
Abstract
Photovoice (PV), a Community-based Participatory Research (CBPR) method, has been used to better understand the lived experience of homelessness. As part of PV, participants use photography to capture phenomena of importance, engage in critical dialogue and analysis, and communicate findings to policymakers and the community. This paper examines: (1) the methodology for recruiting individuals experiencing homelessness (IEH), (2) innovative and emerging applications of PV for capturing lived experiences during a pandemic, (3) strategies for designing partnerships between multi-sectional organizations, (4) the application of infection prevention and control protocols, (5) the use of robust, collaborative data analysis methods, (6) approaches for disseminating and implementing key findings, and (7) lessons learned. Conducting a PV study with IEH can present challenges and as a result, such studies often have small sample sizes (6-13 people). This study was able to recruit and engage 38 participants across multiple sub-populations of IEH during a global pandemic. Partnerships between a healthcare organization, community organization focused on addressing local homelessness, shelter and service agency staff, community members interested in assisting with the study, and a software development company were integral to the success of the project. Participants provided input on how they would like the study findings shared with the public and were invited to join planning meetings for public presentations. Future PV studies conducted among populations experiencing homelessness should consider strategic involvement of partners at various levels (service providers, community members, and participants).
Background
PhotoVoice (PV) is a Community-based Participatory Research (CBPR) methodology that uses photography to enable people to document community strengths and concerns, engage in critical dialogue and analysis, and communicate findings to policymakers and leaders (Wang & Burris, 1997). The PV methodology is rooted in three foundational theories (Wang & Burris, 1997): (1) education for critical consciousness (Freire, 2021), (2) expression and notions of voice (Hooks, 1981; Liebenberg, 2022), and (c) participatory photography documentation (Ewald et al., 1985; Hubbard, 1994). Helpful to understanding a particular phenomenon from the perspective of individuals and groups most affected, PV has been employed in different research areas such as nursing (Close, 2007; Riley & Manias, 2004), psychology (Brunsden & Goatcher, 2007; Pickin et al., 2011), incarcerated children and youth (James & Olausson, 2018), and homelessness (Bukowski & Buetow, 2011; Hodgetts et al., 2007).
Individuals experiencing homelessness (IEH) are often without access to traditional modes of communication and participation in society, making PV an appropriate method to better understand their lived experiences (Cheezum et al., 2019; McKinsey et al., 2021; Pruitt et al., 2018). Because these individuals’ voices often go unheard, PV allows access to visual imagery to communicate experiences and concerns to the community (Halifax et al., 2008), especially when experiences are difficult to describe in words. Researchers employing PV to examine the lived experiences of IEH have noted its ability to foster empowerment (Halifax et al., 2008), a sense of purpose (Pruitt et al., 2018; Wang & Burris, 1997), environmental awareness (Dixon & Hadjialexiou, 2005), and social support (Dixon & Hadjialexiou, 2005; Pruitt et al., 2018; Seitz & Strack, 2016).
Despite these benefits, conducting a PV study with IEH can be difficult to execute because of the transient, unpredictable, and traumatic nature of homelessness (Seitz & Strack, 2016). Common challenges include: high attrition, inconsistent attendance, lost cameras, and hesitancy towards group discussions (Seitz & Strack, 2016). Moreover, with unmet basic needs, these individuals are living in a perpetual state of crisis, and other issues understandably take priority over the project (Halifax et al., 2008). As a result, such studies often have small sample sizes (i.e., 6-13 people). Although PV projects with individuals who have previously experienced homelessness have increased in recent years (McKinsey et al., 2021; Pruitt et al., 2018), PV studies with individuals actively experiencing homelessness are less common. For example, a 2016 review found only seven academic articles published between 2000 and 2013 describing PV studies with IEH at the time of the study, suggesting the need for more research capturing lived experiences of homelessness in real-time (Seitz & Strack, 2016).
