
Abstract
There are few support services specifically for individuals living with young onset dementia (YOD) (age <65 years at diagnosis). To gain a better understanding of what individuals living with YOD desire in a day program, this project aimed to guide a collaborative re-development and evaluation of two new day programs in Southern Ontario. Using action research techniques and consultative processes, we worked with key stakeholder groups, alongside flexible and innovative methods, to engage individuals living with YOD, care partners, and staff. This project brings forward findings regarding processes to engage persons with YOD in research, beyond a biomedical framework (e.g., factors predicting institutionalization, the course and impact of neuropsychiatric symptoms), or focusing solely on information provided by family, care partners, or healthcare professionals. This article details two aims: 1) to document the research processes and approaches used to engage a range of participant groups, particularly younger persons with dementia, and describe the lessons learned, and 2) to provide reflections on the potential of Goal Attainment Scaling as an evaluation measure in the context of YOD programs.
Introduction
Persons with dementia have often been excluded or minimally engaged in research processes, due to misconceptions of being “unagentic” and “lacking cognizance”, driven by dominant biomedical discourses (Bell & Leong, 2019; Dupuis et al., 2012; Mitchell et al., 2013, 2020). Including persons living with dementia as active research partners is important for challenging dominant ideologies about dementia, better understanding their lived experiences, and for providing a communicative space for their voices to be illuminated when they are often overlooked. The question remains as to how researchers can adapt and find creative ways to support persons with dementia in expressing themselves in a way that is comfortable and extends beyond verbal communication.
This project set out to guide the collaborative re-development and evaluation of two new day programs in Southern Ontario for individuals living with young onset dementia (YOD), using action research techniques and consultative processes. The purposes of this article are: 1) to document the research processes and approaches used to engage a range of participant groups, particularly younger persons with dementia, and describe the lessons learned, and 2) provide reflections on the potential of Goal Attainment Scaling (GAS) as an evaluation measure in the context of YOD programs.
Living With Young Onset Dementia
Persons with YOD are diagnosed under the age of 65 (The World Health Organization [WHO], 2012). This means that these individuals can be in their 40s, 50s or even younger; they will likely be employed, socially active, and physically fit (Jefferies & Agrawal, 2009; Kilty et al., 2019). There are approximately 16,000 Canadians who have been diagnosed with YOD (Alzheimer Society of Canada [ASC], 2016), but few day programs are available to support the unique needs of persons living with YOD and their families (Alzheimer’s Association, 2006; ASC 2016; Carter et al., 2018). This underrepresentation of YOD services largely stems from the belief that dementia is a disease impacting only the oldest sections of the population, as well as a focus of program development for a larger group of older people living with dementia. As a result, the current provision of dementia care and services is primarily focused on and reflective of the needs of older adults (Giebel et al., 2020). A recent international Delphi study found a strong consensus that persons with YOD require age-appropriate programs and services (Couzner et al., 2022). Unfortunately, recent systematic reviews identified a paucity of research how to provide or design services for persons living with YOD (Richardson et al., 2016; Mayrhofer and colleagues, 2018). Mayrhofer and colleagues (2018) concluded from their review that “the inclusion of people with YOD and their caregivers in service design is critical when planning support in order to delay institutional care” (Mayrhofer et al., 2018, p. 933).
Individual differences in age, physical ability, and diagnoses often result in practical and emotional needs that are unique for persons with YOD and their families, yet these differences are often overlooked within healthcare and society. YOD has a much more heterogenous etiology (Couzner et al., 2022; Jefferies & Agrawal, 2009) with a more prominent genetic component than what is commonly seen in late onset dementia (LOD) (Rogers & Lippa, 2012). Alzheimer’s Disease (AD) is 50% less prevalent in individuals under the age of 65, yet other rarer forms of dementia are 20% more prevalent (Jefferies & Agrawal, 2009). This is an important distinction, as the type of dementia diagnosed has implications for prognosis and symptom recognition, and for treatment and support options (van Vliet, 2012). Current service provision for persons with dementia are largely age specific and focus on supporting older persons living with dementia; some services go as far as excluding individuals who are under the age of 65 (Couzner et al., 2022; Shnall, 2009).
