
Abstract
Access to Sexual and Reproductive Health (SRH) care is a fundamental right but sustained underinvestment and high demand for services means accessing SRH care can be challenging. Barriers to access are a cause of health inequalities among women. Globally, novel ways to increase equitable access are being explored. This includes the potential for community pharmacies to provide routine services. This qualitative evidence synthesis aims to explore women’s perceptions and experiences of accessing SRH services in high-income countries and the role that community pharmacies can play in improving equity in access to SRH care. Peer reviewed journal articles from MEDLINE, CINHAL and EMBASE databases will be searched using a designated search strategy. This will be an iterative process depending on the number of articles found. The lead reviewer (supported by a supervisory research team) will assess the eligibility of articles, and extract data using a bespoke form designed for this synthesis. The methodological quality of included studies will be assessed using the CASP tool. A thematic synthesis approach will be utilised to analyse the data. Assessment of confidence in the review findings will be evaluated using the GRADE Confidence in Evidence from Reviews of Qualitative research (GRADE-CERQual) tool. Ethical approval is not required.
Background
Description of the Topic
Sexual and Reproductive Health (SRH) is a fundamental component of women’s health, well-being, and quality of life. Women are entitled to a distinct set of globally recognised SRH rights which includes access to information, resources, services, and supports necessary to achieve good SRH (WHO, 2006). Alongside these rights, there are a set of essential services integral to comprehensive SRH care for women, including evidence based SRH education; counselling, and care related to sexual function and satisfaction; provision of contraception; safe abortion services; and the prevention and treatment of Sexually Transmitted Infections (STIs). Access to SRH services has direct benefits for women’s physiological functioning and mental health and ultimately contributes to gender equality, social justice, and economic development (Stirling Cameron et al., 2021).
Improving access to SRH services is identified as key to tackling inequalities in sexual health outcomes (Ong et al., 2022). Kapilashram highlights the importance of intersectionality and poor sexual health outcomes and concludes that a fuller understanding and appreciation of the ways in which how intersectionality perpetuate inequities in SRH is required (Kapilashrami, 2020). There continues to be a strong correlation between deprivation and teenage pregnancy and higher rates of STIs within marginalised communities, such as those living in deprivation, some ethnic groups, younger people, and those without a General Practitioner (Garcia et al., 2021; The PLOS Medicine Editors, 2022). Access to abortion care is a key cause of inequality, with early termination less likely among women living in the most deprived areas (Public Health Scotland, 2023). Research from high income countries highlights the negative impact rurality plays in women’s experience of accessing abortion and other SRH services (Cashman C. et al., 2021; MacGilleEathain et al., 2023; Valentine et al., 2022).
With ever-increasing demands and sustained underinvestment in SRH services it has become increasingly difficult for women to access services to fulfil their SRH needs and rights (Otu et al., 2021). Policymakers around the globe are becoming interested in more flexible options for service access, including the potential to expand the scope of community pharmacy staff roles to complement provision by general practice and specialist SRH services (Agomo et al., 2018; Hindi, Jacobs, et al., 2019).
Community pharmacies are one of the most accessed healthcare providers and play a pivotal role in the global healthcare delivery landscape (Campeau Calfat et al., 2021). With longer opening hours and a wide geographical spread, community pharmacies are ideally situated to increase accessibility for people who may be hesitant to access traditional SRH services, struggle to attend an appointment during working hours or need to travel to access an appointment (Navarrete et al., 2021). There is a growing trend towards role expansion with a multitude of pharmacies across countries such as the UK, America, Canada, Australia and some European countries offering vital public health services like smoking cessation, lifestyle advice, substance use management, and some SRH services, such as emergency hormonal contraception (Navarrete et al., 2022). Some high-income countries have recently implemented policies to expand the role of the community pharmacist (Buckingham et al., 2023). These reforms are steering pharmacists beyond their traditional dispensing role, empowering them to assume more clinical and patient-centred roles (Hindi, Schafheutle, et al., 2019).
A recent international survey of community pharmacists found the majority were interested in additional training and expanding their role in SRH (Navarrete et al., 2023). Two UK landmark strategies signal a growing policy emphasis on women’s health, and both highlight how community pharmacies could play a role in this change (Department of Health and Social Care, 2022; Scottish Government, 2021). Scotland became the first UK nation to unveil a strategy exclusively dedicated to Women and Women’s Health (Scottish Government, 2021), which has SRH care as its focal point with England following suit in 2022 with its Women’s Health Strategy (Department of Health and Social Care, 2022).
