
Abstract
Asynchronous email interviewing has been increasingly utilized as an electronic method of data collection in qualitative research, because it eliminates the need for costly travel and transcription and allows more time for participants to react with thoughtful, reflective responses. While research indicates that data collected in written form is comparable in content and richness with that collected in-person, via telephone, or through virtual live interactions, there is the risk of participant attrition, loss of trust-building with subjects and missing non-verbal/visual cues for the researcher. The aim of this paper is to demonstrate use of asynchronous email interviewing as applied to a study on expectations and demands of chaplains in hospital settings. Unique in this approach is the inclusion of multiple participant groups over a large geographical area. Data were collected among chaplains, chaplain leaders, nurses, hospital executives, and patients and family members across a multi-state healthcare system. Although enrollment was adequate, 37% of those enrolled did not respond to initial interview emails, and of those who did respond, only 42% responded to follow-up questions. For several participants who did not respond to requests for email interviews, subsequent invitations to participate in live virtual interviews were preferred. Analysis reflected significant differences between groups in the quantity, quality, and richness of data, which may reflect communication patterns and preferences, time restrictions, and subject matter engagement. Based on study findings, it is suggested that similar studies offer options of interview modalities to participants to best meet their preferences and schedules.
Introduction
The use of virtual methods of interviewing for qualitative research have been utilized to bridge challenges of time and distance for participants and researchers. Use of technologies such as instant messenger and Skype were used more than a decade ago (Hinchcliffe & Gavin, 2009; Janghorban et al., 2014) and served as the foundation of technologies that advanced rapidly in response to the social distancing needs of the COVID-19 pandemic (Saarijärvi & Bratt, 2021; Thunberg & Arnell, 2022). Early research in virtual interviewing and focus groups focused on feasibility, technological challenges, and ensuring rigor with the use of alternative strategies (Illingworth, 2006; O’Connor & Madge, 2003; Palys & Atchison, 2012). With the rapid progress of technology and forced social distancing, those issues continue to exist, while new phenomena that may impact research integrity such as weariness from online teleconferencing, aka “Zoom fatigue,” are emerging (Nesher Shoshan & Wehrt, 2022; Riedl, 2022). New methods of written qualitative data collection take advantage of cloud-based technology that accommodates real-time data collection, such as synchronous question and response in a live Google Doc (Opara et al., 2023). These methods accommodate geographical and social distancing challenges; however, for those with unpredictable work schedules (e.g., healthcare workers), use of asynchronous data collection may prove valuable (Broyles et al., 2011; Hawkins, 2018).
The practical implementation of asynchronous email interviewing has not been thoroughly documented in the literature. While benefits and challenges to utilizing this technique are frequently discussed, considerations like logistics as well as the preferences and communication styles of potential participant groups have not been widely addressed. This paper describes the processes and outcomes encountered during data collection and analysis among heterogenous participant groups and is intended to help inform future efforts that utilize this method.
Asynchronous E-mail Interviewing
Asynchronous email interviewing consists of an exchange of email communication between researcher and participant which affords time flexibility, privacy, and visual anonymity ((Ratislavová & Ratislav, 2014). From the perspective of the participant, email interviewing mitigates the pressure of face-to-face exchanges, particularly when sensitive topics are at hand, presents a sense of privacy and anonymity, and enables time flexibility for participation (Amri et al., 2021; Dahlin, 2021). The participant experience with email interviewing for qualitative research has been positive and comparable to that of other modalities (Guest et al., 2020). Participants rated email communication (compared to face-to-face, online video, and online chat interviews) as convenient and a safe space to express feelings, though they felt less of a sense of rapport with the interviewer than those who communicated live and synchronously (Guest et al., 2020; Namey et al., 2020). For the researcher, challenges may arise from the inability to directly observe the participant and to note non-verbal cues; however, the lack of visual contact may eliminate any unintentional or implicit biases the researcher may impose based on participant appearance (McCoyd & Kerson, 2006).
Existing research suggests response quality and participant experience may be comparable between email interviews and other modalities, such as telephone, in-person, or live video (Guest et al., 2020; Hershberger & Kavanaugh, 2017; Keen et al., 2022; McCoyd & Kerson, 2006; Ranieri et al., 2021). Asynchronous email interviewing has benefits for both the participant and the researcher because the participant is afforded time to reflect on questions and to formulate well-thought-out and potentially data-rich responses to posed queries (Amri et al., 2021; Dahlin, 2021). Without time pressure, participants may craft their responses precisely and succinctly and/or write stream-of-consciousness, both of which may yield valuable and rich responses (Hershberger & Kavanaugh, 2017; McCoyd & Kerson, 2006). In addition, the researcher is afforded the same time allowance to reflect on responses and mindfully construct follow-up queries (Williams et al., 2012).