The development of more appropriate support services for persons with YOD is not only important to the health and well-being of the individual, but also their care partner. Care partners of individuals with YOD are most likely wives, husbands, daughters, sons, or friends (Zarit et al., 2011) and are also often younger in age. These care partners may have ongoing obligations such as employment or parenting (van Vliet et al., 2010). Without the necessary support systems in place, they may be left unsupported and unsure of how to balance the pressures between their daily and care partner responsibilities. The ramifications of this can be extremely harmful and include social isolation and caregiver burden (Chirico et al., 2021; Shnall, 2009).
Study Context: Participatory Development of YOD Day Programs
A collaborative effort between an advisory committee and two not-for-profit facilities in Southern Ontario aimed to develop two specialized day programs, 1 recognizing there were none available in the region (blinded, 2014), and few YOD programs known to exist in Canada (ASC, 2016). Without appropriate services, care partners either need to leave the person they care for at home in isolation (Roach & Drummond, 2014), or utilize a service that is inadequate for the needs and interests of younger persons with dementia. These factors contribute to feelings of marginalization within the context of support services, and in the social lives of persons with YOD (Beattie et al., 2002; van Vliet, 2012).
The two facilities developed the YOD day-programs to address the need for more support services for individuals with YOD, however, did not involve persons with YOD or care partners in the development process. In recognition of this, about one year after the programs had been operational, leadership from the facilities reached out to our research team, from which a participatory evaluation 2 of the programs was proposed. The goal of the evaluation was to understand the facilitators and barriers of day program utilization, as well as recommendations for program improvement, from the perspectives of persons with YOD and their care partners, as well as of program staff. The evaluation also aimed to develop a better understanding of the needs of persons with YOD and their care partners, so that the programs could be strengthened to better support these dyads. Part of this process included the exploratory use of an individualized outcome measure – Goal Attainment Scaling - as an approach to help identify how the programs are impacting members, while respecting the individuality of each person. A separate manuscript detailing the evaluation results, including specific recommendations for program improvement, is currently in preparation and will be presented in a subsequent article. This article will focus on the methodological lessons learned through the actual process of conducting a participatory evaluation with persons living with YOD, care partners, and staff members, including the exploratory use of GAS.
Site Description
Eligibility Criteria for Young and Late Onset Day Programs.

Program Description
Two specialized YOD day programs were evaluated in this study, each serving a small cohort of individuals living with YOD. At Site 1, the program operated with nine program members, nine care partners, and seven staff members. At Site 2, there were five program members, three care partners, and five staff members. Program participants were diagnosed with YOD, with an age range of 53 to 73 years, and a mix of dementia types, including Alzheimer’s disease, frontotemporal dementia, and vascular dementia. While most program members met the age criterion of a YOD diagnosis before 65, one participant had been diagnosed after 65 but met all other eligibility requirements.
The program provided structured, weekly sessions designed to foster social engagement, skill-building, and personal enrichment. Activities included physical exercise, arts-based activities, cognitive stimulation, and community outings. The programs aimed to address the unique needs of individuals with YOD by offering age-appropriate, socially engaging experiences that supported both cognitive and emotional well-being.
Each site was staffed by a multidisciplinary team, including a program administrator, a family support coordinator, a program leader, and a program assistant. The management and administrative team oversaw the day program along with other support services offered at the site, and also worked to identify gaps in service and connect individuals and care partners to other support services in the community. The family support coordinator conducted intake assessments, provided ongoing support to members and care partners, and facilitated transitions beyond the program. The program leader was responsible for daily programming and ensuring alignment with regional service mandates, while the program assistant supported the delivery of activities and facilitated on-site and community-based programming.
Staff qualifications varied based on role but typically included formal training in health, social services, or recreation therapy, with additional supervisory training provided as needed. The study’s methodology was shaped by the program’s emphasis on small-group engagement, interdisciplinary staff involvement, and participant-driven activities.
Methods
Few qualitative research projects have directly engaged younger persons with dementia (Greenwood & Smith, 2016), and so literature on appropriate research methods was limited. As such, the methods section outlines the methods selected, and the subsequent results section will outline lessons learned and modifications made.