Why is it Important to do This Review?
Delivery of SRH services varies widely (Navarrete et al., 2023). Traditionally SRH services have been provided by specialist SRH services, with Primary Care settings providing routine contraception, asymptomatic Sexual Health Screening, and treatment of chlamydia. Over the last 15–20 years Primary Care’s role has expanded to include some Longer Acting Reversible Contraception such as contraceptive implants and Intra-Uterine Devices. Since the early 2000's Community Pharmacists have added to this SRH service delivery by providing Emergency Hormonal Contraception (EHC) (Glasier et al., 2021) and in some area’s treatment of chlamydia (Willetts et al., 2018). With advances in medicine and laboratory technology there is increasing scope for services, such as testing and treatment of some STIs, to be provided outside of the specialist setting. This opens up the potential role of the community pharmacist.
A lack of comprehensive research hinders understanding of the optimal role for pharmacies and most effective implementation approach. Numerous pilots have explored delivery of different methods of SRH care within a community pharmacy setting (Cameron et al., 2020; Heller et al., 2017; Radley et al., 2018) but few have been translated into a permanent service delivery option. This poses a challenge even as the current policy environment underscores the imperative of expanding the community pharmacy’s role. Further research is required to explore how evidence from pilot studies can be translated into wider scale implementation and how the current system of SRH care delivery could be changed to improve equity of service access and delivery. In order to understand optimum role for pharmacies, there is need to understand the broader context of access and use across the whole spectrum of services, and to do so from women’s perspectives. A wider view is essential to understanding how community pharmacies fit within the whole system and the types of SRH services they are most suited to provide.
This review is the first stage of a larger project exploring the scope for expanding Community Pharmacy provision of SRH care within the SRH system in Scotland therefore the review will focus on high-income countries as research from these countries is most transferable across to the Scottish context (COMPASS). For the same reason the review will focus solely on in-person SRH services and not online or other forms of digital SRH delivery.
The project is aligned with Scotland’s Women’s Health Plan (WHP) which aims to improve women’s health inequalities by raising awareness around women’s health, improving access to health care, and reducing inequalities in health outcomes for girls and women, both for sex-specific conditions and in women’s general health (Scottish Government, 2021). One of the longer-term actions (>3 years) is to “provide more routine sexual healthcare through primary care, community pharmacies and online where appropriate, to enable specialist sexual health services to prioritise those most at risk of sexual ill health or unintended pregnancy”. Therefore, this review will contribute key evidence to inform future Scottish and UK policy.
Objectives
This qualitative review aims to synthesise evidence around women’s experiences of accessing and using in-person SRH services with a focus on the factors affecting access to these services. The review will focus on the SRH service delivery system as a whole, incorporating all in-person service options. It will explore the different characteristics and inequalities associated with each area of delivery. By synthesising the data found we will focus on community pharmacies and what role they can play in delivering more equitable SRH care.
The objectives of the review are: - To understand the factors affecting women’s experiences of accessing and using in-person SRH care across a variety of in-person service settings. - To understand how these factors differ amongst different groups of women, different SRH settings and the inequities that are present. - To understand if and how community pharmacies can play a role in delivering more equitable SRH care for women.
Methods
The aim of a Qualitative Evidence Synthesis (QES) is to establish nuanced understanding of issues that are subtle or sensitive in nature. In particular, the QES method enables greater understanding of individuals’ and groups’ experiences, views, beliefs and priorities for healthcare (Flemming et al., 2019). The QES, is a type of systematic review that brings together findings from primary qualitative research in a systematic way. This protocol adopts the Cochrane Template for Qualitative Evidence Synthesis (Glenton, 2023).
The RETREAT framework, which outlines seven key considerations that review authors should systematically work through when planning a review, was used when selecting an appropriate method for qualitative synthesis and due to a compressed time frame, it was decided to do a Rapid QES (Booth et al., 2108). The Cochrane Methods Group define Rapid Reviews as “a form of knowledge synthesis that accelerates the process of conducting a traditional systematic review through streamlining or omitting specific methods to produce evidence for stakeholders in a resource-efficient manner.” (Garritty et al., 2020). This can be done in several ways such as restricting the number of databases used, reducing the search period and restricting translation time.
