
Abstract
Keywords
Introduction
Much of the existing vision loss research details the adverse implications of vision loss on quality of life, including limitations in practical and physical mobility, restrictions in leisure activities, self-care, and employment (Klauke et al., 2023). However, the embodied experience of vision loss needs to be better understood. The subjective and inter-subjective experiences that are concomitant with visual impairment, and how persons with visual disabilities encounter society from an intersubjective perspective, are crucial aspects of disablement and how disabled identities are constructed (Loja et al., 2013). Yet, non-disabled responses to visible impairment have been historically characterised by social invisibility and, in some cases, over-attentiveness (Loja et al., 2013). Understandings of impairment are rooted in ableist discourses, which Campbell (2001) defines as “a network of beliefs, processes and practices that produces a particular kind of self and body (the corporeal standard) that is projected as the perfect, species-typical and therefore essential and fully human” (p.44). As noted by Bruce (2020), ableism is entrenched into “our everyday thoughts and actions, often rendering us largely unaware of its force in our lives. We breathe its logic, are shaped by its politics, and are unknowingly complicit in nurturing its power” (p. 127). In research, ableism constitutes a profound systemic issue that is manifested in the methodologies employed, how research questions are framed, and how data findings are interpreted, inadvertently perpetuating and reinforcing stereotypes (Loja et al., 2013). Traditional research paradigms often take up a normative view of ability whereby studies are designed in accordance with the experiences of nondisabled individuals, conceptualised as legitimate study subjects. Aside from concerns regarding the accessible design of research, disabled people remain an underrepresented part of the academic institution where knowledge is produced. Indeed, the neoliberal academy generally assumes non-disabled academic faculty, staff, and students (Brown, 2021; Brown & Leigh, 2018; Price, 2024; Rice et al., 2023). For instance, in a recent systematic review, Lindsay and Fuentes (2022) found that experiences of ableism in academia are widespread, citing decisions to disclose, a lack of accommodations, and prevailing negative attitudes as indicators of a presumed non-disabled academic subject and disabling for, and disruptive to, the academic careers of faculty and staff with disabilities. There is an imperative to challenge such entrenched practices to produce accessible, and thus inclusive, research designs that culminate in equitable processes of knowledge creation.
It is important that the embodied experience of visual impairment is understood to validate the impaired body within academia, and critical disability studies (CDS) more specifically, and to destabilise ableism by highlighting variations in the human body (Jones, 2006). Spanning the humanities, social sciences, and educational studies, CDS refers to an interdisciplinary academic field that, broadly speaking, rejects individualistic and biomedical understandings of disability and by extension the dominant notion that disabled people need to be ‘cured’ or ‘fixed’; prioritizes the lived experiences of disabled people; conceptualizes disability as a social, political, and material phenomena and identity; identifies and challenges ableism within structures and systems; and recognizes the ways in which ableism intersects with many other oppressive systems, such as racism, heterosexism, cissexism, colonialism, and sexism (Clare, 2017; Ellis et al., 2018; Goodley et al., 2019; Kafer, 2013; McRuer, 2006; Schalk, 2022). In CDS, the theory of embodiment postulates that disability is not merely a medical condition but a complex intersection of the body, society, and personal experience (Flynn, 2021). This theory explores how bodily differences are experienced by individuals in diverse contexts and how these experiences influence identity, capability, and perception (Siebers, 2013). Researchers in this field challenge the traditional views that frame disabilities strictly as limitations, proposing instead that disability offers unique modes of interacting with the world, which can enrich communal understandings of human diversity. Embodiment theory underscores the relational aspect of the body with its environment; for individuals with disabilities, this includes the physical and attitudinal barriers they encounter (Mackenzie & Scully, 2007). Crucially, this framework offers insights into how the environment’s accessibility dramatically influences how disability is experienced and lived. Disability studies often draw on embodiment to critique how societal norms shape perceptions of normalcy and ability. This critique examines the ‘corporeal standards’ that define which bodies are valued and which are not. It interrogates how cultural narratives around health, productivity, and aesthetics marginalise those who do not fit these norms, leading to discrimination and social exclusion (Flynn, 2021).
Critical participatory action research (CPAR) can encourage the direct participation of individuals with disabilities in the design, development, and dissemination of research that seeks to understand their embodiment of disability (Balcazar et al., 1998). CPAR constitutes a collaborative commitment to empowering people through their direct participation in the research process; knowledge is therefore derived from their subjective and socially-situated experiences (Kemmis et al., 2014). Against this backdrop, CPAR represents a radical departure from dominant research processes, within which individuals with disabilities have been conceptualised as passive objects of study (Nind, 2017), particularly under the medical model of disability. The medical gaze frames disability as an individual problem in need of individual solution (Hughes, 2000; Kitchin, 2001; Loja et al., 2013). In contrast to biomedical conceptualizations of disability, the present study takes up a CDS lens (Goodley, 2013), which moves beyond individualizing disability and instead examines how underlying systems, structures, practices, and institutions serve to disable people (Terzi, 2004). When this same lens is applied to research practices, it demands a more critical analysis of the failures of traditional research approaches that serve to legitimise sighted ways of knowing and doing.