Study Design and Approach
This research used a process evaluation framework and plan, using an action research approach with consultative processes, to evaluate two newly developed programs for individuals with YOD. With the pilot programs still being in their early stages, a process evaluation was chosen as it focuses on the programs’ operations, implementation, and service delivery.
The iterative and adaptive nature of action research allowed for ongoing reflection and adjustment of both the research processes and program logistics based on participant needs and emerging findings (Dick, 2000). This flexibility was critical given the limited existing literature on qualitative methods involving persons with YOD (Bell & Leong, 2019) and the recognition that adjustments might be needed to accommodate participant preferences and communication abilities.
This study was guided by a pragmatic philosophical worldview, which emphasizes the use of flexible and practical methods to address research questions (Feilzer, 2010). Pragmatism and action research share a focus on action and change, aiming to develop knowledge that can lead to improvement (Goldkuhl, 2011). This perspective aligned with the dual goals of the research: to understand participants’ experiences (“what is”) and explore ways to strengthen the programs (“what might be”) (Goldkuhl, 2011).
Consultative processes were integral to the study, fostering ongoing communication between the primary investigator, program staff, care partners, and program members. Informal meetings, emails, and phone calls supported the iterative adjustment of research methods and program elements. The active involvement of program staff, who had established strong relationships with participants, ensured that adaptations to methods and logistics were appropriate and aligned with participants’ needs.
Participant Recruitment
Participants were purposively sampled from two YOD day program sites in Southern Ontario, representing three key informant groups: program members, their care partners, and program staff. Recruitment materials, including information letters and consent forms, were distributed by program staff, and information sessions were held to explain the study and encourage participation. This study obtained ethics clearance from the University of Waterloo’s Office of Research Ethics (ORE #20761). Informed consent was obtained from all participants. For program members who were unable to provide their own consent, care partners were asked to provide consent on their behalf and program members were asked to provide assent. Capacity to provide consent was determined through the primary investigator’s initial contact with program members at the information sessions, in conjunction with input from care partners and program staff.
Data Collection Overview.

Sequence = recruitment → interview (including GAS baseline) → focus group → GAS follow-up → debrief. Bold text indicates total unique participants for each site and across sites.
Data Collection
Data collection was conducted at two YOD day program sites, engaging program members, their care partners, and program staff. A combination of semi-structured individual and focus group interviews was used to gain an in-depth understanding of participant experiences and program dynamics. The diversity of diagnoses among program members, reflected in differences in communication styles, memory, and stages of their dementia journey, guided the design of these methods. Individual (or dyad) interviews captured personal experiences, while focus groups explored shared dynamics, fostering solidarity and camaraderie among participants through their collective experiences. Additionally, GAS, an individualized outcome measure, was piloted to assess how well the programs supported members in achieving their personal goals (Stolee, 2010).
Qualitative Methods
Semi-structured interviews were used as the primary method of data collection for program members, as they offered flexibility to explore their experiences while addressing their unique communication needs. Given that some program members’ primary form of communication was not verbal, alternative formats were offered, such as dyad interviews involving care partners or program staff to facilitate comfort and engagement (Hellstrom et al., 2007). Focus group interviews were also conducted with program members who preferred group discussions, supported by the use of written and visual aids to accommodate diverse communication abilities (Alzheimer Society, 2015; Cantley et al., 2005). These adaptations were informed by input from program staff, who were familiar with the abilities and preferences of the participants.
Care partners participated primarily in semi-structured individual interviews to explore their perspectives on the programs, the caregiving role, and the impact of the programs on themselves and the program members. At one of the sites, care partners participated in a focus group during a results debrief session, which provided additional insights through group interaction. These interviews aimed to capture care partners’ experiences and any recommendations for program improvement.
Semi-structured interviews were conducted with individual program staff across various roles (e.g., management, family support coordinators, program leaders, and program assistants) to understand their perspectives on program implementation and delivery. Focus groups were also used to encourage collaborative discussion among staff about the program’s successes, challenges, and areas for improvement. These methods provided insight into how staff engaged with program members and care partners, as well as how they adapted to meet participants’ needs.