Criteria for Considering Studies for This Review
Question Generation
Research Question Format (PerSPecTIF).
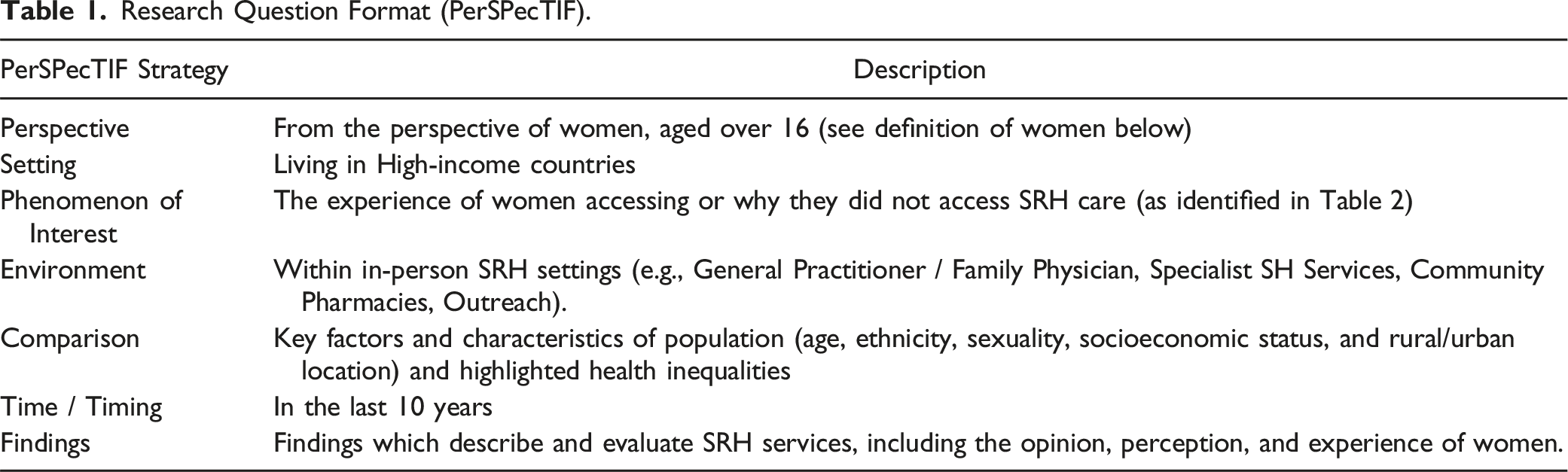
Though the review will have a key focus on Women’s Health and will use the term women / woman throughout it is acknowledged that it is not only those who identify as women who require access to women’s health and reproductive services. For example, some transgender men, non-binary people, or intersex people also experience SRH issues or require access to SRH services. When conducting scoping literature searches for this review I searched the 3 chosen databases for literature around transgender men, non-binary and intersex people accessing SRH services but found very little literature therefore this specific review will focus on articles which use the key term women. The lack of literature around transgender men, non-binary and intersex people accessing SRH services indicates a gap in evidence with further research required.
The Rapid QES will answer the follow questions: 1. What are the factors affecting access to in-person SRH care from the perspective of women in high income countries? 2. How do these factors vary across women with different characteristics (e.g. age, ethnicity, sexuality, socioeconomic status, and rural/urban location) and what inequities are evident? 3. How do these factors vary when comparing different settings of SRH service provision? 4. What does an understanding of the factors tell us about the potential for community pharmacies to increase equitable access to in-person SRH services?
Types of Studies
We will include qualitative studies, including mystery shopper which have qualitative data that can be extracted. Qualitative studies are uniquely placed to explore self-perceptions or lived experiences (Glenton, 2023). Any studies that generate qualitative data but do not use qualitative analysis methods will be excluded. Additionally, commentaries on the topic, research protocols, and quantitative studies will be excluded.
Concepts of SRH Included in this Review
The terms Sexual Health and SRH are often used interchangeably in many policies and documents (Berdzuli et al., 2020). There does not appear to be a globally understood definition of SRH. In fact, the WHO definition that is widely used is that of Sexual Health rather than SRH and this appears to be used most frequently within the literature making both terms synonymous with one another. The commonly used World Health Organisation definition defines Sexual Health as “…a state of physical, emotional, mental, and social well-being in relation to sexuality; it is not merely the absence of disease, dysfunction, or infirmity. Sexual health requires a positive and respectful approach to sexuality and sexual relationships, as well as the possibility of having pleasurable and safe sexual experiences, free of coercion, discrimination, and violence. For sexual health to be attained and maintained, the sexual rights of all persons must be respected, protected, and fulfilled.” (WHO, 2006).