CPAR has, in recent times, sought to reveal disadvantages linked to ethnicity, social class, and gender (Kemmis et al., 2014). Comparatively, the uptake of CPAR in relation to disability has been somewhat limited; even still, there is a pervasive tradition in qualitative research of constructing “sighted individuals as natural and, therefore, legitimate producers and purveyors of knowledge” (Bruce, 2020, p. 128). In fact, by viewing disability overwhelming as a ‘deficit’, it has meant that non-disabled researchers are often positioned as the “unquestioned experts on all things disabled” (Bruce, 2020, p. 127). Such boundaries are further compounded at the intersection of disability and age, such that aging persons with disabilities are often assumed to lack the capacity to fully engage in participatory processes (Corrado et al., 2020). Yet, the core tenets of CPAR supports the inclusion of older adults and persons with disabilities in research practice. CPAR emphasises collaboration in the iterative cycles of research, including planning, implementation, reflective practice, and dissemination (Kemmis et al., 2014). The overarching aim of CPAR is to empower marginalised community members to collaborate in research projects so that their experiences and challenges can be understood, and socially situated, as a starting point for designing effective solutions. Within this framework, it is the participants that identify the research problem by drawing upon their lived experiences; they also play a role in the collection and analysis of data, processes that are directed towards the end goal of social and/or political transformation (Balcazar et al., 1998). At the heart of this approach is the recognition that all participants have knowledge and expertise, which, based on collaboration with experienced and trained researchers, can be leveraged to produce a more inclusive research process. An important implication of this assumption is that the research process is controlled conjointly by the researcher and the research participants, acknowledged as co-researchers, as part of a broader process of knowledge co-production.
CPAR presents older adults and persons with disabilities with an opportunity to articulate their experiences and knowledge while concurrently participating directly in processes that seek to define, analyse, and address these experiences via solutions. Equitable participation and inclusion are the fundamental principles of CPAR, resulting in more authentic analyses of participants’ social realities (Balcazar et al., 1998). These principles encourage participants to share the subjective aspects of their experiences, albeit complemented by the views of the researcher. CPAR is rooted in the acknowledgement of multiple truths and realities, which brings forth a nuanced and contextual interpretation of lived experiences and realities. The accumulated knowledge can be important for advocating for change, which is a crucial aspect of mobilizing social transformation. Indeed, CPAR can boost awareness among older adults, and people with disabilities, about their strengths as co-producers of knowledge which invariably exposes the possibilities of their role as integral resources in the research process.
Research Question and Methodology
Against this backdrop, the present paper aims to unpack how our research collective carried out accessible and inclusive CPAR with older adults with vision loss. The research collective is comprised of three academic researchers, two older adults with vision loss, two student research assistants/associates, one policy advisor, and one vision loss service provider, all of whom were invited authors on this paper. Using meeting notes, group discussions, and reflection as the primary data collection methods, the research collective set out to answer the following question(s): 1) How has the research collective worked to enact an inclusive and accessible CPAR study that supports the full participation of older adults with vision loss? 2) What has the research collective learned through reflecting on the process regarding challenges and strategies for working towards an inclusive and accessible CPAR?
The researchers situate themselves as scholars who are disabled/allied with disabled embodiments across the life course, and consequently, their role as ‘insiders’ (Chammas, 2020; Dwyer & Buckle, 2009) is critically discussed to establish their positionality. The primary author has been engaged in research with communities experiencing vision loss, especially those aging with, and into, vision loss, for over ten years. This immersion provides a certain degree of authenticity and has enabled rapport and trust to be built with low vision service providers as well as older adults aging with vision loss. Developing trusting relationships can “enhance participants experiences of the research process and can help to reduce the power inequalities between participants and researchers” (Novek & Wilkinson, 2019, p. 1048).
The fundamental principles of CPAR, inclusion and accessibility, provide a framework for the present study. However, the research collective recognises that the word inclusion can be problematic when it is framed as a skill to be developed by the individual, with inclusion being achieved through the provision of individual accommodations (Bruce, 2020). It also serves to downplay or naturalize the ways in which most settings are created for able-bodied and able-minded people as the ideal or preferred subject user. Inclusion, as it is taken up in this paper, needs to be the mission of all researchers to transform longstanding and systemic discrimination evident within traditional research approaches and the academic institution itself (Bruce, 2020). As such, the present paper will show that producing access is a collective and desirable on-going endeavour and that older adults with vision loss have expert knowledge and, therefore, should be at the centre of the research process.