Additional benefits of asynchronous email data collection include expanding geographical reach because it facilitates greater feasibility and access while reducing cost for travel, eliminating the time-consuming and often expensive transcription process, producing “cleaner” data free from speech patterns and fillers (e.g. um, uh), while offering anonymity and confidentiality to participants (Amri et al., 2021; McCoyd & Kerson, 2006). Asynchronous email interviewing may be especially effective in communicating with busy working professionals, such as healthcare clinicians, whose hours may be atypical and who can respond as their schedules allow (Amri et al., 2021). Lastly, asynchronous email interviews facilitate simultaneous data collection and constant comparison of data from multiple participants at once (Amri et al., 2021; Dahlin, 2021; Keen et al., 2022).
Documented drawbacks of asynchronous email interviewing include the provision of short, superficial responses, and the inability to probe for additional information or clarification in real time. Additionally, email responses may pose a greater time commitment resulting in high potential for participant withdrawal or attrition, potential for breach of confidentiality, and inability for researchers to verify participants identity when using a non-business email address (Amri et al., 2021; Dahlin, 2021; Hawkins, 2018; Meho, 2006; Ratislavová & Ratislav, 2014). Gathering data via emails limits investigators’ ability to establish rapport and trust-building that may occur during an in-person or live exchange (Ratislavová & Ratislav, 2014) while also omitting investigators’ ability to gather non-verbal data (e.g., body language and physical cues) (Williams et al., 2012). Creating a safe, conversational, and interactive space for the researcher-as instrument to increase participant comfort through, for example, self-disclosure or affirming statements (Pezalla et al., 2012)was also forfeited through the use of asynchronous communication
Background
Hospital Chaplains
The provision of spiritual care in the hospital environment has become an integral part of patient and family care and staff well-being. Recent literature describes various dimensions of chaplains’ work including pastoral assessment, counseling, education, and emotional support of patients, families, and clinical staff (Carey, 2012; Carey & Cohen, 2009; Tartaglia et al., 2024; White et al., 2021)). Hospital chaplains receive specific training, beyond that of community clergy, that prepares them to meet the needs of patients across faith traditions (including those who do not ascribe to a specific faith or are agnostic or atheist) and to address the unique spiritual needs of those in the healthcare setting (VandeCreek & Burton, 2001). The chaplain role is perceived as largely positive by patients, families, and healthcare providers (Cunningham et al., 2017) In one study, willingness to recommend a hospital on industry-standard assessments of patient satisfaction were higher in those visited by chaplains (Marin et al., 2015). In addition, chaplains can spend up to one-third of their time providing staff support (Tartaglia et al., 2022), which is associated with positive outcomes both personally (e.g., increased compassion satisfaction) and professionally (e.g., provision of spiritual care plans) (Gaines et al., 2023; Kim et al., 2017).
While administrators recognize the value of hospital-based chaplains, there are varied perceptions of whether chaplains’ roles are essential (Flannelly et al., 2005). Administrative and organizational support of chaplains is not equivocal, as financial determinants may influence decision-making about allocation of funds for full-time staff chaplains. Research indicates that many spiritual care departments are repeatedly funded at existing levels, however, expansion of services in times of diminishing resources is unlikely (Antoine et al., 2021). It is therefore beneficial for those who advocate for additional staffing to identify the expectations of chaplains within a hospital setting, to understand the demands on their time, to determine needs that are and are not being met, and to communicate opportunities and return on investment to administration.
Chaplain Staffing
Despite the benefit of chaplain-based visitation and care provision, there is limited empirical evidence on staffing models, and most are over a decade old. A seminal study by VandeCreek (2001) was among the first to benchmark chaplain staffing schemes across hospital settings. This study found most hospitals utilize a ratio-based approach, with faith-based community hospitals demonstrating a mean of 2.90 chaplains per 100 patients and a mean of 1.22 in non-faith-based community hospitals (VandeCreek et al., 2001). A recent study reports a mean of 2.5 chaplains per 100 average daily census (Tartaglia et al., 2024). However, there has been criticism of ratio-based staffing, and there is a call to leverage a broader approach that includes identifying priorities, activities to meet those priorities, a business plan, and a cost–benefit analysis as components of a comprehensive staffing model (Wintz & Handzo, 2005). Some suggest referral- and acuity-based models of chaplain staffing as alternatives to ratio-based models (Newberry, 2009; Stoddard, 1993). The Association of Professional Chaplains endorses an approach that considers the needs of individual organizations and quality-based, rather than quantity-based, chaplain staffing (Association of Professional Chaplains, 2009). For those who wish to retain and potentially expand chaplaincy offerings, there is a need to demonstrate return on investment, including estimating cost per unit-of-service and identifying supply and demand imbalances (Victor, 2009). Thus, organizations must identify an appropriate approach to staffing to meet the needs of patients and staff.