IEH and Impacts of COVID-19
IEH were among the vulnerable populations worldwide that were disproportionately impacted by the COVID-19 pandemic (Corey et al., 2022). Particular impacts unique to IEH include a reduction in available services and amenities, and reduced opportunities for earning income (Population At-Risk: Homelessness and the COVID-19 Crisis, 2020). Although PV has been used virtually among older adults during the COVID-19 pandemic (Ferlatte et al., 2022) and among youth experiencing homelessness (Damian et al., 2022), few studies have used the PV methodology with IEH during the COVID-19 pandemic. As such, this study aimed to better understand the impact of the COVID-19 pandemic on IEH in South Santa Barbara County (SSBC) from their perspective. SSBC is home to more than 1,200 IEH, accounting for more than 63% of Santa Barbara County’s total population experiencing homelessness (Cottage Health Community Health Needs Assessment Report 2019, 2019).
This paper examines: (1) the methodology for recruiting IEH, (2) innovative and emerging applications of PV for capturing lived experiences during a pandemic, (3) strategies for designing partnerships between multi-sectional organizations, (4) the application of infection prevention and control protocols, (5) the use of robust, collaborative data analysis methods, (6) approaches for disseminating and implementing key findings, and (7) lessons learned. Given their involvement at each stage of the research process, IEH are referred to as “co-researchers” in this study rather than “participants.”
Methodology
Co-researcher Recruitment
Ethical approval to conduct the study was obtained through the Santa Barbara Cottage Hospital Institutional Review Board (IRB: 20-106sx). For the research team, six research assistants (RAs) were recruited from local volunteer groups and advocacy organizations to help recruit co-researchers. All RAs had some experience volunteering and facilitating conversations with IEH. In addition, RAs completed Institutional Review Board (IRB), Health Insurance Portability and Accountability Act (HIPAA), and Photovoice (PV) training prior to beginning co-researcher recruitment. Each RA spent between a total of 20-30 hours on the following tasks: (1) recruiting, (2) following up with co-researchers, (3) gathering cameras, and (4) facilitating focus groups. RAs were compensated with a $225 stipend for their time.
RAs recruited 50 IEH from the following sub-populations across SSBC County: (1) sheltered, (2) vehicular homelessness, and (3) unsheltered. Sheltered individuals were those sleeping in temporary or transitional shelter. Unsheltered refers to individuals sleeping outdoors, including in tents and makeshift shelters, and vehicular individuals were those sleeping in vehicles. Vehicular individuals make up more than 32% of IEH in SSBC (2019 AHAR: Part 1 - PIT Estimates of Homelessness in the U.S., 2020). Individuals experiencing vehicular homelessness are traditionally hard-to-reach because they are often difficult to identify and recruit, and they are mobile throughout the daytime when researchers aim to recruit study participants.
Recruitment of Sheltered Co-Researchers
After initial communication about the study objectives and methodology, partners, including shelter staff, outreach workers, and community advocates, supported recruitment efforts by distributing flyers to potential recruits and providing relational warm handoffs to RAs. Co-researchers in the sheltered population were recruited from two local congregate shelters (100 beds each), and two local non-congregate shelters (approximately 34 private beds each). RAs coordinated with shelter staff to invite potential co-researchers to participate in an initial informational meeting onsite at the shelter in outdoor or socially distanced settings.
Recruitment of Vehicular Co-Researchers
To recruit co-researchers from the vehicular population, RAs relied heavily on local Safe Parking Program (SPP) staff. One SPP staff member was also an RA. SPP provides approximately 200 parking spaces in 31 select parking lots for those sleeping in cars to safely spend the night and receive case management services (New Beginnings: Safe Parking, 2024). Since SPP sites are confidential, only SPP staff were able to recruit at these sites. SPP members had established trust with the vehicular population which was vital during the recruiting process. Additional recruitment was completed with other RAs working alongside a SPP staff member to conduct outreach in public parking lots and streets known for being overnight parking sites. In the cases where an RA was accompanied by a SPP staff, SPP staff would knock on the car windows of co-researchers willing to participate or direct RAs to co-researchers that were willing to participate. A County Public Health Nurse provided additional recruiting assistance and accompanied RAs to parking sites occupied by clients.
Recruitment of Unsheltered Co-Researchers
To recruit unsheltered co-researchers, RAs first walked through sites with a high density of unsheltered individuals alongside staff from various homeless outreach programs (i.e., City ambassadors, nonprofit outreach staff, and County Public Health nurses). These staff identified individuals and provided a warm handoff so that RAs could more easily gain trust of potential co-researchers. RAs also recruited from Coordinated Entry System access points (sites designated for formal referrals to shelter and services), community food distributions, and other service locations where IEH were likely to visit.