Johnson & Walmsley (2003) have proposed several distinguishing features of inclusive research which have been adopted, and modified, by our research collective to include the following key assumptions. These assumptions guide our work at each stage of the CPAR process including: 1) The research problem should be established and owned by older adults with vision loss. 2) The research problem(s) should further the interests of older adults with vision loss and ultimately lead to improvements in their lives. 3) The research must be collaborative, while representing the views and experiences of older adults with vision loss. 4) Older adults with vision loss hold control over the research processes and outcomes. 5) Older adults with vision loss are treated with respect by the research community. 6) The information shared is accessible to all co-researchers, including those with vision loss.
Results
In this paper we outline the methodological decisions made by the research collective to ensure an accessible and inclusive CPAR with older adults with vision loss. Those methodological decisions are broken down into four key stages in the CPAR process including: (1) study planning stage; (2) data collection stage; (3) data analysis stage; and (4) knowledge mobilization (KMb) stage.
Study Planning Stage
With its commitment to involving community members as co-researchers in a cyclical process of identifying issues, reflection, conducting research, and implementing results (Blair & Minkler, 2009; Kidd & Kral, 2005), CPAR is a promising methodology capable of bringing about personal and social transformation. Although there are multiple examples of CPAR involving young people (Kim, 2016; Livingstone et al., 2014; Ozer, 2017; Schensul & Berg, 2004; Shamrova & Cummings, 2017), there are no present examples of CPAR taken up with older adults aging with vision loss, with the exception of (McGrath, 2021) which outlined the initial steps of a CPAR process whereby the focus was on setting research priorities. Although there may not be examples of specific CPAR studies, there is certainly a commitment to building inclusive research practices that foster the full participation of persons with disabilities, which has been discussed in previous, albeit recent, literature as it relates to deaf-blindness (Watharow & Wayland, 2022), persons with learning disabilities (Milner & Frawley, 2019; Nind, 2017), people living with dementia (Novek & Wilkinson, 2019) and people with vision loss (Bruce, 2020). In fact, Milner and Frawley (2019) have argued that including persons with a disability in research reflects “a more socially just way of knowing disabled lives” (p. 383) and such inclusive methods are one way “for researchers to write the hermeneutical injustice of failing to engage them in the development of inquisitorial frameworks that articulate their own experiences” (p. 383).
Mission, Vision, and Values.
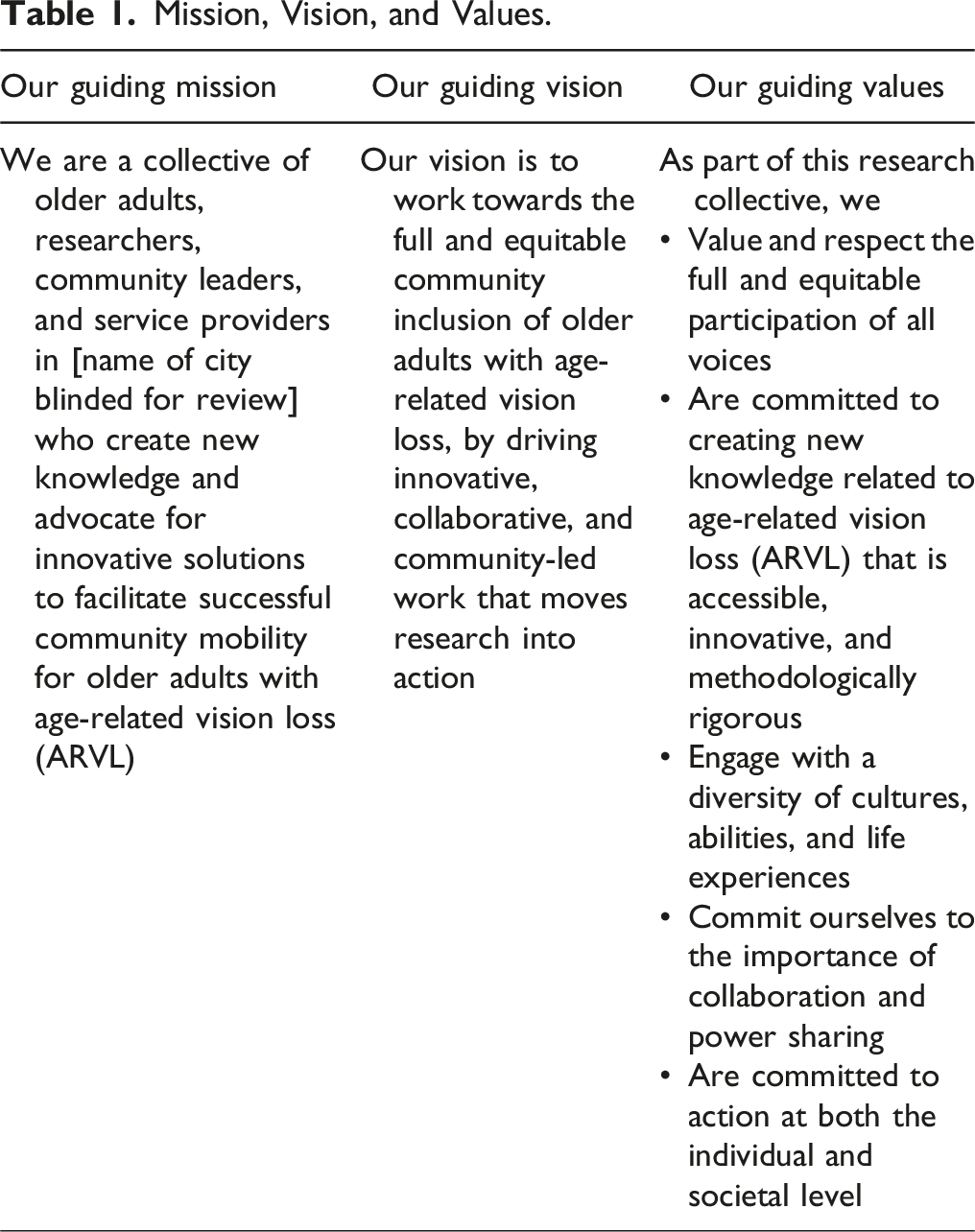