Current Study
This paper describes the practical application of asynchronous email data collection, including the recruitment and data collection processes from a heterogenous sample of participants within a nine-state, 52-hospital faith-based healthcare system. While asynchronous interviewing is often leveraged to access groups that are difficult to engage due to sensitivity of the topic or participants’ social status (Ratislavová & Ratislav, 2014), this study utilized the method to access various populations across a large geographical area. Through asynchronous email interviews, this study sought to examine the perspectives of various relevant parties on expectations, demands, and experiences of interactions with chaplains. These data are intended to identify met and unmet needs of current staffing and eventually to help inform recommendations for future chaplain staffing. Logistical considerations of asynchronous interviewing and variability in the quality and richness of data collected based on sample characteristics are discussed.
Methods and Process
Sampling
To gather perspectives from relevant parties who may have understanding of the roles of chaplains, insight into their job expectations and demands, and/or personal experiences with chaplain interaction, interviews were sought with chaplains, leaders in the spiritual care department, educators in Clinical Pastoral Education (CPE), hospital administrators including Chief Executive Officers (CEOs) and Chief Financial Officers (CFOs), acute care nurses, and patients and/or family members of patients with recent care received from a system hospital (on or after January 1, 2021) within a healthcare system headquartered in Florida. A convenience sample from each group was recruited, with snowball recruitment encouraged. It suggested that saturation of data may be achieved when between 5 and 35 interviews are conducted (Guest et al., 2006) and for the purposes of collecting data from homogenous groups, a sample size of between 5–10 in each category of participant was sought (Hennink & Kaiser, 2022; Saunders et al., 2018)
Recruitment Strategies
Obtaining perspectives from a diverse population requires a multipronged approach. Recruitment efforts for employees utilized organizational charts and distribution lists from 52 different hospital campuses to identify potential participants. Internal distribution lists were used to contact chaplains (n = 39), chaplain leadership (n = 22), CEOs (n = 33), and CFOs (n = 29) via email. Nursing email distribution lists were unavailable, so chaplains were asked to forward emails to nurse leaders on the units on which they serve that included a study invitation and flyer.
As there were 94 chaplains within the organization as potential participants, it was deemed most appropriate to invite a representative sample based on location to moderate sample size. Chaplains were grouped by hospital, and random representatives from each location were selected to receive an invitation. As there was low enrollment from the initial invitation (n = 23), a second invitation (n = 16) was sent to a second set of representative chaplains two weeks after the first. Because other groups of employees (chaplain leaders, C-suite executives, etc.) were smaller, all potential participants received invitations.
Patient and family recruitment required a different strategy. Due to inconsistent documentation of chaplain visits in the electronic health record (EHR) for proactive visits that did not involve a formal consultation request, it was determined that the selection of patients via EHR would be an ineffective strategy. In addition, training and regulatory requirements for access to patient private health information (PHI) would have slowed enrollment and data collection. Instead, connecting with potential patient and family member participants was achieved via presentations to Patient and Family Engagement Councils (PFEC), voluntary groups composed of current and former patients and family members who provide feedback to the organization about improvement opportunities. Through leadership in the organization’s patient experience department, facilitators of the PFECs were contacted with a request for a five-minute allocation of time to present to the membership. PFECs from six hospitals received virtual presentations via Microsoft Teams, including a Microsoft PowerPoint overview of the study expectations and protections. Attendees at the PFEC presentations were emailed study flyers and asked to share them with other potential participants.
To enroll, all potential participants followed a link or scanned a QR code that led to an electronic informed consent document hosted in REDCap (Research Electronic Data Capture) (Harris et al., 2009, 2019). Initial invitations to participate were emailed to chaplains, chaplain leaders, educators, and C-suite executives in January 2023 and enrollment took place from January-June 2023. Recruitment of nurses was ongoing during this period, because contact was contingent on chaplains forwarding the invitation to participate. Active recruitment of patients and family members through presentations to PFECs took place from March-June, 2023.