Sexual Health or SRH provision encompasses a wide range of services SRH: fertility management, prevention, and management of STIs, sexual violence prevention and sexual function, desire, and arousal. The extent of evidence relating to women’s attempts to access these services is likely to be variable across concepts and sub concepts (explained in more detail in Table 1) (WHO, 2006). Understanding this variability is therefore important, as is synthesising evidence on variations between women’s access to these services.
Concepts of SRH Care in the Context of this Evidence Synthesis and Justification of Exclusion and Inclusion.

Concept of Access to SRH Services
Access to healthcare has been conceptualised across five dimensions: (1) Approachability; (2) Acceptability; (3) Availability and accommodation; (4) Affordability; (5) Appropriateness (Levesque et al., 2013). We will use these 5 dimensions as a guide within our data extraction fields when exploring service access within this review.
Search Methods for Identification of Studies
Search Strategy
A search strategy will be developed in consultation with an information specialist from the Social and Public Health Sciences Unit at University of Glasgow and the review authors. A copy of the search strategy can be found in Appendix 1. The search strategy will be validated against a set of core papers (n = 3) which will have been identified by the research team during scoping.
Summary of Inclusion and Exclusion Criteria.
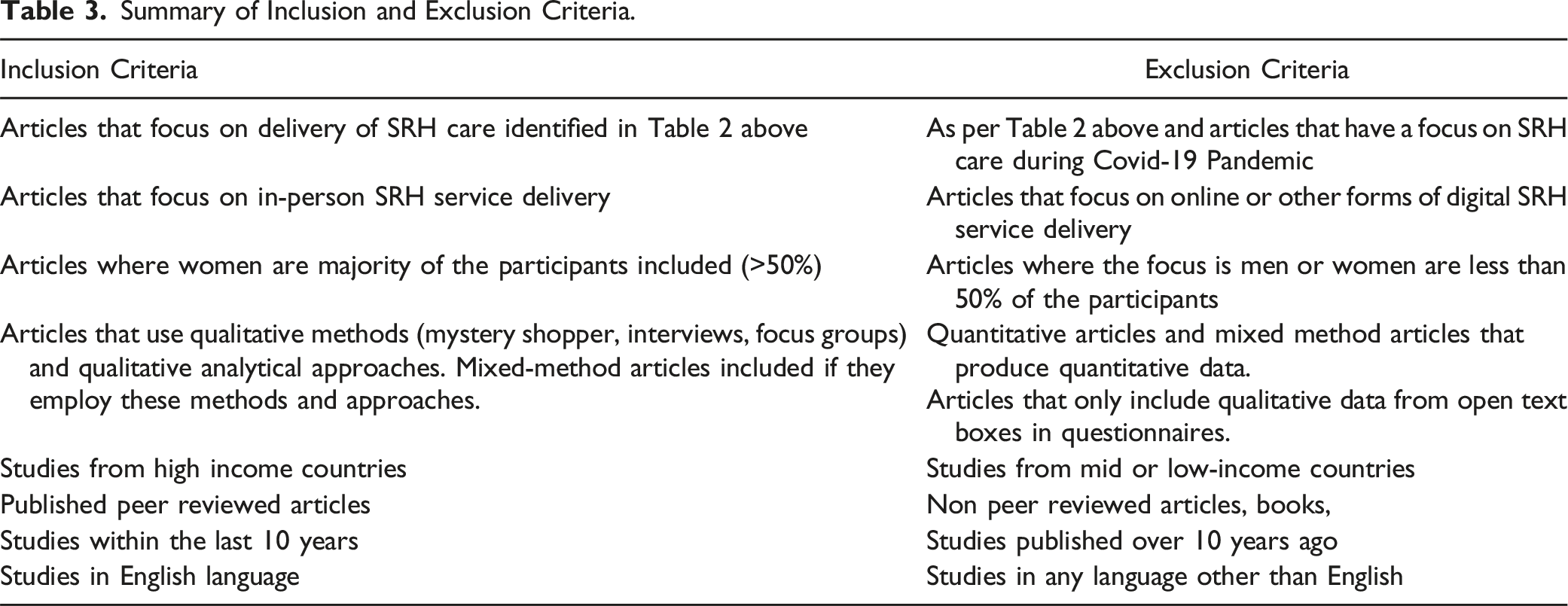
We will include published peer-reviewed studies identified through searches of MEDLINE, CINHAL and EMBASE databases. The number of databases has been limited to assist with the rapid review process. Grey literature, books, book reviews, un-peer reviewed preprints and dissertations will be excluded. Due to limited resources, only English language articles will be included.