Quantitative Methods
GAS was piloted in this evaluation to explore how the YOD day programs impacted participants while respecting the individuality of each person. GAS is an individualized outcome measure that has been successfully applied in geriatric care and mental health, including use with persons with dementia (Bouwens et al., 2008; Hartman et al., 1997; Jennings et al., 2018; Rockwood et al., 1997, 2002; Stolee et al., 1992). This tool allows for the customization of both the goals and the scaling of outcomes, measured on a five-point scale ranging from −2 (much less than expected) to +2 (much more than expected), with 0 representing the expected level of attainment (Stolee, 2010).
While GAS has been validated for use with persons with dementia, this study is among the first to evaluate its potential application in the context of YOD day programs. Initial consultations indicated that goal setting was of particular interest to some program members, and it was anticipated that GAS could provide insights into how program elements supported - or hindered - participants in achieving their goals.
Baseline data for GAS were collected during individual interviews with program members, where participants were asked questions such as, “What are some things you are hoping to get out of the program?”, “Do you have any specific goals?”, and “Are there any issues or concerns you would like the program to help you address?” (Stolee, 2010). These discussions aimed to identify approximately three goals per participant, though the process accommodated variation in the number of goals identified.
At six months, follow-up conversations were conducted to assess the level of goal attainment. When necessary, program staff or care partners were consulted to provide additional input to ensure accurate determination of goal achievement. The GAS process offered a structured yet flexible means of evaluating individualized outcomes, contributing to a deeper understanding of the program’s impact on participants.
Given the diversity of data sources, careful attention was given to ensuring consistency and capturing unique insight across methods. While traditional methodological approaches emphasize distinct analyses for data collected through different methods, this study prioritized inclusivity and participant-centered engagement, recognizing the varied communication abilities of individuals living with dementia. Integrating data from individual interviews, dyad interviews, and focus groups allowed for a balance between methodological rigor and accessibility. Analysis maintained attentiveness to differences in how data were generated, ensuring that themes emerging across methods were examined for consistency while also capturing unique contributions from each approach, ultimately strengthening the trustworthiness of the data.
Data Collection Overview
To illustrate participant engagement across data collection methods, Table 2 outlines the number of individuals who participated in each component of the study. This includes participation in individual and dyad interviews, focus groups, the exploratory use of GAS, and results debrief sessions. The table captures variations in participation across different methods and highlights the level of engagement across program members, care partners, and staff.
Lessons Learned: Reflections and Adjustments Made to Data Collection Methods
Reflections on Engaging Younger Persons With Dementia in Research
Individual and Dyad Interviews
Program members had the option to either participate in an individual interview or, in instances in which it was collectively determined that support from a care partner or program leader would be beneficial, a dyad interview. For program members, questions in the individual interview guide included questions regarding their overall healthcare system experience thus far, goals they would like to achieve in the program, their experiences in the YOD programs compared to other programs, and recommendations for program improvement. In instances in which a care partner was present, the additional portion of the interview guide included the aforementioned questions around care partner experiences.
Providing this option increased participation amongst the individuals who had difficulties with verbal communication or memory, as well as those who were hesitant or unsure about the research process. For example, one of the program participants who had Primary Progressive Aphasia - a type of frontotemporal dementia impacting verbal communication - requested support from one of the program leaders who was familiar with supporting this individual’s communication using body language and a picture/words binder. The interactive focus groups, which will be discussed below, are another example of this.
While dyad interviews have their benefits, they can also be challenging. Including a care partner in the interview may be overpowering at times and can reduce the autonomy of the person with dementia (Hellstrom et al., 2007). To help address this concern, the primary investigator shifted eye contact and redirected the question to the program member, to ensure their perception was heard. From the information session, care partners seemed to have an understanding that their role in they dyad interviews was one that was mainly supportive and so issues regarding the overpowering of care partners remained minimal throughout this project. Also, the interactive focus groups provided another opportunity for the participants to express themselves beyond the support of their dyad partner.
Another concern was that the results may be skewed for interviews where the program member decided to have a program staff member present. The concern was that program members may not feel comfortable discussing how the programs could be improved or suggesting recommendations. That being said, the program staff appeared to have a strong rapport with the participants, which gave the primary investigator confidence that the program members provided accurate responses despite the presence of program staff during the interview. For example, members openly discussed suggestions and recommendations for program improvement despite the presence of program staff.