Data Collection
After consent was obtained electronically, basic demographic information was collected via REDCap, a secure web-based application for data management and survey distribution. Participants were asked to provide a preferred email address that would serve as the direct communication for asynchronous interviews. Separate interview guides, available in Supplemental Material, were developed for each group of participants. Interview questions were based on a review of the literature and edited to align with the research aim of the study. Participants were asked to provide substantive responses, with emailed instructions including a request to “respond to each question as if you were being interviewed about the topic. We want to know your thoughts and opinions, so the more you can expand on your answers, the better”.
The principal investigator emailed interview questions on an ongoing basis within two business days of enrollment, with responses requested within five business days. Because only 33% (28/86) of responses were received within the initial 5 days, the initial response period was extended to 10 days, with a reminder prompt after five days and another five business days to respond. Due to a lack of response to initial and reminder emails, the study team elected to offer enrolled participants the option to take part in a virtual recorded interview instead of an email interview. An email offering the virtual interview option was sent to participants who had not responded to reminder emails, resulting in eight virtual semi-structured interviews. Figure 1 details enrollment and Tables 1 and 2 present demographic descriptions of enrolled participants and study participation by group. Follow-up questions asking for more details, stories, and/or clarification were sent to 40 participants after receipt of initial responses. These questions were crafted by consensus of investigators and involved an iterative process of confirming emerging themes among participants. Of those who received follow-up questions, 42% (n = 17) responded with further data. Enrollment for participants in asynchronous email study of perceptions of hospital chaplains. Demographics of Enrolled Participants. Participation by Group.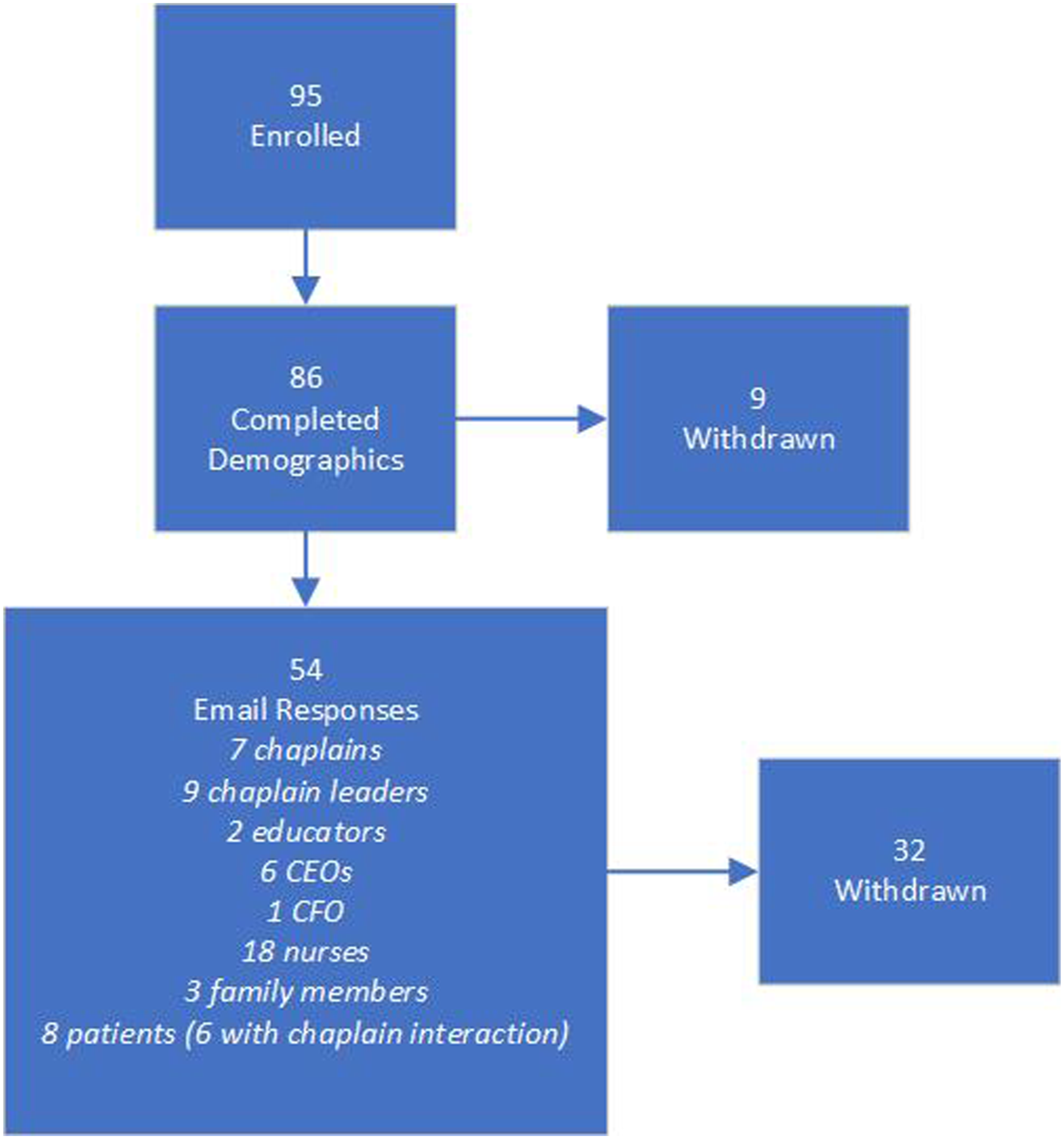


Eight participants elected to engage in live, recorded Microsoft Teams interviews in lieu of email interviews: three CEOs, two chaplains, one chaplain leader, one nurse, and one CPE educator. Interviews lasted between 16 and 46 minutes, with an average duration of 30 minutes. There were distinctions in the duration of the interviews based on profession; the nurse interview was the shortest in duration at 16 minutes, the CEO interviews averaged 22 minutes, and the chaplain/chaplain leader/educator interviews were longer, averaging over 39 minutes.
Ethics and Privacy
The study and all study procedures were approved by the organization’s Institutional Review Board and all participants were consented electronically prior to participation in any study-related activities. Data entered via REDCap were downloaded and participant IDs were assigned with only study team access to the identification key. The only identifiable data collected were preferred email address. All participants had the option to use personal email addresses and to respond from personal devices. Email responses from participants were received by the principal investigator, de-identified, assigned a study ID, saved to a private shared drive accessible to the study team and deleted from the email server. All interview recordings were moved to a private drive, deleted from the Microsoft Teams app, and made inaccessible to anyone outside the study team.