The study inclusion criteria comprised of individuals who: (1) spoke English or Spanish as their primary language, (2) were at least 18 years of age, (3) were alert and oriented x 4 (i.e., alert and oriented to person, alert and oriented to place, alert and oriented to time, and alert and oriented to situation), (4) self-identified as being homeless at the time of study in SSBC regardless of length of homelessness or previous location of residence (or recently housed in SSBC within the past six months), and (5) were interested in participating in the study. Individuals excluded from the study included those who: (1), were visibly intoxicated and/or not alert and oriented x4 (i.e., alert and oriented to person, alert and oriented to place, alert and oriented to time, and alert and oriented to situation), (2) spoke a primary language other than Spanish or English, or (3) were residing in jails, prison, or substance use treatment facilities at the time of study.
Of the 50 co-researchers recruited, 38 co-researchers engaged in the study. Eight co-researchers dropped out during the study due to various challenges, several of which are common to those experiencing homelessness: transience in the community, health and mental health factors, and dealing with stressors, such as having possessions stolen. Thus, a total of 30 co-researchers completed the project.
Data Collection: Co-Researchers and Research Assistant Meetings
Co-researchers and RAs met three times throughout the study (see Figure 1). The first meeting was an initial one-hour recruitment meeting where RAs reviewed the study purpose and methods, acquired the written informed consent and demographic data from potential co-researchers, and distributed disposable cameras. Disposable cameras were used for the study because they are: easy to use, portable and durable, and inexpensive (Wang & Redwood-Jones, 2001). RAs provided technical instructions for the disposable camera use. RAs also explained the photo prompt: “What do we want those in power to know about us and our everyday struggles with homelessness during the COVID-19 pandemic?” Details of the Three Encounters Between Co-Researchers and Research Assistants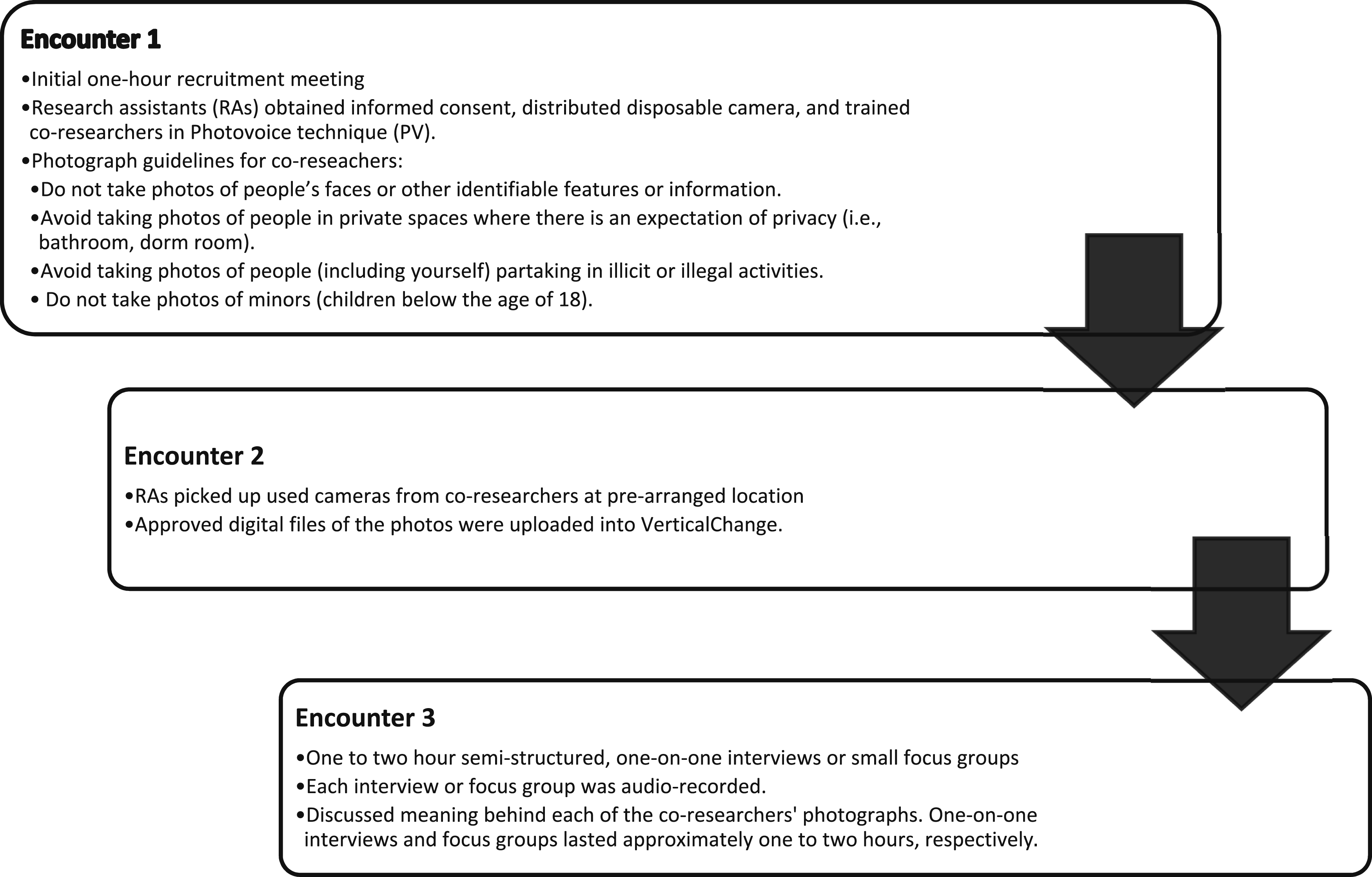
The initial recruitment of sheltered co-researchers was followed by the first PV encounter one week later. Encounters at congregate shelters were scheduled around mealtime to ensure co-researchers were likely to be onsite at the designated time. Shelter staff also checked in with the co-researchers between PV encounters to assess whether additional assistance was needed for participation. For the vehicular and unsheltered co-researchers, the first recruitment meeting also served as the first PV encounter to minimize logistical challenges.
After the first encounter, demographic and consent information were uploaded to VerticalChange, a cloud-based HIPAA-compliant data collection and reporting platform that stored data, notes, audio recordings, and co-researcher photographs (VerticalChange, 2013). Key research personnel were able to access the recordings, photographs, and information for data analysis.