Reflecting on Focus Group Interviews for Younger Persons With Dementia
The first attempt at conducting a traditional semi-structured focus group interview with program members was done at Site 1. Focus groups are particularly useful for individuals in the earlier stages of dementia, especially when using groups of two to four participants (Bamford & Bruce, 2000; Savitch et al., 2006; van Vliet et al., 2017). Group discussions provide feelings of mutual support and opportunities for shared experiences to trigger memory, and also reduce immediate pressure to respond (Bamford & Bruce, 2000). Although it was hoped that providing a discussion-based focus group would unveil rich and complementary data to that uncovered in individual interviews, this format favoured those with strong verbal communication skills while limiting the input of those that preferred alternate means of communication.
For this initial focus group, a list of guiding questions spaced out in size 16 font was handed out to each member along with a pen. Participants were encouraged to write down any comments they did not get a chance to make or had been too uncomfortable saying during the group interview. This was particularly important given that the program leaders were also in attendance to help facilitate discussion. While this is important to consider in future projects, limited data were collected this way.
There were a number of lessons learned from attempting the focus group in this traditional and formal manner, with the ultimate repercussion being exclusion. First, holding the focus group beyond the hours of the program meant that some program members were unable to participate due to issues with transportation. Also, because many care partners of individuals with YOD are still employed, it was not feasible for some families to attend extracurriculars beyond program hours due to lifestyle challenges.
Second, the traditional format of the focus group interview prioritized program members who had strong verbal communication. Amongst the members who were in attendance, there was a clear difference in the level of participation, with more extroverted members at times monopolizing the conversation. Directing questions to the quieter individuals was helpful, but did not completely balance out differences in participation.
Lastly, the formality of the focus group created an atmosphere that some participants may have found off-putting. The focus group was conducted in an empty room that had nothing in it except for the round table and chairs that were used, and although some valuable discussions were had, the overall feeling of the meeting was fairly serious. Reflecting on the limitations experienced in the traditional focus group interview, and with the day program generally engaging members through its fun and lighthearted nature, it was decided that removing the pressure of a formal atmosphere by creating an interactive workshop style focus group might yield increased participation.
For all of the reasons explained, the primary investigator worked with program leaders to ensure any future focus groups incorporated three key changes: 1) the focus groups were to occur during program hours, 2) interactive activities that support a range of communicative abilities were to be incorporated and 3) there would be a combination of smaller and larger group discussions.
Recommendation: Adjusting the Methods in a Focus Group Setting
To make the focus group more engaging and supportive of differing communicative abilities, methods were adapted by drawing on information from the Alzheimer Society of Canada and other sources (Alzheimer Society Canada, 2016, Aphasia Institute, 2015; Cantley et al., 2005; Rehling et al., 2014). These resources provided practical guidance on inclusive communication strategies, such as minimizing distractions, using short and simple sentences, incorporating visual aids, and creating opportunities for non-verbal expression. While the specific activities were designed by the researcher, they were inspired by commonly used facilitation techniques and grounded in best practices to support individuals living with dementia or aphasia in feeling comfortable and able to meaningfully contribute to the discussion in ways beyond verbal communication. Therefore, the alternative focus group incorporated verbal, visual, and written stimuli, and interactive activities.
Interactive Focus Group Activity Guide.