Study Process
The study investigators independently reviewed the emailed responses and noted comments and questions in shared documents. The study team met weekly via Microsoft Teams to review responses line-by-line, discuss emerging themes, and collectively craft follow-up questions to be returned to participants to elicit further data. Responses to follow-up questions and transcripts of video interviews were similarly reviewed.
Once data collection was complete, all responses (including follow-up responses) were rated excellent, good, and poor based on consensus of the study team on the ability of data to be analyzed (i.e., could data be coded, did responses address the questions asked, was there thought/time invested). Those who responded with excellent or good responses were offered the opportunity to claim the $30 participation incentive. All participants were made aware of the parameters for earning the incentive in the informed consent document, and that payment would be at the discretion of the research team.
Data Quantity and Quality
Data Quantity and Quality Between Groups
Mean Word Counts of Initial Email Responses by Group.

Despite garnering the greatest number of participants, nurse participants generally provided responses that were worded succinctly and with little depth. While some nurses responded using complete sentences, many utilized brief phrases and incomplete thoughts that may have reflected a lack of time and/or engagement. This may be attributable to a style of writing consistent with documentation in the electronic health record. Documentation requires clear, concise communication to accurately relay critical patient-centered information, with implications for quality of care, reimbursement, and legal requirements (Blair & Smith, 2012; Jefferies et al., 2012). In addition, it has been noted by journal editors and educators that many direct care nurses who are not regularly engaged in academic pursuits may be deficient in publication-appropriate writing skills (Johnson & Rulo, 2019). Narrative writing skills are not required in their daily jobs, whereas brevity and clarity are, so nurses who participated in this study may have defaulted to health record-style writing. In addition, work emails were utilized for correspondence, so responses may have been rushed and completed during short breaks in the workday, thus negating the convenience and time flexibility benefits of asynchronous interviewing.
Chief executives, including CEOs and the one participating CFO, also provided concise responses, however; the responses were focused and well-written. Executive written communication typically takes into consideration the need for lack of ambiguity and requires diligence as there is no opportunity to add additional context or to address questions (Biggs et al., 2023). In this study, half of the CEOs opted to engage in live video interviews in lieu of writing responses via email. For many in leadership roles, taking the time to craft written responses and the “think time” required to do so is at a premium, and personal engagement is more time-efficient and comfortable (Biggs et al., 2023; Rogers, 2012).