A second meeting occurred seven to ten days after the first encounter where RAs gathered cameras from co-researchers. The research team, which consisted of staff from a local health care system and homeless services provider, used a local film developing service to develop, print, and digitize the film from the disposable cameras. The research team’s mandated reporter (i.e., a registered nurse and/or a social worker) reviewed all photographs prior to uploading the approved digitized files into the Vertical Change database (VerticalChange, 2013). Any photographs that depicted illegal or illicit activities involving children, suspected abuse and/or neglect of dependent individuals or other mandatory reportable events were reported to the appropriate authority (Child Protective Services/Adult Protective Services) by the mandated reporter. Further, any photographs that included identifying information (e.g., faces or tattoos) or other illegal activities (e.g., illegal drug use) were removed, destroyed, and excluded from the study. No photographs were discarded due to poor photo quality. If the quality of a photography was poor, attempts were made by the research team to improve the quality of the photo by using photo editing software.
After another seven to ten days, the third meeting was an audio-recorded, semi-structured one-on-one interview or focus group (consisting of two to six co-researchers). These interviews or focus groups took place from May 24, 2021 to August 12, 2021. During the focus groups, co-researchers had the opportunity to share individual photographs that they had taken. To facilitate the dialogue, the research team utilized the “SHOWED technique” (Kowitt et al., 2015). SHOWED involves asking co-researchers to respond verbally to the selected photographs in response to the following questions: (1) What do you See here? (2) What is really Happening here? (3) How does this relate to Our lives? (4) Why does this situation, concern, or strength Exist? and (5) What can we Do about it? (see Figure 2) (Kowitt et al., 2015). These focus groups lasted approximately 2.5 hours, and each co-researcher received a COVID-19 Prevention Kit and $75 gift card. RAs then uploaded the focus group audio recordings, notes, and forms into VerticalChange (VerticalChange, 2013). SHOWED Mnemonic (Kowitt et al., 2015)
At the end of the focus group, co-researchers indicated which, if any, photographs they wanted to release to the research team for publications and presentations, signing a release form for the selected photographs. All co-researchers received hard copies of their photographs (excluding any photographs that contained content violating study guidelines). Co-researchers also provided input about how they would like the research information shared with the public and were invited to participate in planning meetings for public presentations. For example, some co-researchers suggested offering a PV exhibition at the Public Library, a site where co-researchers often intersect with other members of the public.