The focus will be on articles published in the last 10 years. This reflects and is consistent with other reviews in this area which have utilised the same time frame to ensure findings inform current practice (Eades et al., 2011; Gauly et al., 2019; Gonsalves & Hindin, 2017).
Selection of Studies
All the publications identified will be imported into Zotero and duplicates will be removed. The lead author (KK) will assess the titles and abstracts of the identified records to evaluate eligibility with a second reviewer independently reviewing a subsection of articles (5%) by title and abstract. We will retrieve the full text of all the papers identified as potentially relevant.
The primary reviewer will then review the full text of the selected articles with 10% of the full-text articles reviewed by a second reviewer from the research team. Any disagreements will be resolved by discussion or, where required, a third review author.
Covidence software will be used throughout the rapid review to keep track of the selection and extraction process. Search results and the process of screening and selecting studies for inclusion will be visualised in a PRISMA flowchart.
Sampling of Studies
Qualitative evidence synthesis aims for variation in concepts rather than an exhaustive sample, and large amounts of study data can impair the quality of the analysis (Glenton, 2023). For this review we want to ensure that we have a suitable number of articles which can reasonably be analysed while also ensuring we achieve variation in SRH concepts and healthcare settings. Once we have identified all eligible studies, we will assess whether their number or data richness is likely to represent a problem for the analysis, and if so, the review team will discuss whether a purposeful sampling approach needs to be utilised. If this is required, we will adopt an Intensity Sampling process which involves selecting studies that are ‘excellent or rich examples of the phenomenon of interest’ (Suri, 2011). As suggested by Suri (2011) a purposive sampling approach helps reduce the number of studies involved in syntheses without compromising the integrity of the analysis. This purposive framework will focus on the richness of the data using the 1–5 richness assessment scale (Ames et al., 2019). Additionally, we will seek to use papers that give us a good spread of examples across SRH settings, such as specialist SRH services, community pharmacies or GPs.
Data Extraction
The lead reviewer will extract data from each sampled study. To ensure consistency, a data extraction tool developed in Covidence will be used to record key information in the article and data will be extracted by the lead reviewer from all sampled studies. A second reviewer from the review team will independently extract data from a subset of studies. Each article will be analysed with a focus on method of SRH care, key findings around experience of accessing SRH care, identified factors to access and any recommendations. The proposed data extraction fields will be piloted with a small number of studies (n = 5) and discussed within the research team to ensure transparency and appropriate information is captured. It will be adapted as required.
Proposed data extraction fields: • Author. • Publication year. • Country of origin. • Key SRH concept/s of focus (as highlighted in Table 2). • SRH setting/s (Specialist SH Service, General Practitioner, Community Pharmacist, other). • Demographic information and characteristics of participants. • Any identified inequalities in access highlighted. • Identified experiences, perceptions, and opinions of accessing SRH care (categorised by the 5 domains of access discussed earlier: Approachability; Acceptability; Availability and accommodation; Affordability; Appropriateness). • Identified barriers and enablers. • Any documented recommendations.
Data extraction for a QES falls into 2 categories; the contextual data and the ‘findings’ which take the form of quotes, themes, sub-themes and author interpretations (Flemming & Noyes, 2021). The data extraction tool, which has been specifically developed for this review, will include both contextual data and the more qualitative findings. Typically, data extraction, analysis and synthesis involves movement backwards and forwards between them therefore the extraction, analysis and synthesis will be an iterative process.
Assessing the Methodological Limitations of Included Studies
The lead review author will assess studies’ methodological limitations, using the CASP tool, with a second reviewer independently assessing the methodological limitations of a subset of studies. The CASP tool is the most commonly used tool for quality appraisal in health-related qualitative evidence syntheses (Long et al., 2020). An adapted version of the CASP Qualitative Studies checklist will be used based on the following domains such as context, study design, data collection, and data analysis (CASP, 2023).