Patients and family members were forthcoming, albeit generally brief, with information about encounters with chaplains (for those who interacted with chaplains) or expectations for encounters (for those who did not interact with chaplains). The dearth of more personal narratives of spiritual encounters may be due to the lack of rapport built with participants by the researchers due to the impersonal nature of email communication and the formal nature of research-based correspondence (Dahlin, 2021). In addition, the nature of the questions themselves may not have been explanatory enough to prompt unconstrained responses and ultimately rich, thick descriptions within the data (Meho, 2006).
Chaplains and chaplain leaders provided rich and robust responses regarding their role and its potential impact. By the very nature of their jobs, chaplains are communicators tasked with listening to complex needs, responding through carefully chosen words, and often serving as communication liaisons between patients, families, and staff (Klitzman et al., 2022). Chaplains integrate descriptive writing into their daily electronic health record documentation and are responsible for clear communication of care to the multidisciplinary team (Association for Clinical Pastoral Education, 2015; Lee et al., 2017). Chaplain training and education (Clinical Pastoral Education) is grounded in self-reflection to connect with others who are suffering (Cadge et al., 2019; Vanderstelt et al., 2023). For chaplains, this is often manifested through storytelling and narratives, which involves telling personal stories to demonstrate vulnerability and relatability (Vanderstelt et al., 2023). In addition, interviewing is a methodology often leveraged by chaplains in patient encounters, suggesting that chaplains may make intuitive qualitative researchers (Grossoehme, 2014).
It should be noted the more a topic holds personal importance, the more likely it is to garner a rich response from an interviewee (Ogden & Cornwell, 2010). It is expected that chaplains and chaplain leaders provided deeper responses due to the topic’s personal importance than for those who have professional ties to it rather than personal ones.
Data Quality Between Platforms
Oates and colleagues (2022) conducted an extensive assessment of the quality, duration, content, and user experience between several modalities of qualitative interviewing, including email and video, and found no substantive differences between them. In this study, the data procured from live (video) interviews provided more in-depth content and prolonged engagement from participants than email interviewing (Oates et al., 2022). Although data analysis is ongoing, codes and themes between the two modalities are similar; it is the duration and descriptiveness that differ (Oates et al., 2022).
Previous research indicates that more sensitive and personal content may be elicited via email interviewing due to the comfort and anonymity afforded by the platform (Dowling, 2012). The discrepancy between this trend and the current study patterns may be due to the non-controversial and non-intimate subject matter. Except for patients/families, the content of the interviews was about perceptions and expectations within a professional setting rather than about sensitive personal experiences. Thus, the nature of the data and engagement were relatively impersonal.
In terms of user preference, those who engaged in video interviews cited time commitment and comfort in expressing opinions verbally rather than in writing. One CEO (CEO4) stated, “So I appreciate you moving over to [Microsoft] Teams for me because I wasn't getting it done in written form and I think overall this was a better experience for me,” and a chaplain leader (CL11) stated, “I have to admit that when you send these questions over, I felt like I needed to talk it out. So this is a perfect way for me.”
Discussion
Time and Effort
The logistics of data collection across such a large sample via email proved to be time intensive. Enrollment lasted six months (January-June 2023). Each enrolled participant received a personalized welcome email with survey questions, a follow-up/reminder email for those who did not respond, an email offering video interviewing in lieu of email for those who did not respond to the reminder emails, and finally withdrawal emails for participants who did not engage. Lags in response time, need for follow-up and potential to drop out are all potential disadvantages of email as an interviewing method (Bowden & Galindo-Gonzalez, 2015). It was determined that the principal investigator, rather than a research coordinator, should maintain all email communication to maintain consistency and establish trust and rapport with participants (Hawkins, 2018). Timing and tracking of enrollment, participation, reminders, and status were maintained by the principal investigator. The most active day of enrollment – the first day invitation emails were sent (a Friday morning) included emails sent to eight participants from three participant groups (chaplains, chaplain leaders, and nurses). Emails with follow-up questions were sent in batches of 4–8 emails on a weekly basis after the study team review meetings. It has been noted that the time and effort required to maintain correspondence with multiple participants simultaneously and to properly respond to each is substantial (Fritz & Vandermause, 2018)
While transcription of live interviews is typically a time and cost deterrent (Meho, 2006), the transcription function in the videoconferencing software created a baseline transcript that was reviewed and corrected for accuracy by a study coordinator. Use of videoconferencing-based transcription function can greatly impact the efficiency of the research process (Keen et al., 2022) although some researchers prefer manual transcription to facilitate familiarization with the data and to ensure rigor ((Archibald et al., 2019; Khan & MacEachen, 2022). To ensure accuracy, the transcripts in this study were then reviewed independently by the members of the research team, and weekly meetings involved writing and sending follow-up emails with clarifying questions and probes. Those then required follow-up emails for non-responders.