In addition to ensuring representation of persons with vision loss on the research collective, we were committed to the CPAR ideals of shared power and ownership within the research process (Berg, 2004) as well as equitable collaboration (Meyer, 2000). To enact those principles, our research collective made methodological decisions to ensure all team members could engage meaningfully in the research process. For example, all study documents were made available in large print, braille, and/or as audio recordings. In addition, we circulated all meeting materials in both Word and PDF to enable the use of screen reading software. As it pertained to those older adults with vision loss who engaged in the study as research participants, we read out letters of information during the recruitment phase, if desired; accepted verbal consent over written consent if preferred; and used signature guides to facilitate written consent.
A final strategy we enacted to ensure accessibility for research collective members with vision loss was the continued use of Zoom for meetings long after COVID-19 required virtual meeting attendance. There are known structural barriers to Zoom that have been noted in the literature such as cost of internet, geographic variability of internet quality, and required digital literacy skills. Even still, Zoom was the preferred meeting method for participants with vision loss, who were otherwise concerned about the travel, both in terms of cost and needing to enlist the help of a family member or friend to drive, necessary to attend meetings. We enlisted several strategies to use Zoom in an accessible and inclusive way. For example, training was offered at the onset of COVID-19 on the use of Zoom and keyboard shortcuts, all members are requested to state their name each time before speaking, orientation is always provided when reviewing documents and/or visuals on the shared screen by clearly explaining, verbally, anything that is shown visually, and we avoid tables and graphs whenever possible due to the difficulty some members of the research collective have reviewing such information using their screen reading software. Many members of the disability community, especially those who are immunocompromised, advocate for continued use of Zoom and our research collective will continue to do so, at the request of our members with vision loss. As a further strategy to minimize the risk of exposure to COVID-19 (and/or other airborne illnesses), and to participate in community care, the Research Associate for this study, wears N95 masks when interviewing indoors, unless this poses a barrier to accessible communication for the participant; for instance, if the participant reads lips.
Data Collection Stage
Prior to beginning the data collection phase of the CPAR study, the research collective required all hired research assistants (RA’s) to be trained in sighted guide, which is a technique to safely, and respectfully, guide someone who is B/blind or partially sighted. This was a decision made by the research collective not only to help maximize the safety of older adult participants during the go-along interview (see methodological details on the go-along interview below), but also as an acknowledgement of the difficulties often encountered by participants during experiences of community mobility. When it came to choosing the methods of data collection that would be used, this was a shared decision made by the research collective, thereby ascribing to the CPAR principle of collaborative decision-making (Berg, 2004). Interestingly, the research collective proposed several visually based methods that have not otherwise been taken up in studies with older adults with vision loss, the details of which will be explained below. The research collective is at the stage of data collection and so these methods are currently being trialed.