Application of COVID-19 Pandemic Safety Protocols
Study recruitment and data collection occurred a little over one year after the start of the COVID-19 pandemic (Frequently Asked Questions about COVID-19). Therefore, infection prevention guidelines in accordance with the Centers for Disease Control and Prevention COVID-19 Prevention Actions were used to design this study (How to Protect Yourself and Others, 2020). RAs received surgical masks, hand sanitizer, and disposable wipes for field activities. RAs were instructed to wear masks and maintain social distancing of at least six feet during all study activities. When possible, focus group conversations were conducted outdoors or in ventilated indoor settings where co-researchers were provided with masks, hand sanitizer, and instructions for infection prevention and control measures. To maintain the goals of PV which are to (1) record and represent co-researchers lived experiences, (2) promote critical dialogue and knowledge about person and community strengths and concerns and (3) reach policy makers (Damian et al., 2022), the research team deemed it more advantageous to implement safety protocols rather than conduct PV virtually or with the use of another medium.
Data Analysis
The data analysis team, which consisted of three PhD trained social scientists and an expert non-profit community leader for IEH, started the data analysis process by reading and rereading the transcripts and generating initial codes to identify noteworthy topics. The 13 interview and focus group audio recordings were transcribed and coded using NVivo (QSR, 2020). A thematic analysis approach was used to analyze data from each transcript (QSR, 2020). Themes were primarily generated inductively.
Each team member was assigned three or four transcripts and manually read through each transcript coding ideas, phrases, and quotations. Before individually coding each transcript, the data analysis team met to develop a coding tree that consisted of key words, phrases, and/or ideas grouped into “codes.” Using this coding tree, team members coded the same transcript to ensure consistency of coding. The data analysis team achieved an inter-rater reliability of 0.8 or higher for each code before beginning individual coding. The team also met weekly to reach consensus on all themes and associated quotations for each theme.
Designing Partnerships
This study was conducted as a partnership between four key partner agencies (Figure 3). The study was initiated and led by Cottage Center for Population Health at Cottage Health (Cottage), a not-for-profit healthcare system in Santa Barbara County, and supported by Cottage Health Research Institute. Santa Barbara Alliance for Community Transformation (SB ACT), a 501(c)3 nonprofit organization, assisted with facilitation of partners and co-researchers and data collection. SB ACT “exists to equip the community to lovingly engage the marginalized while actively working for the betterment of their physical, spiritual, emotional, and mental needs” (SB ACT, 2020). As such, IEH are a key marginalized population that SB ACT works with. VerticalChange, a cloud-based HIPAA-compliant data collection and reporting platform, provided data storage and organization (e.g., digital copies of photographs, consent forms) (VerticalChange, 2013). The partnerships developed and deepened throughout this study were integral to its success and instrumental throughout execution. Importance of Partnerships Between Four Key Partner Agencies, Research Assistants, and Co-Researchers
Cottage and SB ACT coordinated on all aspects of study execution. In planning the study, Cottage developed partnerships with local service providers to ensure co-researchers from all three subpopulations (sheltered, unsheltered, and vehicular) across SSBC would participate. Based on this planning phase, strategic partnerships must be built early in the study planning phase to meet recruitment and study goals.