Compared to live interviews, which are discrete events, asynchronous email interviews require a more significant overall time commitment due to ongoing analysis, probing, correspondence, and follow-up. While some research indicates asynchronous email interviewing is the most cost-effective in terms of travel expenses and transcription, logistics and multi-part analysis time have not been considered (Namey et al., 2020).
Scientific Rigor
It was crucial to integrate strategies into study methods to ensure the trustworthiness of findings, therefore techniques to establish credibility, dependability, transferability, and confirmability were considered throughout the study (Forero et al., 2018; Lincoln & Guba, 1985). While face-to-face and virtual interviews provide the opportunity to cultivate relationships that foster trust, prolonged engagement, and persistent observation, it was necessary to reframe engagement and observation when considering the asynchronous aspect of email interviews (Hawkins, 2018; Morse, 2015). Engagement and observation were distinguished by the richness and depth of interview responses that revealed the context of the participant’s experiences with a chaplain in the hospital setting. Many participants further described whether their personal spiritual and/or religious experiences influenced their perceptions and expectations of chaplain interactions, thus providing investigators with deeper insight into participants’ interpretations of their experiences. Investigators’ follow-up probes provided an opportunity to either clarify or gather more comprehensive details to fully capture participants’ experiences.
Triangulation of email interview responses with virtual interview transcripts provided an opportunity to examine two different data sources gathered from participants with multiple viewpoints, from chaplains to those they serve and reflecting a wide range of perspectives from small, rural community hospitals to larger, urban tertiary care centers. Additionally, analyst triangulation enhanced data analysis through multiple perspectives and a wide-ranging lens to illuminate the potential blind spots of each investigator. Furthermore, peer debriefing was conducted with academic peers for objective insight into study findings. Lastly, and most importantly, member checking was conducted with chaplains, chaplain leaders, C-suite leaders, and nurses to ascertain whether overarching themes reflected an accurate depiction of the experiences of their peers.
Transferability relies on thick and rich descriptions garnered from co-created participant and researcher data (Lincoln & Guba, 1985). As previously mentioned, thick description was less robust from certain groups of participants during asynchronous email interviews, likely due to the written professional communication styles among hospital leaders and nurses (Blair & Smith, 2012; Johnson & Rulo, 2019; Rogers, 2012). On the other hand, chaplains contributed rich, thick descriptions of their roles, expectations, and aspirations for hospital-based chaplains. Chaplain communication styles require openness and vulnerability to foster a therapeutic alliance with individuals suffering from spiritual distress (Mascaro et al., 2022).
Asynchronous email interviews allowed for timely audit trails related to analytical decisions throughout the study to establish confirmability and dependability, often with the opportunity to perform constant comparisons across multiple interview transcripts in a single session. This fostered the ability to identify patterns in the data to inform follow-up questions among multiple participants to enhance the ability to probe for additional perspectives about emerging themes.
Challenges and Risks
Anticipated recruitment challenges within an extensive hospital system that spans the United States were a key inspiration behind the asynchronous email interview approach. The study team met frequently to discuss enrollment in order to brainstorm strategies to increase enrollment among specific cohorts. Patient and family participants proved to be the most challenging to recruit as electronic health record documentation may not reflect whether a patient or their loved one engaged with a chaplain during their hospital stay. Therefore, it was necessary to seek permission to engage with patient and family advisory committee members to facilitate connections with patients and/or their families for study recruitment.
Another challenge encountered was obtaining responses to the investigators’ follow-up questions, often leading to reliance on the initial email interview response as the final transcript. Study participants were offered $30 stipends for complete responses, thus prompting investigators to explore and define a complete response that reflected prolonged engagement in the asynchronous email interview and subsequently providing those participants a stipend.
Confidentiality may have been a concern for participants who consented but did not respond to the initial email interview questions. While the topic was not necessarily sensitive, employee participants who experienced negative perceptions of chaplains may have been reluctant to share these perceptions within their faith-based organization. Additionally, technology limitations may have impacted patient and/or family participation if they lacked computer access for email interview responses.