The first data collection session is a spatially informed narrative interview with visual mapping. The research collective proposed to use Wengraf’s (2001) Biographic-Narrative-Interpretive Method (BNIM) approach to interviewing, whereby participants are asked a single question: “Since noticing the changes in your vision, can you tell me about the places you go, or would like to go, in your neighbourhood?” The research collective decided to couple this with spatial mapping (Huot, Aldrich, Laliberte Rudman and Stone, 2022) as a means of visually representing those places in the neighbourhood that the participant travels to, how they get to those places, and the barriers to their walkability that are experienced. Practically, this method is achieved by the older adult describing verbally how they access the environment, while the RA depicts it visually on a map. A direct benefit of this approach is that is draws out details that would otherwise be overlooked in a narrative interview. To create a more accessible end-product, the research collective plans to use a combination of raised dots and fabric/puffy paint added to the map to create a tactile neighbourhood map that could be shared with research participants, and members of the broader community, at a community forum held after the data collection phase is completed.
The second form of data collection that was decided upon by the research collective is a go-along interview (McGrath & Laliberte Rudman, 2019), which allows the researcher to explore participants’ physical and social practices by asking questions, listening, and observing. The focus of the go-along interview is to travel to destinations in the neighbourhood, chosen by the participant, to learn how environmental factors shape experiences of walkability for older adults with age-related vision loss (ARVL). ARVL is defined as low vision related to the natural ageing process encompassing the conditions of glaucoma, macular degeneration, and diabetic retinopathy (McGrath et al., 2017). The go-along also includes the participants’ choice of either a video recording or photo renderings to visually record the experience. An iPhone was used to capture photos while a chest-mounted Go-PRO was used to record video data. All photos and video renderings are shot by the research associate; however, the choice of what to document is at the sole discretion of the older adult with vision loss.
The third, and final, method of data collection is a narrative interview that affords participants the opportunity to share any final thoughts/experiences related to community mobility. Though not a visual method of data collection, it does provide a rich lived experience perspective.
Finally, the research collective chose to perform environmental audits in four neighborhoods in London, Ontario, Canada in the summer of 2022 using the “Road Safety Audit Tool for Pedestrians who are Vision Impaired”, developed by Victoria Walks in association with Vision Australia and Guide Dogs Victoria. Audits were aimed at identifying barriers to walkability for persons with vision loss using three checklists: signalized intersections, non-signalized intersections, and path infrastructure. Photos accompanied all written reports to provide a visual cue of the barrier identified. The audits were always conducted/completed alongside a member of the research collective who had vision loss to ensure that we were picking up on those experiences that a sighted person may not be attuned to, such as, but not limited to, the volume of the locator tone at an audible crosswalk or the impact to safety when crossing the road when tactile ground surface indicators were not present.
In terms of research practicalities, we also provide participants with control over the research space, allowing the older adults with ARVL to choose when and where the research activities will take place and how the environment will be set up to ensure optimal communication. Further, we are committed to providing choice to the study participants regarding the pseudonym they will adopt. This was particularly important to ensure privacy given the relatively small network of older adults with vision loss in London, Ontario, Canada but also as a strategy to promote collaboration and the sharing of power (Lahman et al., 2023).
Data Analysis Stage
The research collective started data analysis in the winter of 2024 and was met with some challenges due to the presumed importance of sightedness during textual analysis. As Bruce (2020)—a self-identified blind researcher, who outlined her approach to data analysis and coding—identifies, many of the tools used for data analysis are incompatible with “auditory ways of working and knowing,” which are prevalent among researchers with vision loss (p.128). In fact, there is an underlying presumption of sightedness within academia, such that it does not include researchers whose way of doing research may be seen as incompatible with established methods of data analysis (Bruce, 2020). The research collective encountered this presumption when anonymized transcripts were shared with the collective’s community and faculty co-researchers. Although the transcripts were accessible to one blind researcher with advanced screen reader technology, we quickly realized that two members with vision loss were unable to access the transcripts because the documents’ formats were incompatible with their individual screen reader technologies. After this meeting, [MS] (an Accessibility and Inclusion Advisor) explained to [JM and other interested co-researchers] how to make the already transcribed documents screen reader-friendly and demand document accessibility standards from future transcription companies. Important recommendations included: avoiding the use of tables (nearly all the previously transcribed documents used tables to convey speech) and using proper and descriptive headings—especially relevant for lengthy documents, like transcripts. To ensure everyone could participate, analysis was paused until JM could correct each document’s inaccessibility to foster meaningful access. JM also met individually with community researchers to learn more about the particulars of their various, and sometimes dated, screen reader technologies to help mitigate possible technology and inaccessibility issues in the future. Data analysis meetings resumed once everyone in the collective was able to listen to and/or read the transcripts. Notably, data analysis meetings also include B/blind practices, such as saying your name before speaking and offering self-descriptions (i.e., a brief physical description of your clothing, hair colour or style, race, age, accessories, and/or mobility aids) and pronouns, since gender cannot be determined by voice or appearance (see Reid, 2022).