Because one partnership included a data management platform, the study collected and managed high quality, sensitive data and securely shared it among partner organizations. This project utilized customized software to store multimedia data, which was collected primarily in the field via electronic devices (e.g., digital voice recorder or iPad). Considering differing levels of technical capacity and HIPAA requirements among partners, the software was carefully configured for accessibility and ease of use, while still maintaining industry-standard security and methodologically-sound data organization. VerticalChange provided data quality assurance and progress reports, which informed decisions during recruitment and data collection. Future researchers are encouraged to include a technology partner. The primary technology-related limitation encountered during this study was variable data entry by RAs. Despite the benefits of a central platform, RAs did not always enter data in a timely or complete manner, which created unplanned work for research coordinators. This may have been mitigated by scheduling dedicated data-entry time for RAs immediately following focus groups and interviews.
Service organizations proved essential to recruiting hard-to-reach co-researchers. These groups educated RAs on appropriate ways to approach potential co-researchers and provided connections to the vehicular population experiencing homelessness. Shelter and service provider staff and community advocates provided warm handoffs to RAs to assist with recruitment, increasing trust in RAs.
Additionally, service providers helped ensure a safe and consistent place for data collection. Many offered space at their organization or shelter for discussions, which allowed for a comfortable, familiar and accessible place for co-researchers and RAs to convene. Having a location familiar to co-researchers was beneficial, especially given closures due to COVID-19. The degree of partner cooperation greatly contributed to high co-researcher retention rates across sub-populations.
Trauma Informed Approach
When engaging in research with vulnerable populations, it is important to remain aware that individuals may become distressed or re-traumatized as a result of sharing their experiences or traumatic life events (Bath, 2008). These individuals can benefit from trauma-informed care that is sensitive to their unique needs. Safety, connections, and managing emotions—three treatment elements that constitute a trauma-informed approach—can be applied by researchers when leading focus groups to promote a healing environment; thus, mitigating the potential for individual distress or secondary trauma (Bath, 2008).
Research team members engaged in trauma-informed behaviors throughout study design and execution. Before the data collection phase of this study, service providers educated RAs on appropriate ways to approach potential co-researchers. Warm handoffs between shelters and service organizations and RAs were critical in the research process. These handoffs helped establish connections between co-researchers and RAs, a critical component of trauma-informed care.
During data collection, RAs sometimes adapted the focus groups to accommodate the needs of co-researchers. In one instance, co-researchers indicated that they felt triggered by the conversation. The RAs paused the conversation and gave these co-researchers the option to leave for the day. RAs then re-engaged the co-researchers in one-on-one interviews on a later date. During the data collection phase, some RAs indicated struggling with experiences of secondary trauma from hearing focus group discussions about co-researchers’ trauma. Future research should consider establishing trauma-informed care protocols for both RAs and co-researchers.
Dissemination
During the focus group interviews co-researchers shared that they would like for the study results to be shared with the public using a variety of dissemination methods such as public presentations (via Zoom or in-person) and a PV photo exhibition. The research team felt strongly about honoring the co-researchers request and broadly shared the results of the study, which were a representation of the co-researcher’s voices, with community leaders, service providers, and the public to provide knowledge specific to homelessness communities in crisis response efforts.
Co-researchers were invited to participate in two planning meetings before the dissemination efforts commenced. Zoom and in-person planning meetings were provided to co-researchers in which the research team shared preliminary study results and asked co-researchers for their input regarding the study results and ideas for dissemination. Based on co-researcher input, the research team presented the study results at: (1) Cottage Population Health and Equity Board Committee Meeting, (2) Cottage Health Research Institute Research Symposium, (3) National Health Care for the Homeless Council (NHCHC) Conference, (4) Santa Barbara (SB) Continuum of Care Elected Leaders Forum, (5) Coordinated Entry System Case Conference, (6) Christ Presbyterian Church---photo exhibition, and (8) SB Public Library--- photo exhibition (see Figure 4). Homelessness Research Project Photo Exhibition at Santa Barbara Public Library
SB Public Library Photo Exhibition
The SB Public Library Photo Exhibition had two components: (1) a large central display case in which 28 co-researcher photographs were displayed inside a glass case along with information about the study and study themes (Figure 5), and (2) a one-time event displaying 28 co-researcher photos and corresponding themes on eleven 6.5 feet tall x 2 feet wide free-standing panels that included study information and themes (Figure 4). A QR code linking to a report detailing the study and a flipbook book titled “Through The Lens: Experiencing Homelessness During COVID-19” was available for attendees to access for additional study information (Experiencing Homelessness During COVID-19: A Collaborative Research Study). The photo exhibition was curated by a collaboration between the research team (i.e., Cottage Center for Population Health and SB ACT), Cottage Marketing, and a professional design team. The execution of the photo exhibition involved meticulous planning and careful consideration of logistical details, which ensured that every aspect from layout design to visitor flow was seamlessly coordinated for an impactful experience. Public dissemination of co-researchers’ photographs and narratives can challenge stereotypes and reduce stigma around homelessness. Photo exhibitions offer a way to blend perspectives with compelling storytelling and should be considered by future research. Homelessness Research Project Glass Case Display at Santa Barbara Public Library
Study Learnings, Challenges, and Opportunities
Recruitment and Retention
Working with various populations experiencing homelessness presented challenges as well as opportunities. Sheltered co-researchers were generally the easiest to locate and most consistent in returning for subsequent PV encounters. Similarly, vehicular co-researchers who were SPP clients were easy to locate and access with SPP staff helping to ensure consistent participation.