Variations in data quality were a concern, particularly between groups and among individual participants. Causes of variations in quality may include everything from distracted participants who are multi-tasking when responding to misinterpretation of investigator prompts (Amri et al., 2021; Vicsek, 2016). Data quality, particularly among some of the nurse participants, was unable to be analyzed due to brevity. It is possible that perceived lack of engagement on the part of the researchers due to the method of communication may have elicited a similar lack of engagement from participants (Amri et al., 2021). Further explanation of the purpose of the research and more robust questions that ask for specific stories and accounts may have attracted more responses from busy professionals with competing priorities (Coyne et al., 2016).
Lessons Learned
Leveraging asynchronous email interviewing as a method to elicit responses among diverse participant groups across a large geographical area is an effective strategy to minimize costs (i.e., travel, transcription). However, some challenges have not been well-documented in the literature, such as the logistical time required to track and engage a larger number of participants fully. Communication with multiple participant populations and seeking data saturation among each group exponentially increased the time involved for the researchers, creating one large qualitative study out of several smaller studies. It is recommended that email interviews be limited to 2–3 concurrently (Fritz & Vandermause, 2018); however, the size and scope of this study necessitated simultaneous correspondence with up to 15 participants at once. The time, effort, and cost avoided in transcribing interviews were substantial (Hawkins, 2018), but a portion of that was reallocated to study coordination and follow-up with participants.
Despite the time and effort invested into crafting and sending follow-up emails, attrition was high after the first email exchange (Bowden & Galindo-Gonzalez, 2015), with responses received from less than half of those who received follow-up questions. The study may have benefited from offering alternative platforms for virtual interviews or focus groups from the beginning, as providing options may have better-accommodated scheduling, competing responsibilities, and comfort (Keen et al., 2022). In addition, the nature of the topic may have lent itself to live engagement, because the use of vignettes and storytelling are often effective in engaging clinical staff with qualitative research (Murphy et al., 2021). Asynchronous email interviews are often beneficial in research with marginalized populations about sensitive topics (Cook, 2012; Keen et al., 2022); however, the relatively non-controversial topic of chaplain responsibilities in professional settings – to all but patients and family members – could have better lent itself to live follow-up prompts that elicited personal stories and substantive data.
Utilizing workplace email addresses while facilitating recruitment more easily, may have introduced some challenges with data quality. In nurses, especially, engagement during work hours using work email placed time pressure on the interaction and likely resulted in abbreviated responses. Nurses may view research as a distraction from their clinical duties, and research that does not directly impact their practice may be deemed low priority (Coyne et al., 2016). The benefits of using workplace email includes the ability to verify the identity and job role of the participant (Amri et al., 2021); however, encouraging participants to utilize personal email addresses may have fostered the perception of privacy and eliminated competing professional priorities.
Conclusion
Gathering qualitative data from multiple relevant parties across a large, multi-state healthcare organization required an innovative approach that would be feasible, cost-effective, and rigorous. Input into chaplain roles within a healthcare system requires the perspectives of decision-makers, care recipients, as well as the chaplains themselves. Asynchronous email interviews with these groups – chaplains, chaplain leaders, nurses, C-suite executives, patients, and families - produced inconsistent results in terms of data quantity and quality, with marked variations between groups. Initial recruitment was successful, but prolonged engagement via email communication suffered, perhaps from an absence of rapport or personal connection to the subject matter. Utilizing asynchronous email interviewing alone is best suited for studies that require smaller sample sizes and seek to explore a specific phenomenon or experience. For larger, more exploratory studies, a hybrid approach of offering email exchanges or interview and focus group opportunities accommodates the challenge of spanning geographical distance while offering options to best suit the preferences of the participants.
Supplemental Material
Supplemental Material - Utilizing Asynchronous Email Interviewing for Qualitative Research Among Multiple Participant Groups: Perspectives on Met and Unmet Needs From Chaplain Staffing
Supplemental Material for Utilizing Asynchronous Email Interviewing for Qualitative Research Among Multiple Participant Groups: Perspectives on Met and Unmet Needs From Chaplain Staffing by Stephanie L. Harris, Martin Shaw, and Jeanette F. Green in International Journal of Qualitative Methods.
Footnotes
Acknowledgments
The authors would like to acknowledge Dr. Patricia Robinson for her leadership and support, the Wholeness Institute at Advent Health, and the participants who donated their time and insights to this study.
Author Contributions
All authors contributed to the analysis of data and drafting and approving the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.