Relatedly, to further ensure inclusiveness and accessibility in our approach to data analysis, the research collective is currently considering how to offer more meaningful forms of data analysis that deprioritize sighted/visual methodologies and, instead, privilege “blind/auditory ways of doing” research (Bruce, 2020, p. 134). Following Bruce’s approach (2020), the collective is aiming to provide the choice to all members to analyze the data by either listening to transcripts (via screen reader technology) or the original audio recordings, thereby connecting more specifically with the voices of the participants. Currently, EM is experimenting with both options.
Finally, the research collective has also discussed moving away from traditional coding practices, given that computer assisted data analysis programs are generally incompatible with screen reading software and this type of approach relies heavily on visually sorting by colors or other visual cues, such as bolding, underlining, or highlighting (Bruce, 2020). As well, the knowledge and skill required to learn data analysis programs may present a barrier to participation for some co-researchers, and, even with the appropriate training and technology, co-researchers may be uninterested in this type of data analysis activity. To this end, JM, a sighted researcher, is coding using traditional data analysis software, and EM, a blind researcher, is listening to interviews and developing participant profiles to bring to light those patterns, story details, and perspectives garnered from engaging in a more auditory approach to data analysis (Bruce, 2020). Both forms of coding are heavily informed by monthly data analysis meeting discussions with community co-researchers, who are generally less invested in creating codes or participant profiles and more interested in listening to the transcripts and contributing their own experiential knowledge as older adults aging with/into vision loss. Central to our analysis is the application of auditory methods in addition to traditional visual or text-based coding systems. The overarching aims of this adjustment are to: design and enhance access in research by enabling members of the research team with vision loss to engage directly and meaningfully with the original audio recordings; and strengthen data analysis through incorporating auditory ways of knowing, which may be better situated to document subtleties that might otherwise be lost in transcription. Our data analysis, therefore, entails an inclusive and innovative approach that adapts traditional methodologies to address the diverse abilities of both study participants and researchers.
Most importantly, we have recognized that there is not a one-size-fits-all approach that can be applied to data analysis when working with members of a research collective that may engage with data in more auditory versus visual means and that cultivating access is an ongoing and relational process that can be supported through fostering ‘access intimacy’ (Mingus, 2011) in research and academia (Valentine, 2020). Ensuring accessibility and inclusivity in the data analysis stage, requires adopting a more fluid and user-driven approach that allows for choice and autonomy in decision-making. This approach, where choice is provided to each member of the research collective, is also in line with the guiding principles of PAR.
Knowledge Mobilization (KMb) Stage
Including co-researchers in all phases of the research process (Blair & Minkler, 2009; Frisby et al., 2005; Minkler, 2010), is a central tenet of CPAR and includes the KMb stage. Our focus on inclusive KMb is ongoing given that data collection is on-going. Our approach to disseminating knowledge has, and will continue to, adopt a critical knowledge mobilization approach which is defined by Grenier et al. (2021) as “contextual and reflexive engagement in the production and sharing of knowledge that challenges the conceptual separation of science, technology, and society, and creates space for an open and inclusive research infrastructure where stakeholders can be both knowledge creators and contributors” (p. 348). In looking at knowledge mobilization as a critical process, our team has reconfigured KMb as a social responsibility that is achieved through adopting the principles of “reflexivity, collaboration, community engagement, and inclusivity” (Grenier et al., 2021, p. 350) and that only occurs when co-created between academic researchers and relevant stakeholders, which in our case includes older adults with vision loss.
To date, and at a minimum, we have meaningfully included all members of the research collective in conference presentations and publications and ensured extensive feedback was obtained on all outputs produced, such as an audit report and policy briefs. We also employ the services of a graphic designer who is proficient in accessible design, specifically working with the B/blind and partially sighted community, to ensure any online tools as well as documents produced are accessible in print form, and with screen reading software. Lastly, we include budget lines in our grant applications for funding for older adult co-researchers with vision loss to attend conferences to co-present findings and to support persons with vision loss to attend conferences with a sighted guide/support person, which is essential to support the meaningful participation and inclusion of the B/blind and partially sighted community in academic discussions. In addition to including members of the research collective in KMb strategies, we are also committed to providing study participants with updates on the study’s progress to minimize the risk of participants feeling used or devalued by researchers who fail to report back the study progress and outcomes (Novek & Wilkinson, 2019).