The COVID-19 pandemic also afforded the research team some unexpected opportunities regarding recruitment and retention, which may have contributed to the high retention rate (38/50; 70% retention rate). A South Santa Barbara County pandemic driven intervention authorized the creation of non-congregate shelters in which IEH at high risk for developing severe COVID were housed in hotel rooms. This intervention provided a centralized location to recruit IEH for the study. Moreover, co-researchers in the non-congregate shelter setting communicated a high level of enthusiasm about their participation because they had felt socially isolated by the nature of their shelter setting, had more idle time, and had limited outlets to connect with their own community, as well as the community at-large. This study provided an opportunity to form relationships within an isolated sub-community that was especially vulnerable to the effects of COVID-19.
Unsheltered individuals, not part of the SPP, were the most difficult to recruit and coordinate follow-up encounters, often due to the varying challenges of day-to-day life without consistent shelter. In some instances, RAs returned for the second encounter and were informed that the co-researcher’s camera had been stolen or lost. In other instances, co-researchers either did not have consistent access or any access to a phone. This inconsistent access to technology created scheduling logistical challenges. For example, RAs had to return three times to the same co-researcher to retrieve the camera. When possible, during the initial meeting, RAs tried to schedule all three encounters for the same time and location one week apart to avoid confusion.
Conducting focus groups with vehicular and unsheltered populations also presented unique challenges, as these individuals were limited to outdoor, largely public settings due to COVID-19 social distancing protocols. RAs had to identify private discussion sites at the far ends of public parks and frequently had to ask non-participating individuals to leave the conversation. Although these pandemic-related issues are not unique to this population, we recommend that future researchers involve community member RAs to identify and secure outdoor meeting sites.
The partnership with SPP played a crucial role in overcoming many of these recruitment and retention challenges, particularly for the vehicular sub-population. SPP staff not only facilitated access to participants, but also helped maintain engagement by providing reminders and logistical support such as securing safe meeting locations and assisting with scheduling follow-ups. Their involvement mitigated some of the barriers related to inconsistent access to technology and transportation, ensuring that co-researchers could return for subsequent encounters. This collaboration highlights the importance of integrating service providers into research efforts to enhance participation and reduce attrition in hard-to-reach populations.
Research Assistants
The key challenge with community members such as RAs was in training and preparation. Partnering with RAs for recruitment of co-researchers required clear expectations to ensure regulatory compliance to maintain fidelity to study methodology execution. RAs must also be flexible when working with populations experiencing homelessness and multiple entities.
Community members acting as RAs were also one of the most unique and successful partnerships developed and leveraged in this project, particularly to achieve recruitment of a large and diverse group of co-researchers. RAs were able to spread out across the region and epitomized a core aspect of CBPR in that they allowed for a disruption of power dynamics between researcher and subject (Grieb et al., 2017). They offered objectivity as a third party separate from co-researchers participating in the study, researchers developing the study, or service providers who may be biased and limited on time due to work requirements. As a result, partnering with community members as RAs for recruitment and data collection may have allowed for increased trust from co-researchers and higher quality data due to decreased social desirability bias, as co-researchers may have felt able to share their experiences more freely without seeking to please the researcher. Instead, in conversations with community member RAs, there was no expert, and co-learning could occur. For these reasons, future PV researchers should enlist RAs who are community members with experience working with IEH.