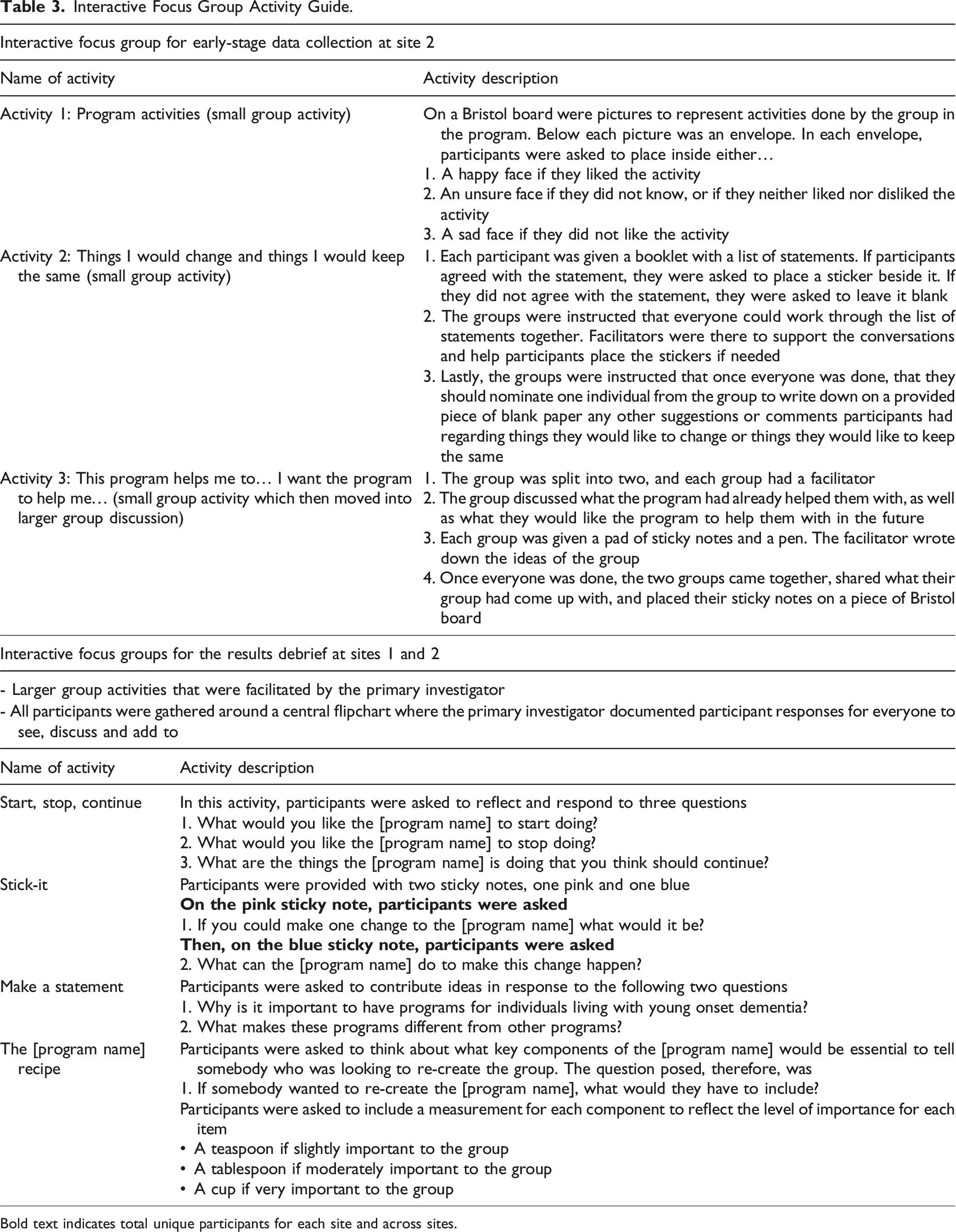
Bold text indicates total unique participants for each site and across sites.
First, it was observed that members seemed to feel more comfortable communicating in smaller groups, which also allowed the staff to make sure they directly involved all members. Second, the interactive activities provided less vocal members with an alternative to the discussion-based format, so that if there was a certain topic they did not want to discuss verbally or had difficulty communicating, the response could often still be collected through their participation in the activities. The group interaction clearly had a positive impact for all program members, which was displayed in the level of engagement observed, and through the improved understanding of participant perspectives regarding the program. Program staff played an essential role in facilitating these discussions while ensuring that participants remained the primary voices in the research. Their familiarity with members allowed for subtle, non-directive facilitation techniques, such as rephrasing questions, using prompts, or encouraging quieter participants to contribute. This support helped balance engagement across communication styles, while still maintaining the autonomy and agency of participants in shaping the discussion.
Reflections on the Use of GAS in Adult Day Programs for Individuals With YOD
GAS was completed for five members across both programs. Due to a change in program location and attrition at the six-month follow-up, GAS was only completed for two members from Site 1. At Site 2, three out of the five members participated, with the remaining two individuals choosing not to participate in follow-up discussions. Both individuals were members of the group who struggled with verbal communication, and so strictly using a discussion-based format for identifying goals and level of attainment should be seen as a limitation when working with younger persons with dementia, and alternatives to this format should be explored (e.g., use of pictures and images).