Given that critically informed KMb is not a static endeavor reduced to an end- product of outcomes, but rather is contextually situated, collaborative/inclusive of all voices represented on the research collective, and is socially minded (Grenier et al., 2021), our commitment to KMb will be ongoing throughout this CPAR project.
Discussion
This reflexive paper highlights the steps being taken by a research collective to enact an inclusive and accessible CPAR study that supports the full and equitable participation of older adults with vision loss, including a reflection on the strategies that worked, and the challenges encountered thus far in this on-going process. We conclude with a discussion highlighting what has been learned, with respect to building inclusive research practices, that our research collective, and other teams, can take forward in future research that endeavours to be inclusive and seeks to cultivate access.
An important learning of the research collective is that one approach does not fit all and that building inclusive research practices is an iterative process. There is no set of principles or quality criteria that can be applied to determine if one’s research is inclusive. In fact, there is no right way to ‘do’ inclusive research, but rather it’s a process of learning that requires taking ample time to work through challenges and design solutions. There are, however, some questions, as adapted from Nind & Vinha (2012), that our research collective has asked ourselves throughout the process, to determine if we are heading in the direction of inclusivity, including: 1) Is the research topic relevant to the lives of older adults with vision loss? 2) Does the research have the potential to inform real world personal and/or social transformation? 3) Have older adults with vision loss been involved in the research process in a meaningful, authentic, and active way? 4) Has choice and autonomy been provided throughout the research process? 5) Have older adults with vision loss been treated with respect throughout the research process? 6) Has the research team been committed to providing information in accessible formats to ensure that individuals with vision loss can understand, and respond to, information provided?
Choice, autonomy, and control, in combination with flexibility, were paramount to building an inclusive CPAR study and was provided at all stages of the research process, thereby demonstrating our commitment to shared and collaborative decision-making. With respect to the research collective members with vision loss, choice regarding what aspects of research to be involved in was provided. This was paramount given that research suggests that “allowing choice and flexibility promotes inclusivity and it can also give participants some control over the research” (Novek & Wilkinson, 2019, p. 1048). As it pertained to the older adults with vision loss who participated in data collection, control over the research space was prioritized, which meant inviting participants to choose when, and where, the research activities would take place and how the environment would be set up to ensure optimal communication. For example, choice over the time of day, duration of interviews, and location of the research meeting was paramount (Hubbard et al., 2003; McKillop & Wilkinson, 2004) not only to encourage optimal communication but also to maximize research participant comfort.
In relation to flexibility, we also learned that it is vitally important to engage in flexible communication approaches that are responsive to the participants needs and abilities (Digby et al., 2016; Heggestad et al., 2013). For example, as noted above, we used a variety of approaches to maximize communication such as large print, braille, Word copies for better compatibility with screen reading software, audio recordings, and maintained the use of Zoom. As it pertained to those older adults with vision loss who engaged in the study as research participants, we read out letters of information during the recruitment phase if desired, accepted verbal consent over written consent if preferred, and used signature guides to facilitate written consent. We also engaged in flexibility in the research process by building in time for informal chats with the participants, which was regularly used to build rapport. We were also flexible in conducting 1–2-h interviews over multiple sessions or with several breaks to ensure participant comfort.
Inclusivity has become a mission at many academic institutions; however, there is a tension between the aims of inclusive research and the institution of academia (Milner & Frawley, 2019), whereby accessibility within academia is often predicated on the notion of developing individual skills or providing accommodations at the individual level which, although helpful, means that institutions rarely consider the transformation of long standing traditions (Bruce, 2020), such as that of their obstructive ethics processes which can often deter participation of the most marginalized and hinder, and/or slow, community action and networking. Although not explicitly addressed in this paper, inclusive research practices are significantly impacted by obstructive ethics processes, including, at times, inaccessible ethics forms themselves. For example, with respect to research involving persons with vision loss, to ensure true, and informed, consent there needs to be greater effort paid to providing information in multiple formats including regular print, large print, braille, and perhaps audio recordings. Providing information in both print and digital formats is also necessary to ensure screen reading software can be used, as necessary. There also needs to be efforts made by researchers, and supported by ethics boards, to develop consent forms that are less wordy as we know that persons with sensory impairment often find such consent forms to be overwhelming, unreadable, and too long (Watharow & Wayland, 2022).
To make the ethics process in research more inclusive, additional proactive steps can be adopted that directly involve, and enable, disabled faculty, students, and community members. One effective approach is to include persons with vision loss on ethics review boards. By having designated seats for representatives with disabilities, the boards can benefit from diverse perspectives, ensuring that research protocols are scrutinised for accessibility and inclusivity in research. This includes reviewing research methods, materials, and consent forms to ensure they are accessible and appropriate for participants with various disabilities.