Multi-Sector Partnerships
The partnerships between the three agencies (Cottage, SB ACT, VerticalChange) and , and service providers were instrumental throughout the study execution and ultimately contributed to the success of the study. These collaborations not only facilitated study implementation, but also provided critical infrastructure for data, participant trust-building, and infection prevention measures. Cottage proactively developed relationships with local service providers to ensure representation from all three subpopulations (sheltered, unsheltered, and vehicular) across South Santa Barbara County. This strategic approach underscored the importance of establishing partnerships in advance of the study launch to help reach populations that would otherwise be difficult to engage.
Having VerticalChange as a technology partner helped facilitate confidential data collection, management, and communication among partner organizations. This partnership provided real-time quality assurance and allowed researchers to identify gaps in data collection early to adjust strategies as needed. The collaboration with a dedicated technology partner helped achieve high research integrity data management.
Engaging with community-based service organizations proved invaluable for recruiting and retaining hard-to-reach populations, particularly for vehicular co-researchers and those living in non-congregate settings. Service providers offered direct connections to co-researchers, and educated RAs on the most effective and respectful ways to approach potential co-researchers. By building on the existing trust between service providers and IEH, the research team was able to establish credibility and increase participation rates.
The integration of healthcare, community organizations, technology providers, and service networks created a collaborative framework that improved data integrity, co-researcher engagement, and overall study success. Future research initiatives should prioritize early and intentional partnerships, particularly with data management platforms, service providers, and healthcare organizations, to ensure robust data collection, enhanced participation, and sustained engagement across diverse populations.
Limitations
Despite the strengths of using PV as a Community-Based Participatory Research methodology, several limitations should be acknowledged. PV provided a participatory and empowering approach for co-researchers; however, it required co-researchers to have some level of engagement and technical ability to use disposable cameras. This may have limited participation from individuals with cognitive impairments or those unfamiliar with photography. Additionally, participation required a willingness to engage in multiple study meetings, which may have excluded individuals with severe mental health conditions, substance use disorders, or those experiencing transient movement outside the county. The study was conducted in South Santa Barbara County, an area with unique social, economic, and policy factors influencing homelessness. The methodologies employed by this study may not be generalizable to other areas with different housing policies, climates, or service infrastructures. Community-Based Participatory Research methodology is inherently contextual and tailored to address the specific needs and priorities of the communities involved through an equitable and collaborative process to maximize diverse contributions (Collins et al., 2018). Future studies should consider the use of the PV methodology in other communities to further enhance the depth of findings.
Conclusion
This paper examines: (1) the methodology for recruiting IEH, (2) innovative and emerging applications of PV for capturing lived experiences during a pandemic, (3) strategies for designing partnerships between multi-sector organizations, (4) the application of infection prevention and control protocols, (5) the use of robust, collaborative data analysis methods, (6) approaches for disseminating and implementing key findings, and (7) lessons learned. Co-researchers from sheltered, unsheltered, and vehicular populations experiencing homelessness shared their perspectives through photographs.
The unprecedented effects of the COVID-19 pandemic added a level of complexity to conducting this PV project. However, partnerships between the healthcare organization, community organization focused on addressing local homelessness, shelter and service agency staff, community members interested in assisting with the study, and software development company were integral to the success of the project. The methodology described in this study can inform future efforts to conduct PV among IEH and offer insights on how to strategically involve partners and IEH at various levels (service providers, community members, co-researchers).
Footnotes
Acknowledgements
The authors would like to thank all the co-researchers who generously contributed their time and perspectives to this research. The authors would also like to thank the following auxiliary staff and organizations that were instrumental to this work: all Research Assistants, service agencies, shelters, and the Safe Parking Program.
Ethical Approval
This study involves human participants and was approved by the Santa Barbara Cottage Hospital Institutional Review Board (20-106sx). An informed consent document was signed by all co-researchers before taking part in the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funding from the Cottage Center for Population Health and Cottage Health Research Institute.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.