Program members each identified 2–4 goals they would like the program to help them with, such as: being out in the community (post-diagnosis), learn/use strategies to help cope with symptoms of the diagnosis (e.g., memory), learn/try different types of exercise, socialize, and learn/try something new. When creating the GAS scales for each of the goals, specific words from their interview were used to the extent possible to name the goal. These goals reflected a number of themes, including but not limited to the importance of appropriate programming, group size, and engaging members in selecting activities and outings.
GAS was helpful in identifying the types of goals that participants have in this context. The five program members who completed this part of the project typically reached or surpassed their expected level of goal attainment. GAS shows promise as an individualized outcome measure in social programs for younger persons with dementia. There were also lessons learned about how the measurement could be more effective in this setting. First, alternatives to a discussion-based format should be explored for those who struggle with verbal communication. Second, and in support of this first point, the relationships members have developed with the program staff could be helpful in supporting all members who wish to participate in goal setting. The relationships that had developed between program members and staff were apparent in the level of comfort and understanding that was demonstrated in the data collection processes. It is therefore anticipated that program staff may be better able to support all members in developing and reaching their goals.
An unanticipated finding about the data collection for GAS pertained to the ability of the interactive focus group to provide support in the goal setting process. While many goals were identified by using individual and dyad interviews, the interactive focus group provided unique contributions. The group setting helped the development of ideas for some of the members who did not originally have an in-depth response about their personal goals. As noted by Bamford and Bruce (2000), focus group discussions can provide feelings of mutual support, and an opportunity for shared experiences to trigger memory, as well as reduce immediate pressure to respond.
Peer support played a crucial role in helping individuals clarify and expand their goals, suggesting that interactive focus groups may enhance both goal identification and attainment. The group setting fostered reflection, idea generation, and mutual encouragement, strengthening engagement in the process. The small focus groups also allowed for tracking individual contributions, aiding the development of GAS scales. This highlights the potential of group settings in refining GAS as an outcome measurement tool, particularly in dementia programs, where structured discussions can support both personal and program-level goal setting. Further investigation into this approach is warranted.
Reflections on Engaging Care Partners in Research
Care partners had the option of participating in an individual interview, or in dyad interviews if it was felt that it would help support the person with dementia in the interview process. Most of the care partners (n = 8) participated in a dyad interview together with the person they care for; three had individual interviews. While helpful, it is likely that the interviews were too few to capture a comprehensive picture of care partner experiences of the program and broader healthcare system.
Initially, a focus group for care partners was not planned. However, during the results debrief session at Site 2, a separate group discussion for care partners was organized to accommodate the high number of participants who agreed to attend. This session allowed the primary investigator to present findings, seek feedback, and ensure the results reflected the care partners’ experiences. While the care partners largely supported the findings, the session also sparked rich discussions that extended beyond program-specific feedback to include broader challenges and suggestions related to caregiving for individuals with YOD. Notably, many care partners shared feelings of isolation and the value of connecting with others who shared similar experiences. The group setting fostered a dynamic exchange of resources, stories, and support that was not captured in individual interviews. A debrief session was also held at Site 1, but no care partners attended, resulting in participation from only program members and staff.
Reflecting on this process, a structured focus group earlier in the data collection phase could have captured a broader range of care partner perspectives and provided opportunities for peer connection. The focus group format also had the potential to enhance engagement, expand on individual responses through group interaction, and address resource constraints that limited the feasibility of conducting individual interviews for all care partners.
Reflections on Engaging Program Staff in Research
All staff who were involved in the development of the YOD day programs were recruited to participate in the study, and invited to participate in semi-structured individual and focus group interviews. Originally, one generic interview guide was developed for all program staff, however interview guides were adjusted to include role-specific questions.
Interview guides generated an abundance of information on the program’s development, operations, and future development. A focus group interview was used in conjunction with the individual interviews, to elicit responses informed by group interaction and the comingling of individual participant experiences and beliefs (Stewart et al., 2008). While helpful in shedding light on the strengths and limitations of communication amongst staff, most of the information derived from the focus group was repetitive of the data derived from individual interviews. With the individual interviews providing a safe space where staff could speak freely about the strengths and challenges of the program in the absence of other program staff or management, a focus group with program staff may have been more useful later on in the evaluation process; this could have created an opportunity for staff to come together to set goals and make a plan for the program moving forward, as well as for exploring ways to incorporate any remaining feedback.