Another impactful strategy pertains to appointing an equity representative with lived experience of disability and/or who specialises in CDT on ethics boards. This representative’s role would be to ensure that research proposals are evaluated with a focus on dismantling ableist views and promoting methodologies that enable, rather than exclude and marginalise. This strategy could profoundly shift research practices towards more equitable approaches that validate and respect the contributions of individuals with vision loss.
Recognising older adults in CPAR as legitimate researchers, not merely as participants, can also transform traditional research dynamics. This involves treating them as co-researchers with rights to co-author publications, participate in the design and implementation of studies, and engage in the dissemination of results. Providing specific training to enhance their research and digital skills can further reinforce their roles and contributions, aligning with a model that respects their insights and lived experiences. Furthermore, conducting regular training and workshops can play a salient role in dismantling ableist assumptions within the research community. These educational initiatives should focus on changing perceptions about risk, autonomy, and paternalism in research settings. By educating researchers and participants on identifying, and challenging, implicit biases and fostering a culture of accessibility, rather than accommodation, research design has the potential to become more inclusive and respectful of all individuals’ capabilities, contributions, and identities.
Moreover, the dollar amounts, and types of compensation, for participation in, or collaboration with, a study need to be carefully reconsidered by research ethics boards. Participants should be fairly, and adequately, compensated for their time and specialized knowledge. Community-based studies often require many hours of co-researcher’s time. When studies prioritize compensating participants and co-researchers fairly, research ethics boards may resist and thus delay timely, community-oriented research, insisting that such amounts can incentivize participation. For “marginalized” populations (i.e., communities affected broadly by adversity, including wage and employment discrimination, and the conditions of precarity and poverty), such as disabled people and/or older adults experiencing crosscutting forms of inequality, participation in research should indeed be incentivized. Uncompensated or poorly compensated participation, under any other circumstance, would be considered exploitative. As well, it seems critically pertinent to note that the dollar amount of compensation can have other serious, unexpected ethical implications for study participants and co-researchers, especially for recipients of disability- and/or age-related social assistance. For instance, some dollar amounts might significantly alter (i.e., decrease) the monthly amount of social assistance participants receive, effectively penalizing, and thus discouraging, necessary and valuable participation in research. Thus, when designing accessible, inclusive, and ethical studies, researchers working with people with disabilities and/or other populations receiving social assistance should seriously consider the amount of compensation, a potential barrier to participation if not enough or too much, and actively create workarounds that do not shortchange marginalized participants of fair compensation or their monthly income. Some workarounds might include purchasing gift cards at a store of the participant’s choosing or extending institutional resources, such as particular types of technology or software. However, a common compensation practice in research, providing gift cards, is also a contentious issue because it can “result in unfair and inadequate compensation for participants and communities” (Cheff, 2018, p. 11). As Cheff (2018) indicates, such “paternalistic” and “insulting” compensation strategies are often bound by funding and institutional restraints. It is therefore important that research ethics boards and funding agencies re-evaluate participant knowledge and contributions, enabling researchers to provide fair and meaningful compensation to variously situated participants and communities.
In addition to our suggestions for equitable research ethics practices, we recommend a set of budget considerations for funding agencies to promote accessibility and inclusion within research. Funding agencies need to allow for extra budget lines to support the provision of alternative technologies and formats, such as up-to-date screen reading software for co-researchers and/or braille documents. Funding agencies should also fund support persons to attend conferences alongside persons with vision loss as well as provide on-the-ground research support, including assistance with data collection, analysis, and management.
Conclusion
This paper aimed to unpack how the research collective, which was comprised of academic researchers, students, older adults, policy makers, and service providers, carried out accessible and inclusive CPAR with older adults with ARVL. Using meeting notes, group discussions, and reflection as the primary data collection methods, the research collective answered two primary questions including: (1) How has the research collective worked to enact an inclusive and accessible CPAR study that supports the full participation of older adults with vision loss? and (2) What has the research collective learned through reflecting on the process regarding challenges and strategies for working towards an inclusive and accessible CPAR? This was accomplished by outlining the methodological decisions made by the research collective to ensure an accessible and inclusive CPAR at four key stages in the research process including: (1) study planning stage; (2) data collection stage; (3) data analysis stage; and (4) knowledge mobilization (KMb) stage. It is our hope that by outlining the steps our research collective has taken, with respect to building inclusive research practices, that CPAR scholars can take the strategies discussed forward in future research that endeavours to be inclusive of persons with vision loss.
Footnotes
Acknowledgements
The authors would like to acknowledge the older adults with age-related vision loss who participated in this research study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the Social Sciences and Humanities Research Council Grant 435-2020-0861.