Data Management, Analysis, and Synthesis
The qualitative data extracted will be analysed with the contextual data extracted to look for patterns between either SRH setting or participant characteristic. A thematic synthesis approach will be taken with the qualitative findings as described by Thomas and Harden (2008) to generate descriptive and analytical themes. The three stages of thematic synthesis are: line by line coding of the qualitative ‘findings’ extracted, development of descriptive themes encompassing similar codes and development of analytical themes (Thomas & Harden, 2008). A narrative synthesis will be produced which will discuss each of the key themes, known as a Summary of Qualitative Findings. Any limitations within the rapid review will be acknowledged and discussed.
Assessment of Confidence in the Review Findings
The GRADE-CERQual (Confidence in the Evidence from Reviews of Qualitative Research) will be used to assess confidence in the review findings as developed and outlined by Lewin et al. (2018). The four approaches: (1) methodological limitations, (2) coherence, (3) adequacy of data, and (4) relevance will be used (Lewin et al., 2018). The GRADE-CERQual assessment for each finding will be made by the lead reviewer and be discussed with the research team, prior to being presented in a summary of qualitative findings table.
Summary of Qualitative Outcomes Table(s)and Evidence Profile(s)
We will present summaries of the analytical statements and of our assessments of confidence in these findings in the Summary of Qualitative Themes tables. Additionally, we will include an Evidence Profile which details descriptions of our confidence assessments.
Author Reflexivity
The lead reviewer (KK) will be supported by the research team (RL and KM) both of whom are experienced qualitative researchers and reviewers. The lead reviewer has clinical experience in SRH which may influence how the data is interpreted or choice of article selection. The research team will meet regularly during the review process to discuss and highlight any unconscious bias.
Footnotes
Acknowledgments
We would like to thank Valerie Wells, Information Specialist within the MRC/CSO Social and Public Health Sciences Unit, for her comments and guidance in designing the search strategy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a PhD studentship (KK) from the Medical Research Council. KM and RL were supported by the UK Medical Research Council (MC_UU_00022/3) and the Scottish Government Chief Scientist Office (SPHSU18).
Ethical Statement
Appendix
Search Strategy.
#
Query
1
((pharmac* or druggist or chemist) adj1 community).ab,ti,kw.
2
“community pharm*”.ab,ti,kw.
3
(family physician or general practitioner).ab,ti,kw.
4
(sexual Health adj (clinic or service)).mp. [mp = title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword heading word, floating subheading word, candidate term word]
5
(family planning adj (clinic or service)).mp. [mp = title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword heading word, floating subheading word, candidate term word]
6
1 or 2 or 3 or 4 or 5
7
(contraception or contraceptive).ab,ti,kw.
8
Contraception/ or Contraceptives, Oral/or Contraceptives, Oral, Combined/
9
“pre-conception care”.ab,ti,kw.
10
“free condom*”.ab,ti,kw.
11
(Sexually Transmitted Diseases/or Chlamydia trachomatis/ or Gonorrhea/) and screening.ab,ti,kw.
12
((Gonorrhea or Chlamydia or STI or sexually transmitted disease*) adj2 (treatment* or screening)).ab,ti,kw.
13
((HIV or Hepatitis C or Hepatitis B or Syphilis) adj2 (treatment* or screening)).ab,ti,kw.
14
Menopause/ adj2 (service or care or advice).ab,ti,kw.
15
((menopause or menstruation or menstrual) adj2 (health or service or care or advice)).ab,ti,kw.
16
Contraception, Postcoital/
17
(emergency contraception or morning after pill).ab,ti,kw.
18
(pregnancy adj (testing or advice)).ab,ti,kw.
19
(mifepristone or misoprostol or medical abortion).ab,ti,kw.
20
sexual assault/ or rape/
21
(pre exposure prophylaxis or PreP).ab,ti,kw.
22
(post exposure prophylaxis or PEPSE).ab,ti,kw.
23
7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22
24
(enablers or facilitators).ab,ti,kw.
25
(challenges or barriers or difficulties or obstruction).ab,ti,kw.
26
24 or 25
27
6 and 23 and 26
28
limit 27 to (english language and yr = “2013 -Current”)