The triangulation of data from program members, care partners, and staff provided a multi-dimensional understanding of program effectiveness and individual experiences. By integrating multiple perspectives, the evaluation was able to capture a more holistic view of the programs’ impact, including aspects that may not have been apparent if only a single group had been consulted. This methodological approach enhanced the credibility and richness of the findings by ensuring that program evaluation and improvement recommendations were informed by diverse stakeholder experiences.
Conclusions and Implications
This article had two primary aims: (1) to document the research processes and approaches used to engage a range of participant groups, particularly younger persons with dementia (YOD), and describe the lessons learned, and (2) to provide reflections on the potential of GAS as an evaluation measure in the context of YOD programs. The findings contribute valuable insights for both research and practice, emphasizing the importance of flexible, inclusive methods and collaborative approaches.
Working with younger persons with dementia was an eye-opening experience that underscored the need for adaptable and engaging research processes. The high levels of physical ability, unique life stage experiences, varying symptom profiles, and diverse communication abilities of the group demanded innovative methods. The use of dyad interviews and interactive focus groups ensured that individuals with varying needs and abilities could meaningfully contribute to the research. The camaraderie and support observed among participants were powerful, creating a sense of collective engagement in program improvement.
The study also challenges dominant stereotypes of persons with dementia as “unagentic” or “lacking cognizance” (Bell & Leong, 2019; Dupuis et al., 2016; Phillipson & Hammond, 2018). By using inclusive and flexible methods, this research demonstrated how persons with dementia can actively participate and provide meaningful contributions, emphasizing the importance of innovative approaches to support their communication and engagement.
For care partners, who initially participated to support program members, it became apparent that their unique perspectives warranted separate exploration. Future studies should consider introducing dedicated care partner focus groups earlier in the research process to capture these valuable insights. Similarly, while individual interviews allowed staff to reflect on program challenges and successes, incorporating staff focus groups could encourage collective reflection and provide additional depth to program evaluations.
The exploratory use of GAS demonstrated its potential as a person-centered evaluation tool for YOD programs. By aligning program outcomes with participants’ personal goals, GAS offers a unique framework for understanding individualized impacts. However, challenges in applying GAS, including the need for external support to clarify and assess goals, highlight the importance of further adapting the tool to better align with the communication styles and preferences of persons with YOD.
One consideration for future evaluations is the potential impact of participant turnover, including both attrition and the addition of new program members over time. While this study focused on a relatively stable cohort, future research should explore how changes in program membership influence both the evaluation process and program dynamics. Incorporating flexible strategies for tracking participant transitions, as well as adapting engagement and data collection methods to accommodate new members, may enhance the continuity and applicability of findings.
This study underscores the importance of employing flexible and inclusive research methods when working with populations like persons with YOD. The findings contribute to the growing field of qualitative health research by: • Demonstrating how tailored methods, such as dyad interviews and interactive focus groups, can enhance inclusivity and participation for individuals with diverse communication abilities. • Highlighting the need to recognize and address the distinct contributions of multiple stakeholder groups, including care partners and staff. • Challenging stereotypes about persons with dementia by emphasizing their agency and capacity to contribute meaningfully to research. • Providing guidance for the use of individualized outcome measures, like GAS, in program evaluations.
By documenting these processes and reflections, this study contributes to the development of innovative research practices that prioritize inclusivity and empowerment. These insights aim to inspire future qualitative health research to continue exploring and addressing the unique needs of underrepresented populations, such as persons with YOD and their care partners.
Footnotes
Acknowledgements
We would like to express our heartfelt gratitude to the program members, care partners, and staff who generously contributed their time and insights to this research project. Your willingness to share your experiences has provided invaluable perspectives on how to meaningfully include persons with young-onset dementia in qualitative research. This work would not have been possible without your openness, collaboration, and commitment. Through your contributions, we hope to advance understanding and practices that promote the inclusion of persons with YOD in research and the development of more tailored, supportive services.
Ethical Statement
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by Sunnyside Seniors Services, Region of Waterloo.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.