al., 2023; Ski et al., 2023). Studies show that concise, easy-to-understand summaries improve patient comprehension and engagement (Byrne et al., 2023). Regular training on communication techniques, such as motivational interviewing, has been shown to improve patient-provider interactions and compliance (WHO, 2023). Workshops on communication techniques and SDM can also enhance clinicians’ ability to engage patients in meaningful discussions (Byrne et al., 2023).
Therapeutic reconciliation, an evidence-based intervention involving a systematic review of patients’ medications during care transitions, has been show to reduce discrepancies and improve patient compliance (Lee et al., 2017).
Procedures
The absence of structured discharge and referral processes contributes to care discontinuity, a well-documented barrier to patient compliance (Ski et al., 2023). Poor coordination between cardiology and PHC exacerbates the issue, leaving patients without the necessary post-discharge support (WHO, 2018). Developing clear referral pathways and enhancing communication between cardiology and PHC align with the principles of integrated care (Ski et al., 2023). Evidence from successful models, such as the “Care Transitions Intervention,” highlights that structured protocols and follow-up systems significantly reduce readmissions and improve compliance (Powers et al., 2014).
Facilities and Resources
Staff shortages and inadequate resources are common challenges in healthcare systems worldwide. Research links these issues to reduced quality of care and lower patient compliace. Increasing nurse staffing ratios has been shown to improve patient education and outcomes (Yoon, 2022). Similarly, equipping facilities with functional communication tools, such as telehealth technologies, enhances coordination between care teams (Byrne et al., 2023; Homem et al., 2024; WHO, 2019).
Policies
The current focus on disease rather than patient-centered care reflects a broader challenge in healthcare systems. Evidence supports the transition to patient-centered models, which emphasize holistic, individualized care and shared decision-making (Byrne et al., 2023; Ski et al., 2023).
Policy reforms are essential to enhance accessibility and continuity of care. Increasing the availability of general practitioners (GPs) and ensuring timely appointments are critical, as primary care access is a key determinant of improved chronic disease management (WHO, 2018).
Challenges in Implementing Participatory Health Research
This study highlights several critical insights and challenges encountered in implementing Participatory Health Research (PHR) within clinical settings.
One central theme was the importance of building relational trust. A scoping review by Gilfoyle and colleagues (2022) explores how trust is conceptualised, operationalised, and measured in PHR, emphasizing the relational dynamics within collaborative partnerships. While the participants were health professionals, they often operated within an institutional framework that excluded them from strategic decision-making processes. Trust was cultivated through pre-existing relationships between facilitators and participants, as well as by creating familiar and comfortable environments. This required a deliberate effort to promote transparency, shared leadership, and genuine engagement throughout the process.
Ethical dilemmas, particularly around informed consent in dialogical practices, also emerged as a key issue. The decision not to record focus group sessions reflected a commitment to ethical reflexivity, prioritizing participant comfort over comprehensive data collection. This aligns with the broader concept on “process consent,” which view consent as an ongoing, reflective, and ethical dialogue between researchers and participants, rather than a one-time procedural formality (Mondragón-Barrios, 2009).
Reciprocity was a guiding principle, but its limitations became clear throughout the study. While nurses contributed significantly to identifying problems and suggesting solutions, the implementation of policy-level changes was largely beyond their control. This highlighted the importance of managing expectations and clearly communicating the boundaries of localized agency, even within participatory frameworks.
Despite these challenges, the study demonstrated the potential of collective action to generate meaningful local impact. Nurses were actively involved in the co-identification of challenges and the co-creation of solutions to improve hospital discharge practices. This engagement reflects the core principles of PHR (ICPHR, 2021), emphasizing empowerment as both a process and an outcome. By strengthening personal and collective capacities, participants gained a sense of agency while reflecting critically on their roles within institutional structures. This participatory and dialogical approach allowed nurses to better understand the systemic factors affecting patient care.
However, consistent with PHR literature, the study also recognized that transformational change requires more than localized action. It necessitates broader organizational commitment and structural reform, especially to address systemic issues like fragmented communication between hospitals and primary care. While the research process empowered participants to articulate these challenges and envision improvements, actual change at the policy or structural level depends on institutional will and cross-sector collaboration. This underscores the need for participatory efforts to be integrated within wider health governance strategies.
A significant risk in PHR is disempowerment, especially when participants invest time and effort but see limited follow-through. The study mitigated this risk by fostering honest discussions about institutional constraints and framing the initiative as one phase in a longer journey toward change. This approach helped maintain motivation and ensure realism among participants.
In dealing with the potential risk of pseudo-participation and greenwashing, the study explicitly addressed tensions surrounding tokenism and limited power. Facilitators were transparent about which aspects of care could be influenced and which remained outside the group’s control. This openness preserved the integrity of the process and differentiated genuine co-production from superficial consultation.
Additionally, the study revealed persistent power dynamics and positionality even within the same professional category. Nurses expressed feeling undervalued by policymakers, and the participatory process offered a rare opportunity to voice systemic frustrations. These intra-professional dynamics echo broader critiques of epistemic injustice within institutional structures, where certain voices are often marginalized.
Efforts to promote equity within participatory practices included valuing the experiential knowledge of nurses and co-developing patient education strategies tailored to individual needs. However, entrenched hierarchies remained evident, particularly in policymaking, where nurses had limited influence. The findings support the need for greater inclusion of frontline staff in institutional planning and decision-making. For instance, a participatory action research project involving a nursing team in a Dutch geriatric rehabilitation center found that a supportive learning environment, regular reflection, and collaboration could empower nurses to take ownership of care improvements. However, systemic barriers such as lack of protected time and weak links to organizational quality policy limited the impact (Vaalburg et al., 2024)
Throughout the study, researcher accountability and reflexivity were essential. Facilitators, who were themselves embedded in the same professional context, maintained continuous awareness of their dual roles as insiders and researchers. Strategies such as using anonymous post-its and participant-led categorization of discussion themes were employed to minimize facilitator dominance and promote inclusive participation.
Finally, the use of visual tools, such as color-coded post-its and the Ishikawa diagram, played a pivotal role in supporting collaborative inquiry. These methods helped externalize hidden knowledge, visualize complexity, and encourage non-linear, emergent thinking among participants. By making abstract concepts more tangible, these methods enhanced group reflection and fostered a more engaging and inclusive co-production process (Salvati, et al., 2023).
Conclusion
This study highlights the importance and challenges of implementing PHR in clinical settings. Building relational trust, continuous ethical reflection, and fostering genuine participatory processes were essential for the success of the initiative. Despite limitations in terms of policy and structural changes, the active participation of healthcare professionals, such as nurses, demonstrated the potential of collective action to generate meaningful local impacts. However, issues such as pseudo-participation, power dynamics, and the need for greater inclusion of frontline professionals in institutional decision-making highlight the complexity and challenges of the co-production process. The use of visual tools, such as the Ishikawa diagram, was a crucial resource in promoting collaborative reflection and visualizing complex solutions. Ultimately, the study underscores the need to integrate participatory practices within broader health governance strategies, recognizing that transformative change requires wider organizational commitment.
Footnotes
Acknowledgements
The authors would like to express their gratitude to the ULS Coimbra Cardiology team for their commitment and motivation in achieving better care for citizens.
Ethical Consideration
Ethical approval was obtained from the ULS Coimbra Ethics Committee (2024-2-ESI.SF) on March 8th 2024.
Consent to Participate
The participation was voluntary, and those who agreed provided written informed consent.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article.